


Abstract
Schistosomal cholecystitis is remarkably uncommon disease which is associated with concomitant gallstone disease. The disease prevails with low socio-economic conditions of population. It is still not clear that the widespread fibrocalcific reaction in the wall of gallbladder and the cystic duct, observed for all the reports, predisposes to cholelithiasis or gallstones coexist. In the present study, we report a case of the Saudi male patient affected with schistosomal granulomatous lithiasic cholecystitis. The patient’s gallbladder was badly inflamed therefore performing a safe cholecystectomy in the patient was extremely difficult. Also, infection with schistosoma is related with chronic granulomatous inflammation making the cholecystectomy procedure difficult and risky, therefore, we mainly focused on preventing the injury of bile duct by being prepared that the patient will present a complicated case. This was achieved by using the technique of laparoscopy to safely excise the gall bladder.
Schistosomiasis is caused by trematode helminth of genus schistosoma. It is a deadly parasitic disease which infects more than 200 million individuals worldwide. It ranks second only to malaria in terms of its impact. The disease is acquired and transmitted mostly due to low socioeconomic and poor sanitary conditions of the inhabitants. The disease burden is especially high in the developing nations. The disease is acquired in humans by contact with infected water and spreads as an endemic when they are exposed to this water due to agricultural activities, daily chores and recreational activities such as swimming and water sports.1 The parasite first identified to cause schistosomiasis was Schistosoma hematobium (S. hematobium). There are 5 species of schistosoma are now known to infect the human host, Schistosoma mansoni (S. mansoni), Schistosoma haematobium (S. haematobium), Schistosoma japonicum (S. japonicum), Schistosoma intercalatum (S. intercalatum), and Schistosoma mekongi (S. mekongi).2 Schistosomiasis is also known as snail fever since the parasite develops and multiplies in certain types of snails. Once the parasite enters human body by penetration through skin, it matures and releases eggs that travel either to bladder or intestine which eventually can be passed out in urine or faeces thus continuing the cycle. Eggs that are not passed out of the body remain in the bladder or intestine itself causing symptoms of the disease and inflammation. Gastrointestinal manifestations of the disease are mainly caused by deposition of the eggs of S. mansoni in the walls of the gut.3 Schistosomal cholecystitis, one of the gastrointestinal presentations of schistosoma, is a rare condition where the patients are mostly found to have concomitant gall stones as well. However, it is not clear whether the reaction to deposition of eggs in the gallbladder walls trigger this acute cholecystitis or gallstones co-exist.4 In the present study, a 50 years old male patient was presented with a rare condition of granulomatous cholecystitis related with deposition of S. mansoni eggs in the gallbladder with concomitant cholelithiasis. The infection was acquired due to drinking of contaminated water by the patient. The patient did not show any sign of hepatosplenic or urinary symptoms.
Case Report
A 50-year-old obese diabetic male, born in Saudi Arabia, was presented to our department for elective laparoscopic cholecystectomy. He hailed from rural area with poor socioeconomic and sanitation status. He was suffering from gallbladder symptoms since past 9 years and was on oral hypoglycemic medication. He had been following the hospital for 3 months with recurrent attacks of biliary colic and multiple emergency department visits for pain control. All throughout this period, he kept afebrile.
Clinical findings.
In the clinic, he reported a history of repeated nausea and vomiting with weak abdominal pain originating from the right upper quadrant. Physical examination was carried out at the time of admission revealed tenderness at the sight of pain and a +/- Murphy sign with no palpable mass. Table 1 summarizes the time line of the case, interventions given, and the progress of procedure conducted on the patient.
Summary of the patient’s history and follow up with interventions given.
Diagnostic assessment
Laboratory tests showed normal white blood cells count of 10.6 × 109/L (normal range: 4.5 to 11.0 × 109/L), Alkaline phosphatase (ALP), Aspartate aminotransferase (AST), alanine aminotransferase (ALT) and bilirubin levels with a mild increase in γ-glutamyl transpeptidase (147 IU/L). Upper abdominal ultrasound revealed a fatty liver and 2 gallstones measuring 8mm in diameter in the dependent portion of the gallbladder with acoustic shadowing and normal wall thickness (4 mm). No distension of the gallbladder was seen. Because of the patient’s morbid obesity there was a sonographic suggestion of early acute cholecystitis. Since he showed no clinical symptoms of acute disease such as fever or leukocytosis, elective cholecystectomy was performed. On performing laparoscopy, gallbladder was identified to have a very thick wall and appeared grey in color. The laparoscopy operation was straight forward and all the standard way of performing laparoscopic cholecystectomy 4 ports with all the precautionary measures to protect the vital structures was performed. Mobilization and retraction of the gallbladder was difficult due to its strong adhesions to the hepatoduodenal ligament and impacted stone in bladder neck. Since the gallbladder was firmly attached to the liver bed, its dissection was very difficult. The wall of the gallbladder appeared extremely thick and inflamed with necrotic spots which made mobilization really hard to accomplish. Aspiration of the distended gallbladder was carried out to ease the manipulation of its fundus. The gallbladder was evacuated to make it easy to grasp. The impacted stone was thus extracted after draining the contents. By using this approach, cystic duct and artery were easily identified and ligated and finally the gallbladder was safely excised. All this procedure was accomplished laparoscopically.
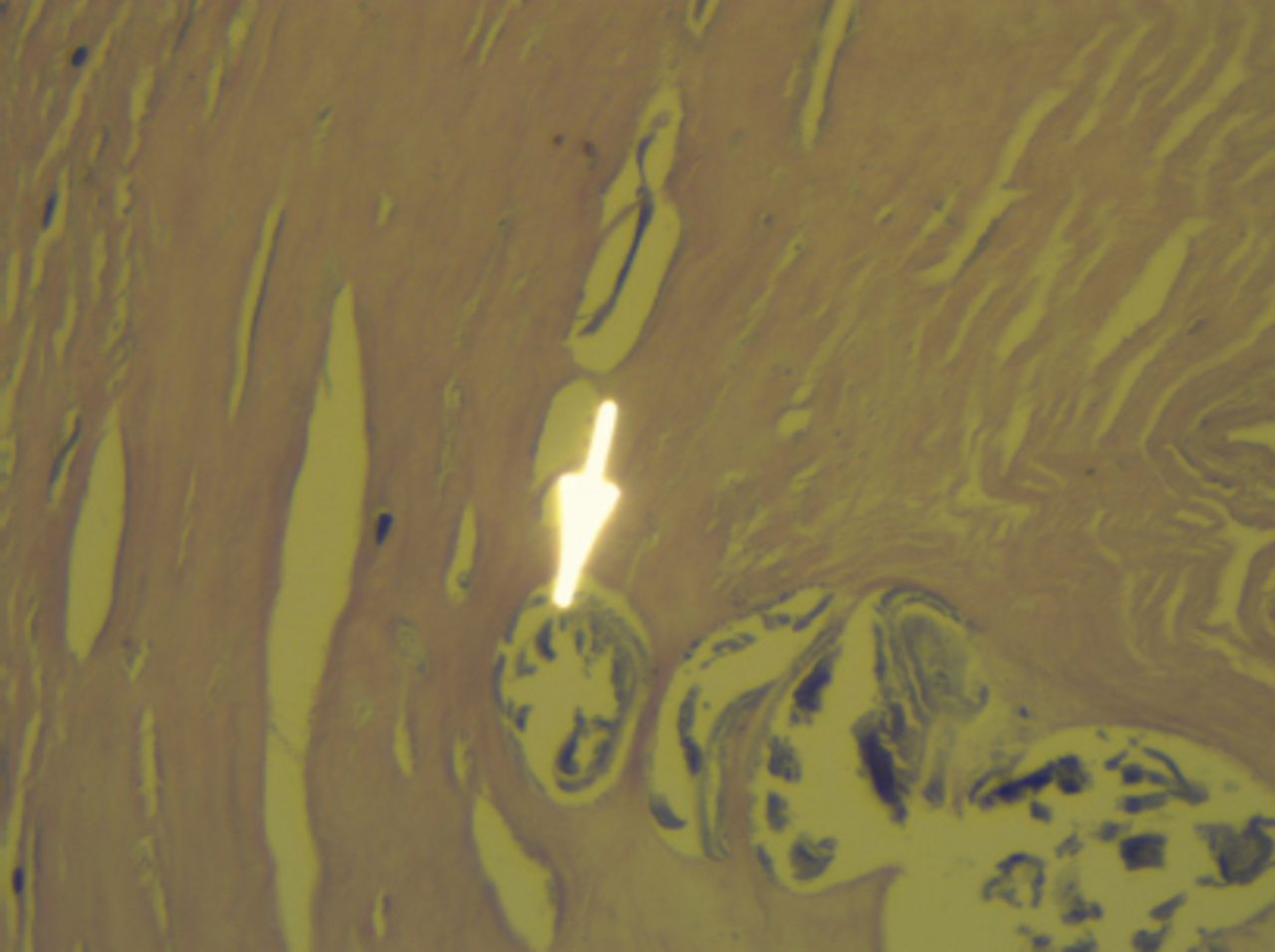
On examining the gall bladder histopathology, marked granulomatous inflammation was observed which surrounded numerous calcified parasitic eggs suggestive of S. haematobium infestation (Figures 1 & 2). He showed remarkable fibrocalcific improvements in both the cystic duct walls and gallbladder. Postoperatively, after the procedure his abdominal pain improved and the laboratory reports also came out to be normal. However, serological testing showed positive schistosoma antibodies but the stool analysis was negative for the parasite. He was further referred to the infectious diseases team to start the therapeutic intervention of praziquantel.

Microscopic image of gall bladder wall showing the presence of Schistosoma haematobium (40x magnification; Haemotoxylin and Eosin staining).

Chronically inflamed gall bladder wall showing the presence of parasitic eggs (Schistosoma haematobium) (40X magnification; Haemotoxylin and Eosin staining).
Discussion
Schistosomiasis is a systemic disease where the parasitic eggs can be found deposited in any tissue of the host. Because of the presence of chronic schistosomiasis, the host body generates an immune response that leads to the development of delayed-type hypersensitivity granulomas.5 Patients having hepatosplenic schistosomiasis are found to have certain ultrasonographic abnormalities such as calcification and thickening of the wall with reduced volume in the gallbladder, as could be seen in our case.6 A very few international reports showed a rare histopathological finding of a granulomatous cholecystitis with schistosomal egg deposition, like that observed in the present case, hence being a rare finding. However, recognizing the disease as schistosomal cholecystitis is a debatable conclusion because a variety of different disease like X-linked chronic granulomatous disease, Crohn’s disease, xanthogranulomatous cholecystitis, fibroelastosis of the gallbladder and infection with Mycobacterium tuberculosis and Candida glabrata may also cause granulomatous cholecystitis. Since S. haematobium is endemic in some regions of the Kingdom, we reasonably assumed that the patient was infected during his long term stay in the southern region. A number of reports of schistosomal cholecystitis are described in the literature but the direct cause of deposition of schistosomal eggs and growth of symptomatic cholecystitis is still unanswered. We found a concurrent presence of cholelithiasis along with schistosomiasis which has been reported in a number of cases known until date.7,8 The patient presented with a strong fibrocalcific reaction accompanied by chronic schistosoma-induced granulomatous inflammation. As suggested by Al-Saleem et al9 this apparent association between cholelithiasis and gallbladder schistosomiasis is linked to fibrotic stenosis of the cystic duct. Also, it can stagnate the bile in the gallbladder and thus helping in the development of gallstones. Contrary to this, another study by Sharara et al10 reported a direct contribution of schistosoma inducing an acute cholecystitis in the host. Indeed, these reports showed cases of lithiasic schistosomal cholecystitis where none of the gallbladder aberrations were ecographically demonstrable, 10 days before the beginning of symptoms.
Schistosomal infection is related with chronic granulomatous inflammation rendering the procedure of cholecystectomy problematic and risky. The medical doctor in charge should keep in their attention the chances of acute biliary episode as a rare complication of infection with S. haematobium. The surgeons working in endemic areas should be highly trained to deal with complicated gallbladder cases with low threshold for open surgery in order to take care of patient safety. The best way to deal with such a case is to follow the laparoscopic excisions of the gallbladder as elaborated in this report.
This disease has also significantly linked with the travel history of patient. In the Western countries, it is observed that many of the previously controlled diseases such as schistosomiasis are recurring because of more reasonable international travel, population migration, labor export, and global trade and commerce. Similar case was observed in our case study patient where the patient had a travel history to the southern regions of the kingdom, an area that is endemic for schistosomiasis. Thus, the medical professionals must know the travel history of the patient to keep a check on the significant features of the pathogens and include them in the differential diagnosis.
In conclusion, it is still indecisive whether the schistosomal eggs deposition in the gallbladder can cause an episode of acute cholecystitis or there is no link between the 2. However, due to increase in the study of infection with schistosoma with cholelithiasis, as observed in the present case, a lithogenic outcome of schistosomiasis secondary to the induction of chronic granulomatous and fibrocalcific deviations of the gallbladder and biliary ducts wall, seems undisputable. The patient’s clinical presentation, including the presence of gallstones, chronology of events, and pathologic findings, supports strongly the association among the cholecystitis and schistosomal infection.
Acknowledgment
Authors were grateful to Dr. Abd Al Wahid Yousuf A. Alneel, MD, Department of Histopathology, East Jeddah Hospital, Ministry of Health, Jeddah, Saudi Arabia for carrying out histopathological analysis in this piece of work.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 8, 2018.
- Accepted June 6, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.