


Abstract
Pediatric regional anesthesia is widely used to relieve postoperative pain after abdominal surgery. Commonly used techniques of regional anesthesia include lumbar epidural and caudal block. However, the use of central neuraxial blockade has limitations. It is contraindicated in patients with clotting abnormalities, spinal dysraphism with tethered cord syndrome, meningomyelocele, and following spinal surgery with instrumentation. Ultrasound guided transversus abdominis plane block is a new method of regional anesthesia that can be used in settings where central neuraxial blockade is contraindicated. In this study, we present 5 pediatric cases in which major abdominal surgery was performed but central neuraxial blockade could not be carried out due to spinal abnormalities.
Regional anesthesia is widely used for postoperative pain control in pediatric patients. Caudal epidural block (CEB) is the most commonly used method for postoperative analgesia in children.1 Due to its ease of use and high success rate, it is currently considered the gold standard for pain relief after lower abdominal and pelvic surgery in children.1 However, being a central neuraxial block it may be contraindicated in some cases, including coagulation disorders, spinal malformations including meningomyelocele, tethered cord syndrome and after spinal surgery.2 Improved understanding of abdominal wall anatomy has led to the use of transversus abdominis plane block (TAPB) to control postoperative pain after lower abdominal surgery.3,4 Rafi5 first described a “blind” abdominal field block technique performed through the inferior lumbar triangle (Petit’s triangle). The inferior lumbar triangle is formed inferiorly by the iliac crest, anteriorly by the external oblique, and posteriorly by the latissimus dorsi muscles. This method provides blockade of lumbar anterior spinal nerves from T10-L1. After the introduction of ultrasound-guided techniques in regional anesthesia, Hebbard et al6 described the technique of TAPB using real time ultrasound guidance. They placed the ultrasound probe between the costal margin and the iliac crest on the anterior axillary line at the level of the umbilicus. Ultrasound-guided TAPB was performed with local anesthetic administration between the fascial planes of the internal oblique and the transversus abdominis muscles. In this study, we present the cases of 5 pediatric patients with spinal dysraphism who underwent TAPB for postoperative pain relief after major abdominal surgery.
Case Report
Patient 1
A 12-year-old girl weighing 14 kg presented with lumbosacral meningomyelocele without sensory deficit over the anterior abdominal wall. Her medical history revealed hydrocephalus and spina bifida. She was scheduled to undergo a laparoscopic cholecystectomy. Her physical examination did not reveal any significant findings. Hemoglobin, hematocrit, platelet count, coagulation profile, liver enzymes, bilirubin levels, blood glucose, serum creatinine, serum urea, serum sodium and potassium levels were within normal limits in preoperative investigations. There were no abnormal findings on the preoperative chest x-ray (Table 1). Preoperative investigations revealed no abnormal findings.
Patient 2
A 5-year-old boy weighing 15 kg presented with neurogenic bladder dysfunction due to lumbosacral meningomyelocele. He had no sensory deficit over the anterior abdominal wall. His medical history included hydrocephalus and spina bifida. He was scheduled for bilateral ureteroneocystostomy. The physical examination did not reveal any significant findings. Hemoglobin, hematocrit, platelet count, coagulation profile, liver enzymes, bilirubin levels, blood glucose, serum creatinine, serum urea, serum sodium and potassium levels were within normal limits in preoperative investigations. There were no abnormal findings on the preoperative chest x-ray (Table 1). Preoperative investigations revealed no abnormal findings.
Patient 3
A 12-year-old girl weighing 17 kg presented with lumbosacral meningomyelocele. She had no sensory deficit over the anterior abdominal wall. Her medical history included scoliosis, hydrocephalus, and spina bifida. She was scheduled for laparoscopic insertion of a peritoneal dialysis catheter. Her physical examination did not reveal any significant findings. Hemoglobin, hematocrit, platelet count, coagulation profile, liver enzymes, bilirubin levels, blood glucose level, serum sodium and potassium levels were within normal limits in preoperative investigations. Blood urea level was 80 mg/dl and serum creatinine level was 2.4 mg/dl. There were no abnormal findings on the preoperative chest x-ray (Table 1). Preoperative investigations revealed elevated urea and creatinine levels.
Patient 4
A 10-year-old boy weighing 35 kg presented with lumbosacral meningomyelocele. He had no sensory deficit over the anterior abdominal wall. His previous medical history included spina bifida. He was scheduled for laparoscopic intraabdominal testis exploration. There were no significant findings on physical examination. Hemoglobin, hematocrit, platelet count, coagulation profile, liver enzymes, bilirubin levels, blood glucose, serum creatinine, serum urea, serum sodium and potassium levels were within normal limits in preoperative investigations. There were no abnormal findings on the preoperative chest x-ray (Table 1). Preoperative investigations revealed no abnormal findings.
Patient 5
A 13-year-old girl weighing 18 kg presented with lumbosacral meningomyelocele. She had no sensory deficit over the anterior abdominal wall. Her medical history included scoliosis, hydrocephalus, and spina bifida. She was scheduled for laparoscopic insertion of a peritoneal dialysis catheter. Her physical examination did not reveal any significant findings. Hemoglobin, hematocrit, platelet count, coagulation profile, liver enzymes, bilirubin levels, blood glucose level, serum sodium and potassium levels were within normal limits in preoperative investigations. Blood urea level was 74 mg/dl and serum creatinine level was 2.1 mg/dl. Her preoperative chest x-ray revealed scoliosis. Pulmonary function tests were within normal limits (Table 1). Preoperative investigations revealed elevated urea and creatinine levels.
Timeline including diagnostic tests, interventions, and follow ups.
Therapeutic intervention
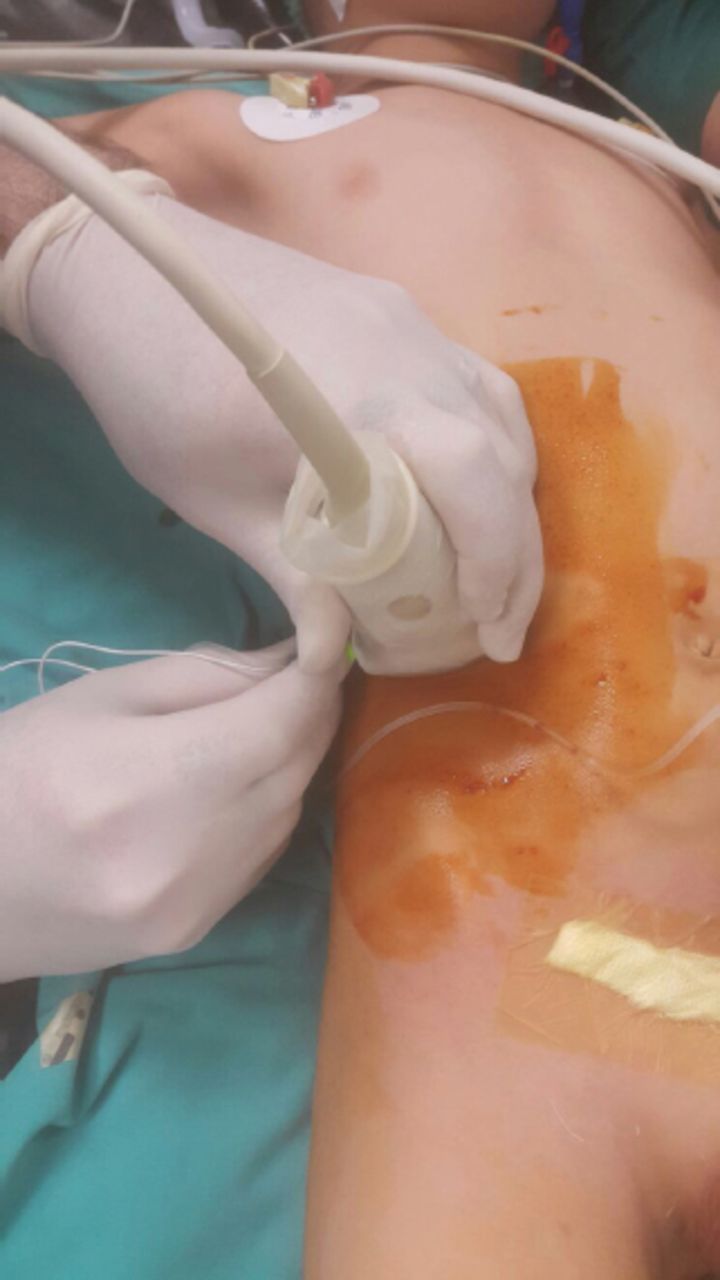
All patients received sedation with a routine 1 mg of midazolam in the operation room. During the surgery, heart rate (HR), arterial oxygen saturation, end-tidal carbon dioxide, and non-invasive blood pressure (BP) were monitored. After commencement of monitoring, anesthesia was induced with intravenous administration of propofol 2 mg/kg; fentanyl, 2 mcg/kg; and mivacurium, 0.2 mg/kg; followed by endotracheal intubation. Anesthesia was maintained with a 50/50% mixture of oxygen/nitrous oxide and sevoflurane at 1-1.5 vol %. The concentration of sevoflurane was decreased towards the end of surgery until patients were awake. No intraoperative complications were encountered. After surgery, bilateral TAPB was carried out under ultrasound guidance. Using an in-plane approach, a high-frequency, 7.5 MHz linear probe (Esaote, My Lab 30cv, Florence, ITALY) was placed in the mid axillary line between the costal margin and the iliac crest and moved forward towards the umbilicus (Figure 1). A mixture of 2 ml of 0.125% bupivacaine and 2 ml of 0.2% lidocaine diluted in 4 ml of normal saline was injected on each side. After performing the block, patients were extubated awake in the operating room and followed up after recovering from anesthesia.

Ultrasound guided transversus abdominis plane block.
Follow up and outcomes
Pain scores were assessed at 0, 1, 4, 6, 12, and 24 hours postoperatively using the Faces Pain Scale-Revised (FPS-R). Systolic and diastolic BP and additional analgesic requirements were recorded (Table 2). Blood pressure and HR were recorded post-operatively for 24 hours (Table 3). If the pain score was more than 5, 10 mg/kg of paracetamol was administered intravenously for additional pain relief.
Postoperative faces pain scale-revised score.
Postoperative hemodynamics values (mmHg per minutes)).
Discussion
There is increasing research evaluating the efficacy of TAPB for postoperative analgesia following lower abdominal surgery. In a study by Sethi et al,4 TAPB resulted in less pain compared to caudal epidural 6 hours postoperatively; there was no difference in opioid use between groups block; although no difference was observed in the first 12 hours, postoperative morphine requirement at 24 hours was less in patients who had TAPB than in those who underwent caudal epidural block.7 In another study, Kendigelen et al3 compared TAPB with wound infiltration and found that postoperative pain scores and analgesic requirements were higher in the wound infiltration group. In our study, adequate analgesia was achieved in all patients in the first 24 hours after ultrasound-guided TAPB and no additional dose of analgesics was required.
The term “spinal dysraphism” describes any abnormality of the spinal cord, cauda equina and overlying tissues, including skin, muscles and vertebrae.8 Spinal dysraphism includes meningocele, meningomyelocele, tethered cord, sacral agenesis, and spina bifida.7 Several neurological, orthopedic, cardiac, urological, and vertebral defects are commonly observed in these patients.8 Central neuraxial blockade for postoperative analgesia is contraindicated in patients with spinal dysraphism.8 Wild et al9 used a subcutaneous catheter for continuous local anesthetic infusion in patients with spinal dysraphism and provided effective postoperative analgesia. However, subcutaneous infected seromas were observed as a complication in these patients. Taylor et al10 also performed continuous TAPB using ultrasound guided catheters in patients with spinal dysraphism. John et al11 conducted a multi-center study (1994) to investigate the safety of TAPB in children and found a 0.3% incidence of block-related complications. These complications were minor and no further intervention was needed. In bilateral blocks, median dose of bupivacaine was found to be one (0.47-2.29) mg/kg. In our study, the bupivacaine dose used in bilateral blocks was comparatively less; a single dose of local anesthetic for TAPB did not lead to any complications.
In conclusion, our patients received a single bolus dose of ultrasound-guided TAPB; and the maximum pain score reported was 4 out of 10 points on the Visual Analog Scale for Pain. Further, no additional dose of analgesics was required. No side effects related to TAPB were observed in these patients. We believe that TAPB may be an efficient technique of postoperative analgesia in spinal dysraphism. Larger series comparing TAP block with other method of postoperative analgesia are warranted in patients with spinal dysraphism.
Footnotes
Disclosure
Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 13, 2017.
- Accepted October 25, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.