


Abstract
Intra-parenchymal sialolithiasis and subsequent fibrosis of the submandibular salivary glands is a rare disorder. The resulting swelling, pain, and infection derives affected patients to seek treatment. We present the case of an 85-years-old Saudi male patient who suffered from repeated swelling and infection in the left submandibular region which was misdiagnosed and treated for over 60 years as dental infection, infected skin sebaceous gland or lipoma. The presented case represents the largest intra-glandular submandibular stone with the longest duration ever reported in the medical literature.
Sialolithiasis is the most common disease of salivary glands, accounting for more than 50% of salivary gland diseases.1 It affects males more frequently than females.2 Sialolithiasis is mostly described as a disease of the adult population that very rarely affects children.2,3 The great majority of salivary calculi (over 80%) occurs in the submandibular gland, mainly in its ductal system, followed by smaller percentages of the parotid, at 5% to 10%, and rare occurrence reported in the sublingual gland and the other minor salivary glands.1-3
The exact etiology of salivary stones is still unknown, but several factors contribute to their development in the submandibular gland like mechanical, inflammatory, chemical, neurogenic, infectious, and foreign bodies.4 Salivary stones can occur in the glandular parenchyma or in the salivary ductal system, as single or multiple stones, unilaterally or bilaterally, and can vary in shape and size. The ducts and the hilus of the gland are the common sites of occurrence of sialoliths, whereas sialoliths on the parenchyma occur in 9% to 17% of all cases, especially when affecting the submandibular gland.5
Sialolithiasis may occur unilaterally or very rarely bilaterally.3 The shape of salivary stones depends on where the stones originate. Stones originating from the ductal system are mostly elongated, whereas stones originating from the hilus or within the gland parenchyma are round or oval.6-10 The size of sialoliths also varies considerably from small particles, described as salivary sand, to a giant calculus, also described as megaliths.1,2 Giant sialoliths (megaliths) are rare, especially when they form within the parenchyma of submandibular gland. Bimanual palpation of the floor of the mouth, in a posterior to anterior direction, reveals palpable stones in many cases of submandibular ductal calculi.3 The symptoms affecting patients, in general, are mainly during mealtimes because of the high stimulation of salivary secretion in a partially obstructed gland, although sometimes the saliva manages to leak around the sialolith resulting in an asymptomatic obstruction. On the contrary, complete obstruction causes constant pain and swelling, in addition to the absence of infection, which can lead to atrophy of the gland with lack of secretory function and eventually fibrosis. Imaging modalities both conventional and advanced are very useful. One of the conventional methods for visualizing radiopaque stones is a standard mandibular occlusal radiograph, and because of the gland’s posterior inferior position, a mandibular lateral oblique may be useful as well. Computed tomography (CT) scan, which is the diagnostic modality used in our case, is a noninvasive procedure especially useful for evaluating of the number of stones and the inflammatory conditions associated with sialolithiasis. The treatment objective for sialoliths is the recovery of normal salivary secretion. This is achieved by considering several factors: the size, position, and the number of calculi. Surgical removal of large sialolith located in the ductal part of the gland can be performed through an intraoral approach (trans-oral sialolithotomy). Another course of action is the removal of the gland itself (sialoadenectomy) via an extraoral approach when the stones are presented intraglandularly. Small calculi are treated by more conservative methods such as endoscopy, shockwave lithotripsy, and intraductal laser fragmentation techniques.5
Case Report
An 85-year- old Saudi male patient was referred to the Oral and Maxillofacial Surgery Department, AlKharj Military Industries Hospital, Riyadh, Saudi Arabia, for consultation and treatment of large swelling on the left side of the neck. His medical history did not contribute to the lesion. He reported that the swelling appeared over more than 60 years ago. During these past years, the patient has sought treatment in different hospitals for repeated infections and pain related to the growing mass but he was given variable treatments, mainly antibiotics, to resolve the acute phase. Different diagnoses were attributed to the swelling by the different treating clinicians including skin infection, dental infection and lipoma (Figure 1).

Clinical extra-oral view showing submandibular swelling of the left side of the neck.
Clinical findings
Upon clinical examination, the neck mass was bony hard and located in the left submandibular region, extending to the neck. The mass is non-tender, and the related neck lymph nodes are normal. Intra-oral examination showed normal oral tissues and normal salivary flow from all major salivary glands except the left submandibular gland, where no salivary flow is noted from the orifice of wharton’s duct after manual milking of the gland.
Diagnostic assessment
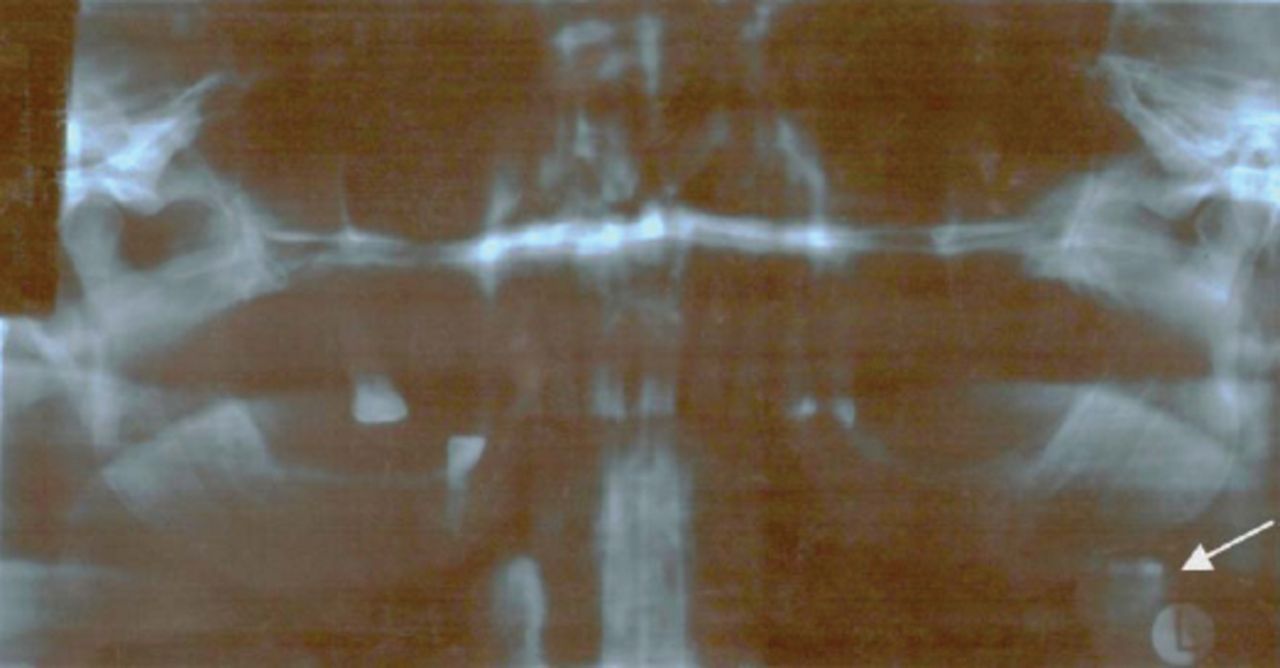
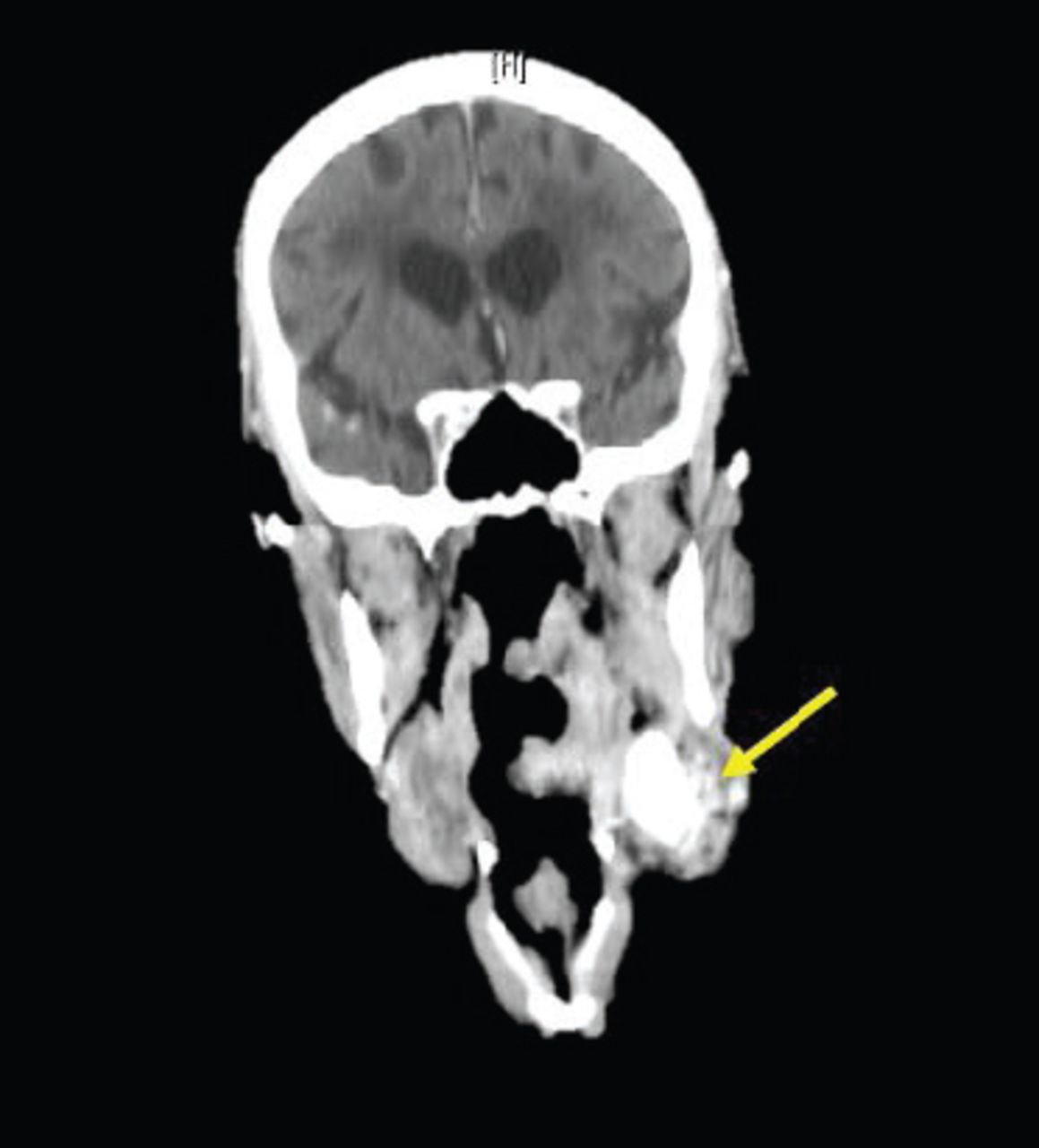
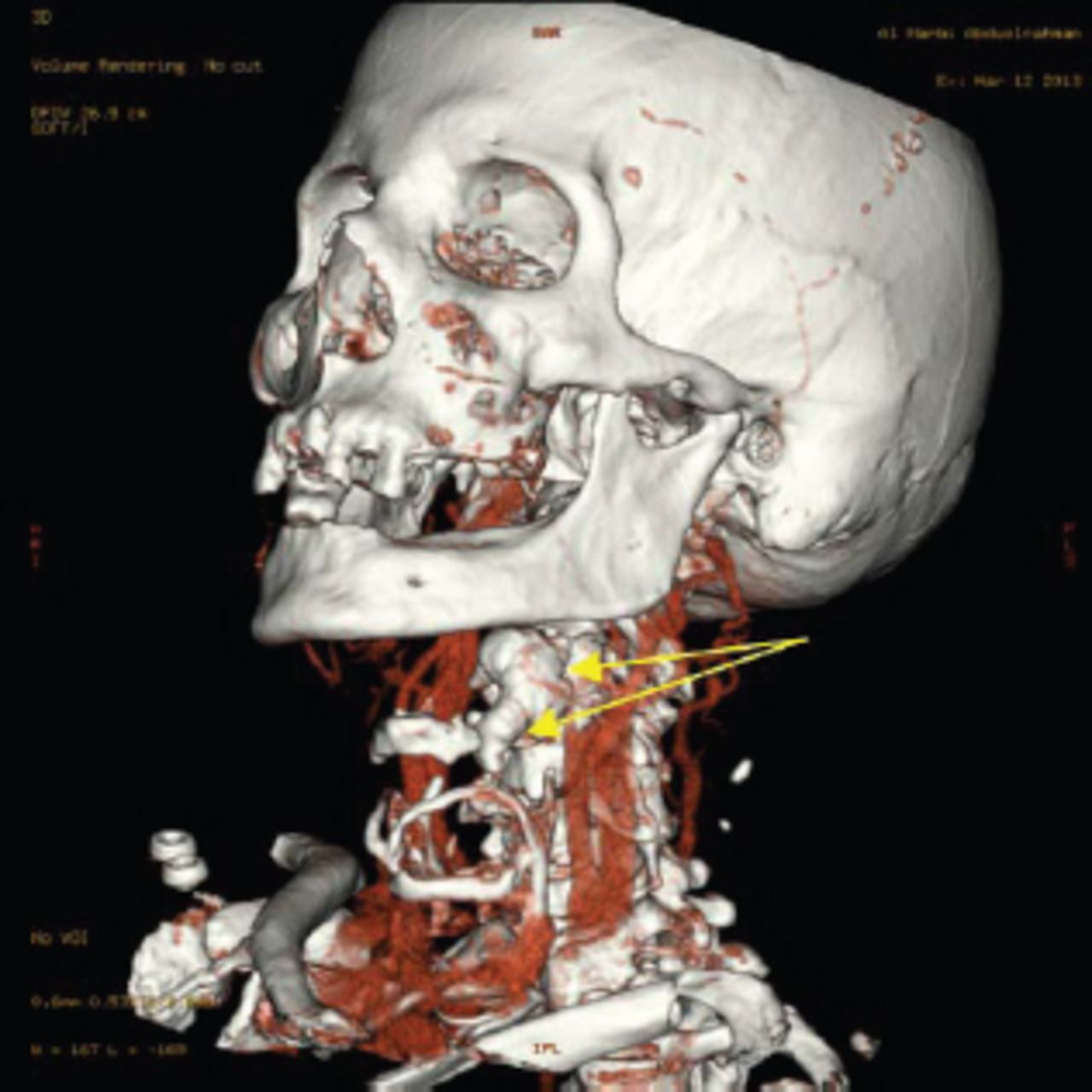
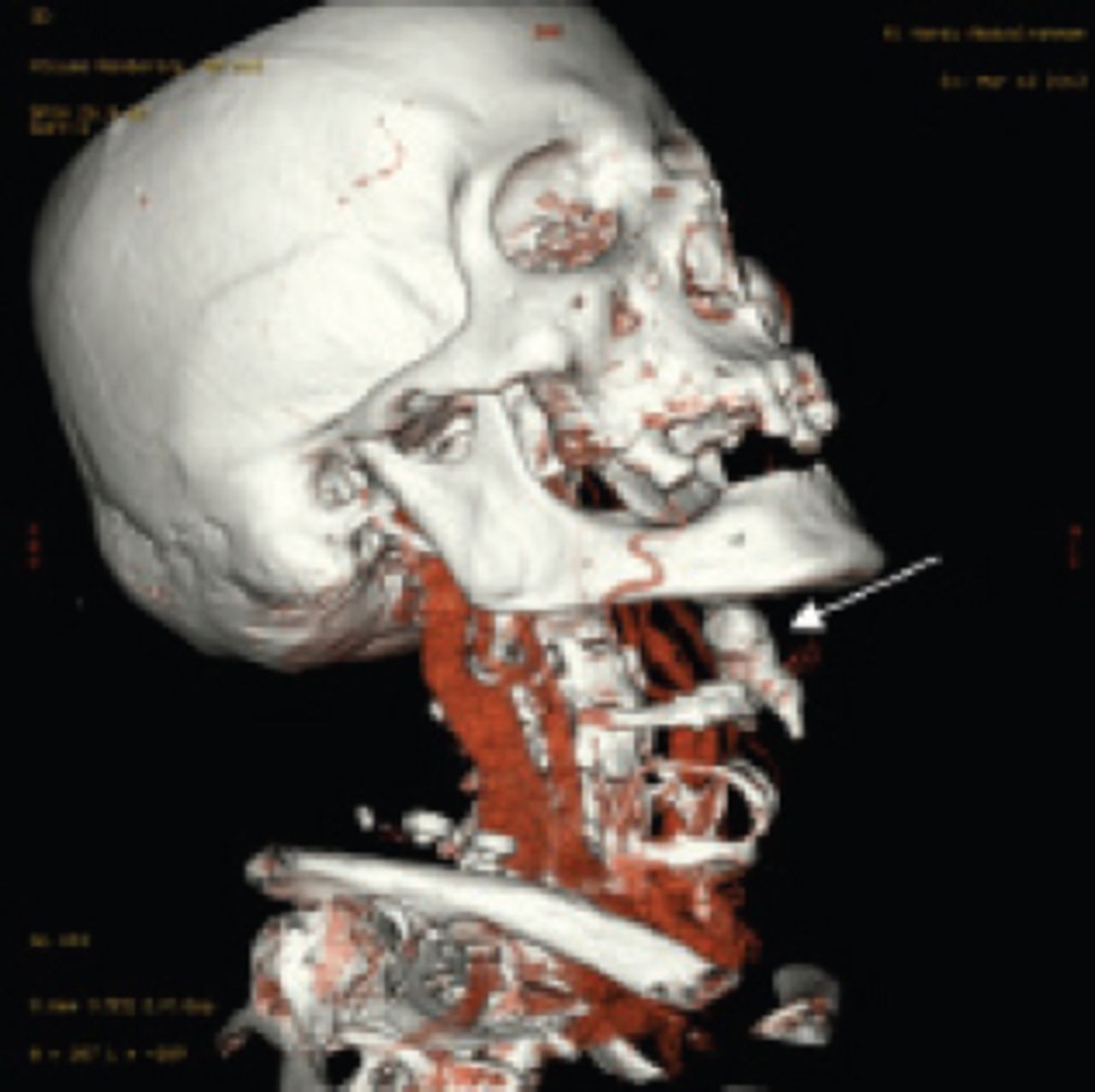
The initial ortho-pantomo-graphic (OPG) x-ray showed a large calcified mass in the left submandibular region. Reviewing an old OPG x-ray of the patient taken about 12 years earlier showed the same calcified mass in the same region but of a smaller size (Figures 2 & 3). The differential diagnosis of the lesion includes; long-standing fibrosis of the left submandibular salivary gland or a giant salivary gland stone (megalith) with subsequent gland fibrosis. Therefore, CT scan of the head and neck region with contrast dye and 3D reconstruction was requested to confirm the diagnosis. The CT scan confirmed the presence of a well-defined bone-density calcified submandibular lesion measuring 30 x 20 x 15 mm with smooth margins exactly within the submandibular salivary gland region, with inflammatory dirty fat appearance around and peripherally enhancing dilated ducts related to the mass, and it shows no evidence of invasion or bony destruction. In addition, there is no evidence of lymph nodes or abnormalities seen in other neck structures (Figures 4-6).

Ortho-pantomo-graphic (OPG) x-ray view at the time of presentation showing a calcified mass in the left submandibular region (arrow).

Ortho-pantomo-graphic (OPG) x-ray view 12 years earlier to the time of presentation showing a calcified mass in the left submandibular region (white arrow).

CT coronal view showing a salivary stone within the left submandibular salivary gland.

CT 3D view showing left submandibular salivary stone (arrows) with smooth surface caudal extension closely related to the hyoid bone.

CT 3D view showing the left submandibular salivary stone (arrow) and its relation to adjacent structures without any bony invasion.
Therapeutic intervention
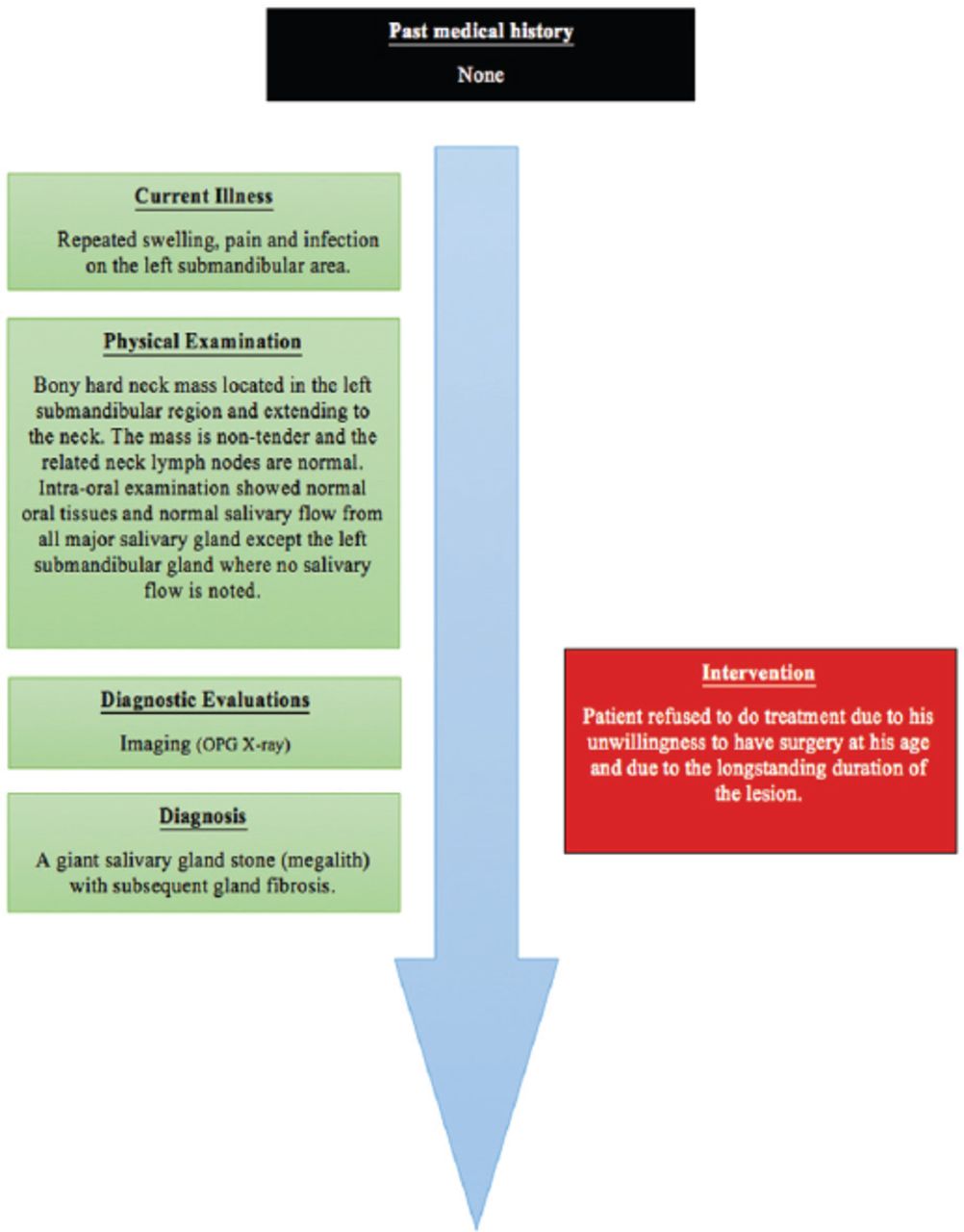
Megalith with subsequent gland fibrosis and infection was diagnosed and discussed with the patient. Unfortunately, he refused to undergo any surgery to remove the affected gland together with its stone. His refusal to treatment was merely due to his unwillingness to have surgery at his age and due to the longstanding duration of the lesion (Figure 7).

Patient’s timeline.
Discussion
The presented case has many unique characteristics compared with the previously reported cases in the medical literature. Firstly, it represents the longest duration of the disease ever reported, which is over 60 years, without progressing to a more life-threatening condition or a major health issue.
Secondly, the size of the reported megalith, to the best of our knowledge, is one of the largest reported salivary intra-parenchymal submandibular gland stones compared to previously reported cases.6-10 In addition, the size of the reported megalith together with the long duration of the disease confirms that salivary stones grow over time.
Thirdly, unlike other previous cases,6-10 the shape of the reported megalith is irregular rather than oval or round with an extension approaching the hyoid bone without any serious effects of the nearby vital structures.
Fourthly, despite the prominent physical disfigurement caused by the disease and failure to resolve it by different medical treatments offered over 60 years, none of the treating physicians and dentists thought of submandibular gland disease or requested a simple and routine investigation such as CT scan, MRI or ultrasound examination. Although the patient refused to undergo treatment due to his old age and the longstanding presence of the stone, for such large sialoliths, sialoadenectomy remains the golden standard of management.
In conclusion, proper evaluation of the swelling in the submandibular area and the use of adequate imaging modalities will lead the clinician to the correct diagnosis, which will provide the patient with the appropriate treatment option to prevent possible severe complications.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 5, 2018.
- Accepted May 30, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.