


Abstract
Objectives: To investigate the cytotoxic effect of anastrozole on breast (MCF7), liver hepatocellular (HepG2), and prostate (PC3) cancer cells.
Methods: This is a prospective study. Anastrozole’s mechanism of apoptosis in living cells was also determined by high content screening (HCS) assay. Methylthiazol tetrazolium (MTT) assay was carried out at the Centre of Biotechnology Research’s, Al-Nahrain University, Baghdad, Iraq between July 2015 and October 2015. The HCS assay was performed at the Centre for Natural Product Research and Drug Discovery, Department of Pharmacology, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia between November 2015 and February 2016.
Results: The most significant cytotoxic effect of anastrozole towards 3 cancer cell lines was obtained when its concentration was 400 µg/mL. The MCF7 cells were more sensitive to anastrozole compared with the HepG2 and PC-3 cells. There was a significant increase in membrane permeability, cytochrome c and nuclear intensity when anastrozole (200 µg/mL) was used compared with doxorubicin (20 µg/mL) as a standard. Also, there was a significant decrease in cell viability and mitochondrial membrane permeability when anastrozole (200 µg/mL) was used compared with positive control.
Conclusion: Anastrozole showed cytotoxic effects against the MCF7, HepG2, and PC3 cell lines as determined in-vitro by the MTT assay. The HCS technique also showed toxic effect towards MCF7. It is evident that anastrozole inhibits the aromatase enzyme preventing the aromatization mechanism; however, it has a toxic effect.
Aromatase inhibitors play an important role in estrogen receptor (ER)-positive breast cancer therapy in postmenopausal women.1 The inhibitor suppresses the activity of aromatase enzymes, which is responsible for the production of estrogen from androgens under normal circumstances. There are 2 main types of aromatase inhibitors, which are known to block aromatase action, which consequently results in a reduced estrogen production.2 The first type produces a permanent bond with the aromatase enzyme, which leads to permanent inactivation of the enzyme.3 This type is known as an irreversible steroidal inhibitors. The second type is referred to as a non-steroidal inhibitors (for example, anastrozole).2 They inhibit estrogen synthesis through reversible aromatase enzyme competition.3 They also inhibit the production of estrogen through reversible binding to the aromatase enzyme heme-iron component.4 Aromatase inhibitors are well tolerated by patients and additionally are highly selective for the aromatase enzyme. They are an effective second-line therapy since its mode of action is different from first line treatment options such as tamoxifen which blocks estrogen activity at the receptor level.4 Research shows that anastrozole among other drugs can be used effectively after surgery in hormone-dependent advanced breast cancer patients.5,6 Cancer is caused by irregular and uncontrolled growth of cells, which leads to the destruction of tissue.7 It is expected that the number of new cancer patients to be approximately 14 million by 2030.8,9 New anticancer drugs do not directly target the DNA biosynthesis, but mainly affect the signals, which regulate the cell cycle.7 Necrosis is a degradation process, which leads to the death of tumors cells.10 This passive reaction could be fatal and is highly influenced by external factors outside the cell such as toxins, infections and/or trauma.10 In contrast, apoptosis is a programmed cell death due to cell morphology changes.11 Cell shrinkage, messenger RNA decay and DNA fragmentation are the most common changes within cell morphology due to apoptosis.11 It has been estimated that the number of cells, which undergo apoptosis in one day within a child (8-14 years old) is approximately 20-30 billion.12 Various techniques can be used to treat cancer which includes surgery,13,14 radiation,15 and chemotherapy.16 Although, surgery and radiation are effective at killing cancer cells, they can also lead to the destruction of healthy cells and organs.17 In addition, chemotherapy can lead to intolerable side effects and is not an efficient treatment for cancer when used alone. Recently, we reported the effect of anastrozole levels on estradiol in women with postmenopausal breast cancer. Strong positive correlations were found between serum aromatase and estradiol (r = 0.79-0.82).18 We have also investigated the effect of aryl phosphonate derivatives on human breast cancer cells (MCF7) and liver carcinoma cell line (HepG2).19 The MCF7 cancer cell line is a very sensitive to estrogen receptor and can be used as a model to investigate the response of the hormone.20,21 In this stuedy, we report the cytotoxic effect of anastrozole against MCF7, HepG2 and prostate (PC3) cancer cells.
Methods
Ethical approval
Ethical approval was obtained from the College of Applied Medical Sciences Ethics Committee, King Saud University, Riyadh, Kingdom of Saudi Arabia.
Cell culture
The MCF7 cancer cell line was purchased from American Type Culture Collection (ATCC, Manassas, VA, USA). The HepG2 and PC3 cell lines were provided by the Centre of Biotechnology Research, Al-Nahrain University, Baghdad, Iraq. The MCF7, HepG2 and PC3 cells were allowed to grow in Dulbeccos modified Eagle medium (Life Technologies, Inc, Rockville, MD, USA) supplemented with 10% heat-inactivated fetal bovine serum (Sigma-Aldrich, St. Louis, MO, USA), glutamine (2 mM), penicillin (1%), and streptomycin.
Biological activity
Methylthiazol tetrazolium (MTT) assay was carried out at the Centre of Biotechnology Research’s, Al-Nahrain University between July 2015 and October 2015. The high-content screening (HCS) assay was performed at the Centre for Natural Product Research and Drug Discovery, Department of Pharmacology, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia between November 2015 to February 2016. The MMT and HCS assays were carried out based on standard procedures.22,23
Cytotoxicity assay (MTT assay)
The MTT assay was carried out on MCF7, HepG2, and PC3 to determine the anticancer activity of anastrozole. Anastrozole was dissolved in Dimethylsulfoxide (DMSO) to produce the stock solution. Doxorubicin was used as a control in each plate and incubated. After removing the media, the obtained formazan crystals were stabilized by the addition of DMSO. The absorbance was measured (570 nm) using a Hidex Chameleon plate reader and the growth inhibition was calculated. The kit used contains Hidex Chamelon plate reader with a 570 nm filter, 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT; 10 × 5 mg), multi-channel pipette (8 to 12 channel), pipette tips (10-100 µL), phosphate-buffered saline (PBS), sterile HCl, DMSO; 0.01 M and CO2 incubator (5%).
Preparation instructions
The stock solution was prepared by dissolving anastrozole in DMSO and serial dilutions were made (25–400 µg/mL). The stock solution (100 µL) was added the MCF7, HepG2, and PC3 cancer cells cultures. In each plate, doxorubicin was included as control. After 24 hours in CO2 incubator, MTT (5 µg/mL) was added to each well and the plates were incubated in CO2 incubator for 1-4 hours. The media was removed and DMSO was added into each well to solubilize the formazan crystals. The absorbance was measured (wavelength = 570 nm) using a micro plate reader.
High-content screening (HCS; cytotoxicity 3 Kit)23
Thermo Scientific Cellomics Multi parameter cytotoxicity 3 Kit (Thermo Scientific, Japan) was used to enable simultaneous measurement of cell permeability, cell count, nuclear intensity, mitochondrial membrane potential, and cytochrome c level for the MCF7 cell line. The kit used contains cytochrome c (primary antibody), DyLight™ 649 conjugated goat anti-mouse IgG. It also contains mitochondrial membrane potential, permeability and Hoechst dyes along thin plate seal assembly. Wash buffer (10X Dulbecco’s PBS), permeabilization buffer (10X Dulbecco’s PBS with 1% Triton® X-100), and blocking buffer (10X) were used. The kit enables measurements of several cell parameters at the same time. The distribution and intensity of fluorescence within cell line (N=5) was imaged with HCS system (Thermo Scientific). The HCS system was attached to a computerized imaging microscope equipped with Zeiss 40X (0.75 NA) Plan-Neofluar objective lens. The cells were treated for anastrozole for 24 hours followed by the addition of Mitochondrial membrane potential (MMP) and the cell permeability dyes and then incubated 37°C for 30 min. The cells were fixed and permeabilized using a standard procedures.23
Hoechst 33342 staining assay
The Hoechst 33342 staining assay was used to study the nuclear morphology of the MCF7 cells. Six-well plates were used to culture the MCF7 cells for 24 hours. Zeiss Axio Observer microscope (Thermo Scientific) was used to investigate the changes in MCF7 cells nuclear morphology.
Results
Cytotoxic effect of anastrozole on cancer cell lines, in-vitro study using MTT assay
The cytotoxic effect of the anastrozole was determined within 3 cell lines as MCF7, HepG2, and PC3. The analyses were carried out using MTT method.23 Various concentration (25−400 µg/mL) of anastrozole were tested used along with doxorubicin (20 µM) as a standard. The results obtained along with least significant differences (LSD) are shown in Table 1. The high anastrozole concentration (400 µg/mL) showed the most significant cytotoxic toward all cell lines treated for 24 hours.
The cytotoxicity effect of anastrozole on the MCF7, HepG2 and PC3 tumor cell lines (N = 5).
The inhibition rate of MCF7 cells after 24 hours of incubation was 84.0 for doxorubicin (standard). The viability values was 58.4 when anastrozole concentrations was (400) 30.9 (200), 22.5 (100), 8.9 (50), and 7.7 (25) µg/mL. The results indicated that 24 hours after the administration of anastrozole to MCF7 cells, viability was 69.5% when anastrozole (400 µg/mL) was used. The inhibition rate of HepG2 cells after administration of standard for 24 hours was 77.79 compared with 41.7 when anastrozole was 400 µg/mL with a viability of 53.6% when anastrozole concentration was 400 µg/mL compared with standard. For PC3 cells, the viability was 37.6% compared with that obtained for the standard. The differences between the standard and all experimental groups were statistically significant (p<0.05).
High content screening and analysis
Cell permeability, cell count, nuclear intensity, mitochondrial membrane potential, and cytochrome c level was measured to detect the apoptosis changes during 24 hours exposure. Various anastrozole concentrations on MCF7 cell line were used along with the standard. The results obtained are shown in Figures 1-5. The differences between standard and all experimental groups were statistically significant (p<0.05).
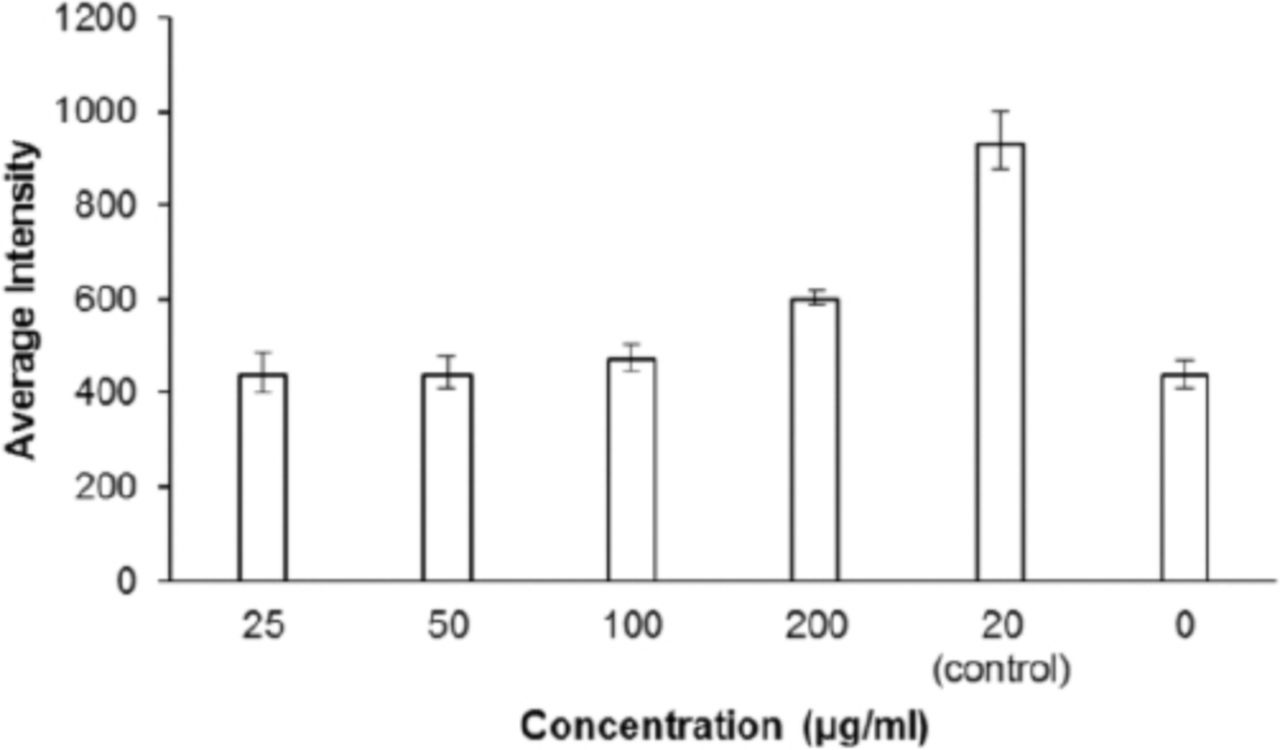
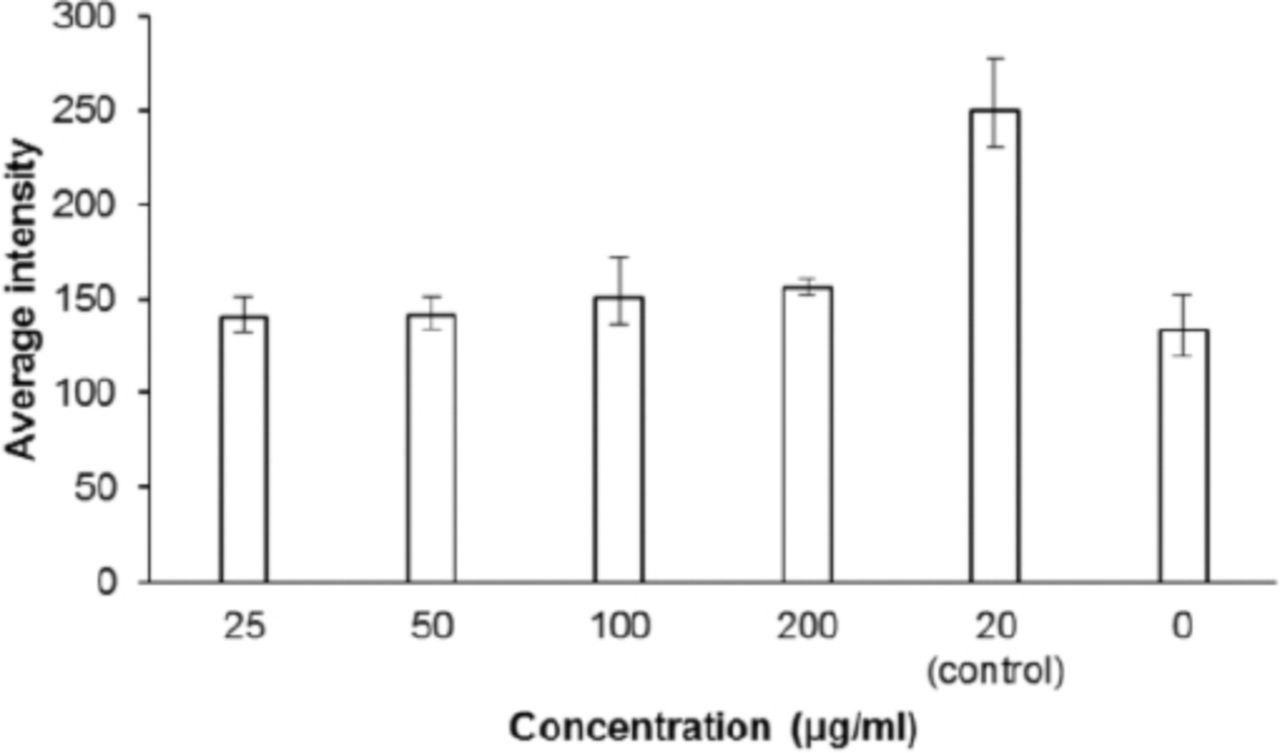
Effect of anastrozole on the nuclear intensity in human breast cancer cells line (n=5); p=0.0243 for anastrozole (200 µg/mL); p<0.0001 for control (20 µg/mL).
Effect of anastrozole on the cell membrane permeability human breast cancer cells line (n=5); p=0.012 for control (20 µg/mL).

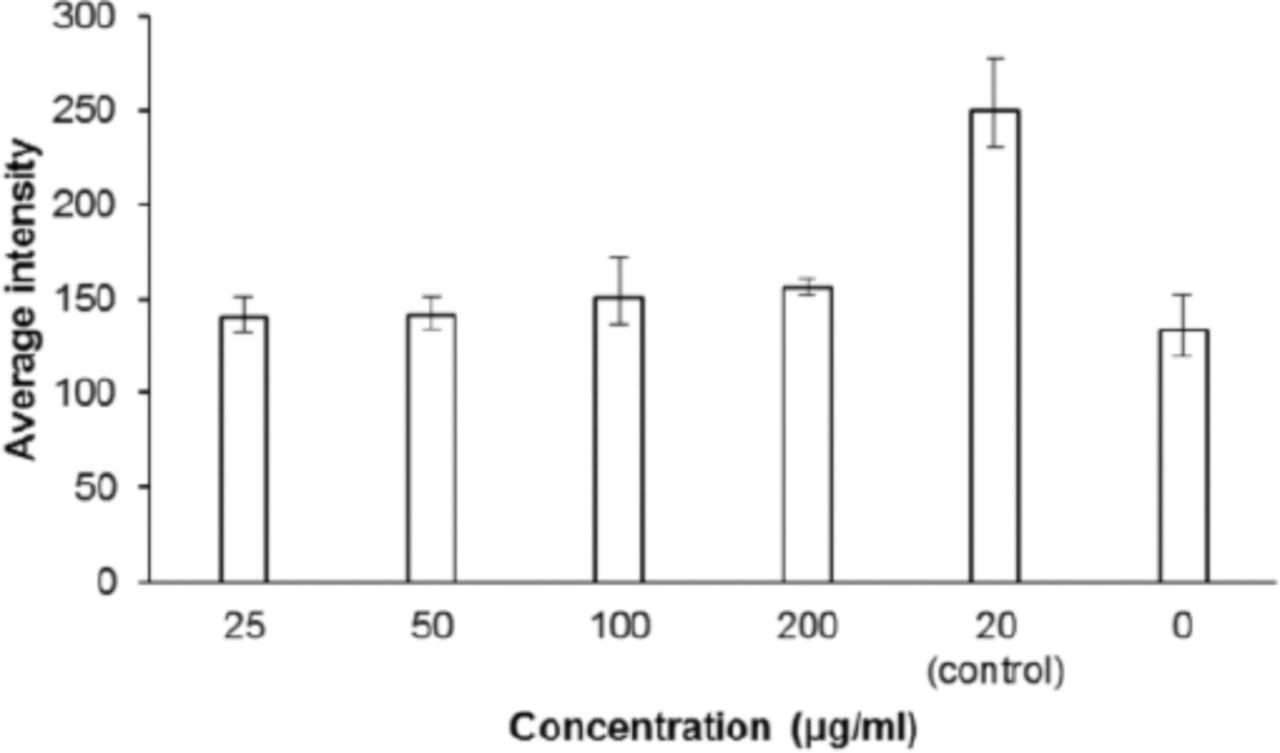
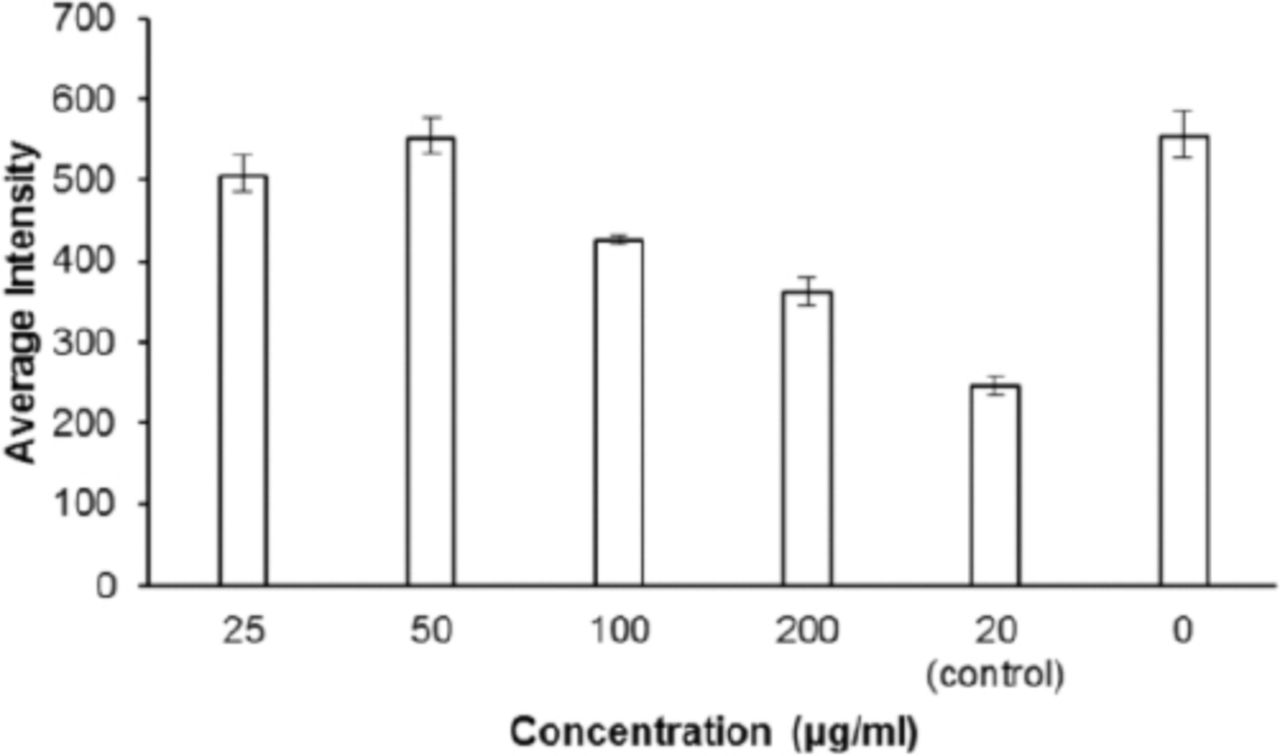
Effect of anastrozole on the mitochondrial membrane permeability in human breast cancer cells line (n=5); p=0.0026 for anastrozole (200 µg/mL); p=0.0002 for anastrozole (100 µg/mL); p<0.0001 for control (20 µg/mL).

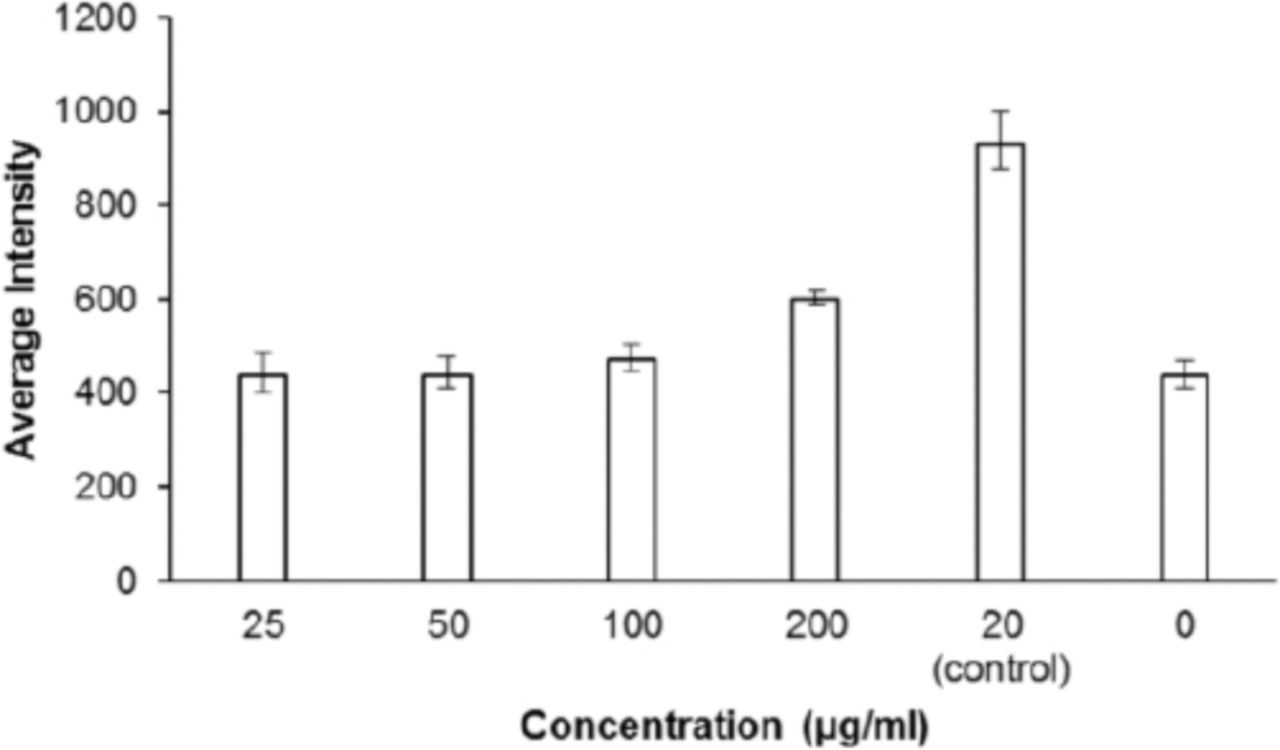
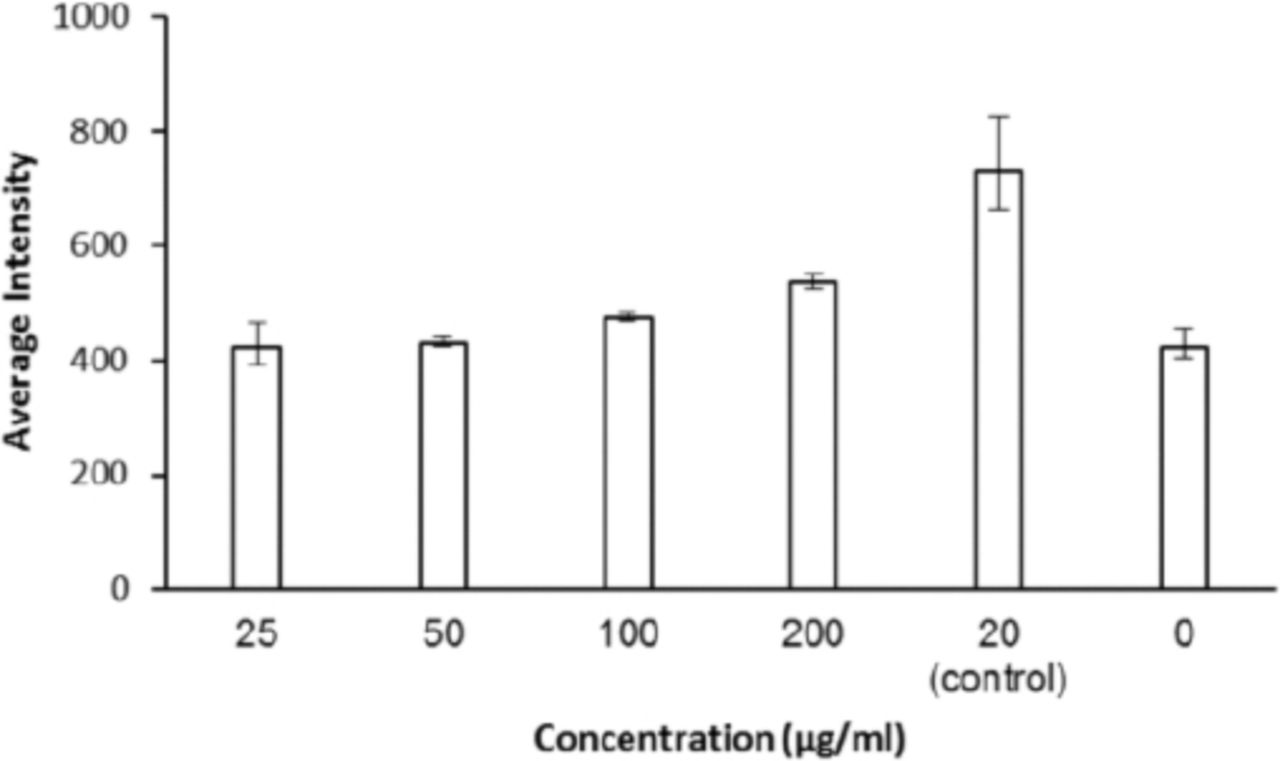
Effect of anastrozole on cytochrome c in human breast cancer cells line (n=5); p=0.0009 for control (20 µg/mL).
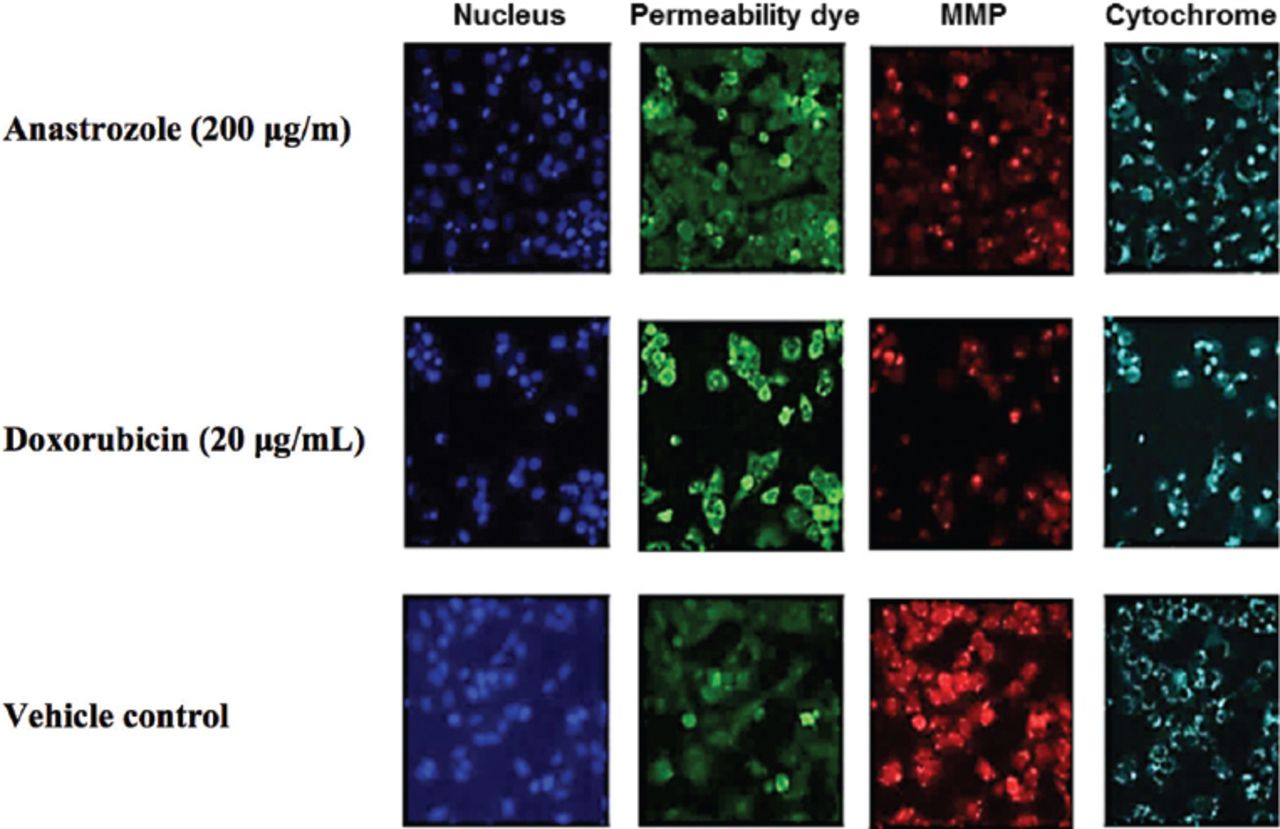
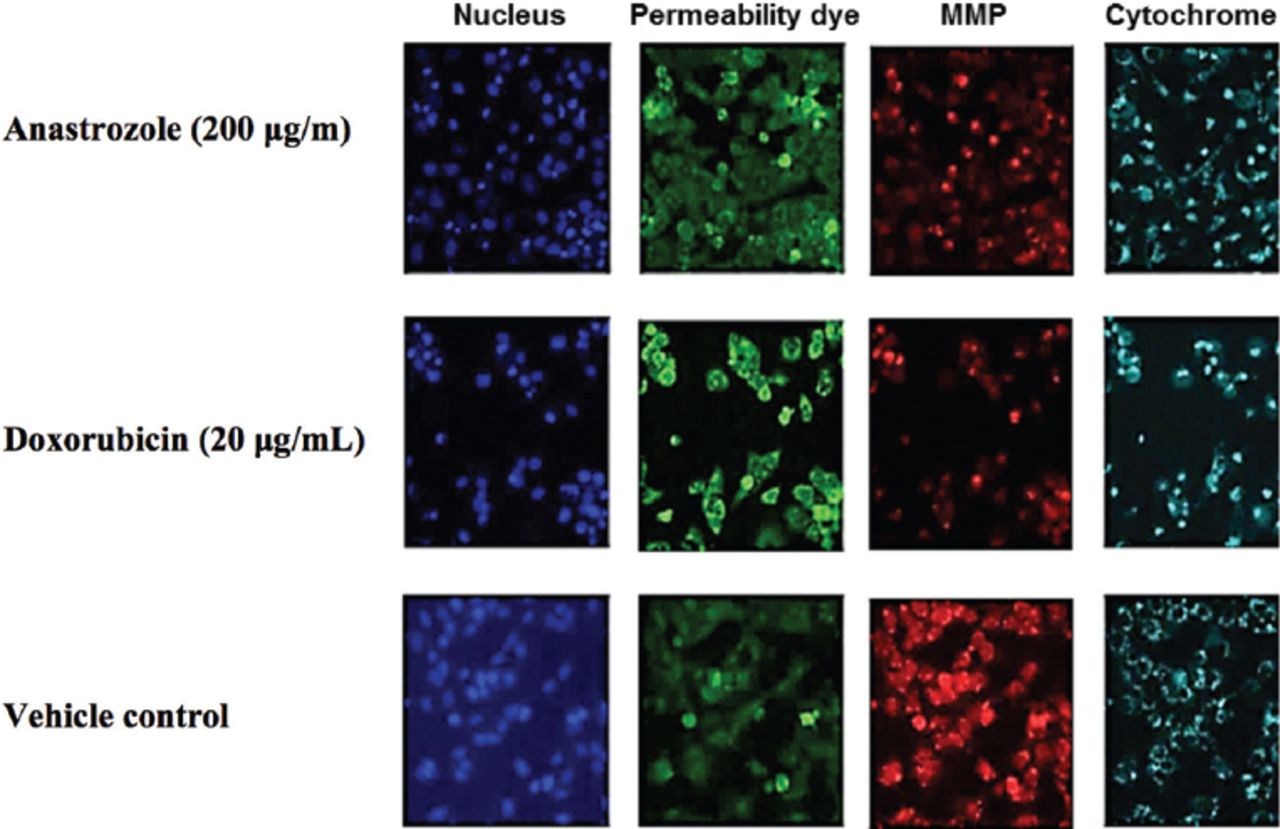
Multipara meter cytotoxicity analysis of anastrozole treated human breast cancer cells line, MMP - Mitochondrial membrane potential
Cell viability
Cell viability is one of the main tests that can be used in toxicity assays.24 Cell viability test indicates that there was a slight increase in cell viability when concentration of anastrozole was reduced. The cell viability percentage was 88.6 when the concentration of anastrozole was 200, 95.3 (100), 99.9 (50) and 99.9 (25) µg/mL. The cell viability was 46.7% when doxorubicin (20 µg/mL) was used.
Nuclear intensity
The MCF7 breast cancer cells treated with anastrozole were stained with Hoechst 33342 dye and the nuclear morphological changes within the cancer cells were examined. The results of nuclear intensity are shown in Figure 1. The nuclear intensity corresponding to apoptotic changes was 38% after anastrozole (200 µg/mL) treatment in breast cancer cells when compared to the standard (20 µg/mL). No significant differences between other anastrozole concentrations (100, 50, and 25 µg/mL) were observed when compared with the standard (20 µg/mL).
Cell membrane permeability
Figure 2 reveals the effect of anastrozole was dose dependent in which the intensity of MCF7 cell permeability increased when the anastrozole concentration also increased. The dose-dependent increase in cell membrane permeability was best significant (17.3%) when anastrozole (200 µg/mL) was used compared to the standard (20 µg/mL).
Mitochondrial membrane permeability
The effect of anastrozole on changes in mitochondrial membrane permeability was investigated and the results are shown in Figure 3. The dose-dependent increased mitochondrial membrane permeability percentage was significant (65.4%) when anastrozole (200 µg/mL) was compared with the standard (20 µg/mL).
Cytochrome c
The treatment of cells with anastrozole (25, 50, 100 and 200 µg/mL) caused a significant increase in cytochrome c releasing intensity (Figure 4). The cytochrome c intensity percentage was 29.2% when anastrozole (200 µg/mL) compared with the 41.4% obtained from the standard (20 µg/mL).
Figure 5 shows images of MCF7 cell treated with anastrozole (200 µg/mL), and doxorubicin (20 µg/mL) as a positive control, and culture medium only as a control. The cells were stained with Hoechst 33342 dye (excitation 350/emission 461), cell membrane permeability dye (excitation 491/emission 509), MMP dye (excitation552/emission 576), and cytochrome c antibody. Anastrozole (200 µg/ml) stained the cells and show a similar staining effect as for the standard (doxorubicin; 20 µg/mL).
Discussion
The MTT (pale yellow) cytotoxicity assay is based on the ability of mitochondrial dehydrogenase enzymes from viable cells to cleave the tetrazolium rings of MTT. Dark purple formazan crystals were formed, which are largely impermeable to cell membranes and accumulate within healthy cells. The level of formazan produced is directly proportional to the number of surviving cells. The results indicated a decrease in cell viability after treatment of 3 cell lines with the aromatase inhibitor anastrozole, but the MCF7 cells were more sensitive toward anastrozole when compared with HepG2 and PC3 cell lines used. The results were in agreement with the literatures in which the mechanism of anti-proliferative effects of anastrozole on breast cancer cells was suggested.25,26 Therefore, the cytotoxicity of anastrozole on MCF-7 cells was studied further using HCS assay.
Screening potential drugs for in-vitro toxicity is very important in the drug discovery process. Toxicity of cells can lead to either necrosis or apoptosis along with other changes in nuclear morphology, mitochondrial function and cell permeability.24 Cell toxicity can also lead to the loss of mitochondrial membrane potential and hence the release of cytochrome c from mitochondria.24 In-vitro cytotoxicity test is designed to measure the lowest anastrozole dose that can cause cell toxicity. The changes in cell viability have a positive correlation with the toxic effect of the anastrozole tested. The toxic effect on MCF7 cell viability increased with the anastrozole concentration elevation. The most significant reduction (p<0.05) in cell count was at the high anastrozole concentration (200 µg/mL). Evidently, MCF7 cell viability was dose dependent after 24 hours of treatment with different concentrations of anastrozole, which affect the cellular survival of MCF7 cells and reduced the cell count. In postmenopausal women, anastrozole is metabolized within 3 days after the does. Unchanged anastrozole (10%) and anastrozole metabolites (60%) were identified in the urine.27 Triazole was the most common identified anastrozole metabolite in the urine.27
Nuclear condensation and/or fragmentation is a hallmark for apoptosis.28 The results of nuclear intensity show that MCF7 nuclear intensity increased significantly when the concentration of anastrozole was increased. The influence of anastrozole was dose dependent.
Dye-permeability assays are used in cell biology which provide an indication of the integrity of cell membranes.29 However, dye molecules cannot penetrate intact membranes, but can traverse the damaged cell due to their polar nature.30 Cell membrane permeability is a key parameter for the evaluation of the cell compound interaction, the high doses of the anastrozole increased cell membrane blebbing leading to an increasing cell membrane permeability. The changes in cell membrane permeability are usually associated with apoptotic responses, and the cell membrane integrity loss is a common phenotypic feature of marked cytotoxicity.31
Membrane potential is a central feature of healthy mitochondria, and membrane depolarization is a good indicator of mitochondrial dysfunction, which is increasingly implicated in drug toxicity.32 After toxicity, cells often undergo either apoptosis or necrosis along with other changes in mitochondrial function. This leads to the loss of mitochondrial membrane potential and hence cytochrome c release from mitochondria.33
Cytochrome c, which exists between the inner and outer mitochondrial membranes has a significant role to play in apoptosis. An apoptotic stimulus triggers the release of cytochrome c from the mitochondria into the cytosol.34 Cytochrome c stained weakly. In contrast, anastrozole treated-MCF7 showed strong staining around the nucleus (Figure 5). The treatment of breast cancer cells with anastrozole could trigger the translocation of cytochrome c to the cytosol from mitochondria.
Study limitations
The current study has a number of limitations. First, only few types of cancer cell lines were used. Second, there is a biases possibility. Third, the process could be expensive for large scale treatment. Fourth, only few concentrations of anastrozole were used. Fifth, anastrozole has a toxic effect. A more detailed study is still needed to establish the effect of anastrozole against various cancer cell lines and to confirm the ideal treatment duration. However, the current study provides the primarily results for the use of anastrozole as anticancer drug against breast cancer. Also, it confirms the link between anastrozole and aromatase enzyme inhibition.
In conclusion, anastrozole showed a cytotoxic effect against MCF7, HepG, and PC3 determined in-vitro by the MTT assay. The HCS technique for anastrozole showed a toxic effect toward MCF7 cell line in a dose-dependent manner with an elevation in cell membrane permeability, cytochrome c, and nuclear intensity. Changes in mitochondrial membrane potential and a decreasing cell viability level were also observed. Anastrozole inhibits the aromatase enzyme and hence the aromatization mechanism; however, it has a toxic effect.
Copyright
Whenever a manuscript contains material (tables, figures, etc.) which is protected by copyright (previously published), it is the obligation of the author to obtain written permission from the holder of the copyright (usually the publisher) to reproduce the material in Saudi Medical Journal. This also applies if the material is the authors own work. Please submit copies of the material from the source in which it was first published.
Acknowledgment
he authors extend their appreciation to the College of Applied Medical Sciences Research Centre and the Deanship of Scientific Research at King Saud University, Riyadh, Kingdom of Saudi Arabia for their funding of this research and to Al-Nahrain University, Baghdad, Iraq for continued support.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company. The study was supported by the King Saud University, the Deanship of Scientific Research, Riyadh, Kingdom of Saudi Arabia and Al-Nahrain University, Baghdad, Iraq.
- Received October 3, 2016.
- Accepted December 16, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.