


Abstract
Ovarian teratoma is a rare cause of autoimmune hemolytic anemia (AIHA) by warm antibodies, resistant to corticosteroid therapy. This also implies that ovarian teratoma should be included in the differential diagnosis of AIHA, whether or not associated with pregnancy. We present a case of a primigravida who presented with ovarian dermoid cysts and AIHA at 24 weeks of gestation. The patient received corticosteroids, intravenous immunoglobulin, rituximab, and multiple blood transfusions, with no significant improvement. Hemoglobin levels returned to normal only after laparoscopic ovarian cystectomy. Autoimmune hemolytic anemia caused by dermoid cyst is a rare condition especially in pregnancy. However, in light of similar case reports and review of the existing literature, we conclude that surgical excision should be considered when AIHA and ovarian teratoma coexist.
There may be several causes of autoimmune hemolytic anemia (AIHA). Rare causes of AIHA are tumors, including ovarian tumors,1,2 and these can be either malignant or benign.3,4 We present a case of AIHA which developed during pregnancy, associated with ovarian tumor. Autoimmune hemolytic anemia is IgG Mediated disease for that it is a serious condition for mother and fetus5 The mechanism of hemolysis in pregnancy has not yet been defined. Agarwal et al in 20036 discuss the pattern of such condition and reviewed their clinical course, he reviewed 20 cases of AIHA associated with dermoid cyst, 85% of them respond to cystectomy after failed corticosteroids and one under went cystectomy shortly after diagnosis who showed some response to steroid management. However, effective treatment in our case was post delivery tumor removal. Thus, it is important for obstetricians/gynecologists to know that teratoma is one of the etiologies of AIHA during pregnancy.
Case Report
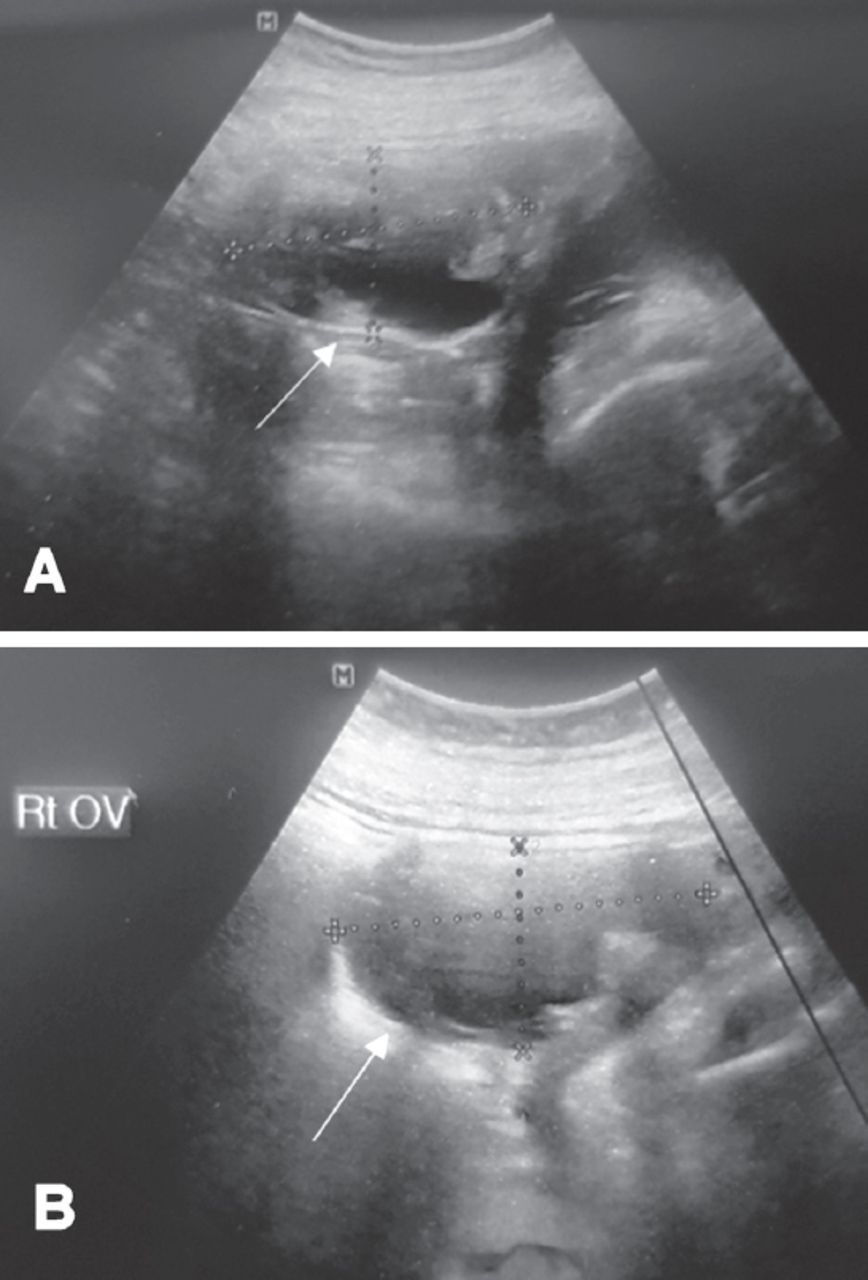
A 24-year-old, primigravida was referred to us at 24 weeks of gestation, as a case of AIHA, first diagnosed during pregnancy. Initially she was presented with fatigue and dizziness and low hemoglobin (Hgb) with no history of any medical illness or surgery. She had not been started on any new medications and had no family history of hematological diseases. Initial laboratory tests showed white blood cell (WBC) count 22.9 x 109/L, red blood cell (RBC) count 2.68 mcL, hemoglobin (Hgb) 7.7 g/dL (normal: 120-160 gm /L, platelet count 545000 (normal: 150-400X10A9 /L), reticulocyte percentage 18.63 (normal: 0.5-2.5%), lactate dehydrogenase (LDH) 567 U/L (normal: 125- 243U/L), and total bilirubin 44.1 (normal: 3.4-20.5 umol/L. Kidney function tests were within normal limits, and the direct Coomb’s test was positive. Viral serology, anti-nuclear antibodies, anti-double stranded DNA antibodies, anti-lupus, anti SS-A, anti SS-B were all negative. Ultrasound showed a normal fetus with size corresponding to gestational age. However, the maternal right ovary was enlarged, measuring 7.7 x 7 cm. A complex cyst measuring 6.7 x 6 cm was seen within the ovary, and was thought to be a dermoid cyst (Figure 1).
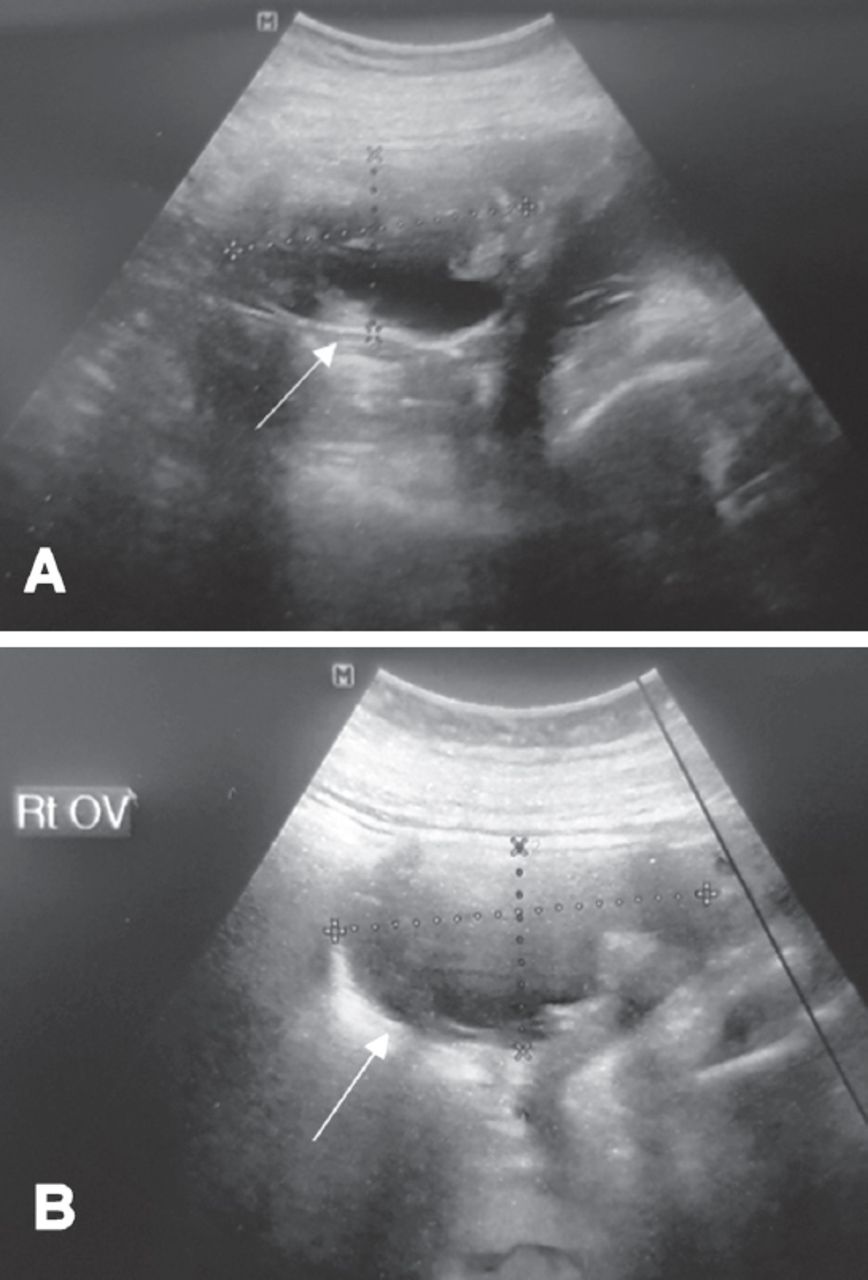
Right sided ovarian dermoid cyst.
She received high dose steroids (started by prednisolone 100 mg) with no significant improvement. Rituximab once a week four doses and intravenous immunoglobulin 3 doses were added, without any success. Hemolysis was refractory a trail of Azathioprine post delivery. Transfusion of multiple packed red blood cells (PRBCs) reached 44 units.
During follow up, the patient received a total of 44 units of PRBC for refractory low Hgb level. At 36-37 weeks of gestation, ultrasound revealed fetal pericardial effusion, and a slightly enlarged dermoid cyst.
Induction of labor was carried out and she uneventfully delivered a healthy baby vaginally. Postnatal echocardiography revealed no pericardial effusion and no other significant abnormalities.
Postpartum, Hgb level dropped from 11.0 g/dl to 7.0 g/dl. Azathioprine and prednisone, along with 6 units of PRBC were transfused. Two weeks later, the patient was seen on outpatient basis, with condition having worsened, with Hgb level having dropped further, to 6.1 g/dl.
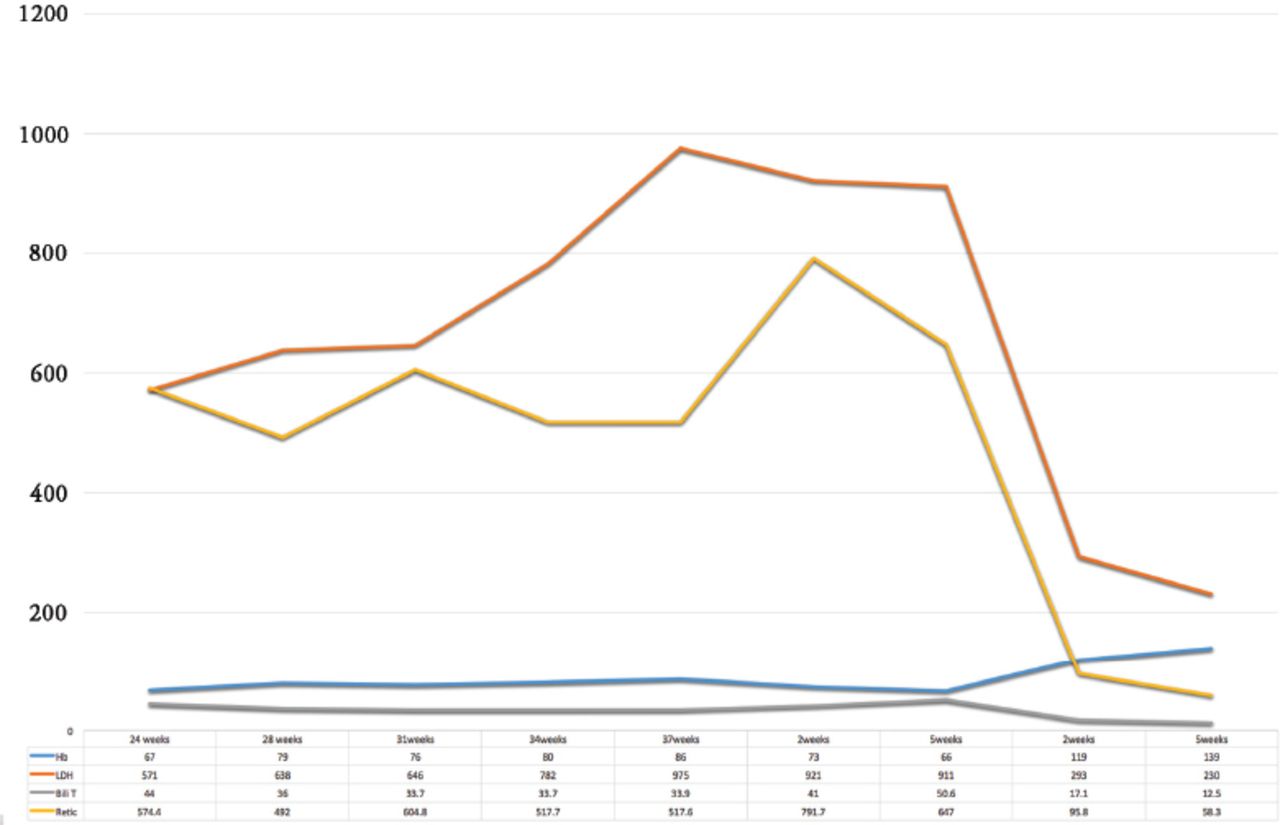
Laparoscopic right ovarian cystectomy was performed and intraoperative findings of right ovarian dermoid cyst were confirmed on histopathological examination. Postoperatively, she improved significantly; signs and symptoms of anemia reduced and Hgb level increased up to 13.8 g/dl, while LDH levels dropped to 169 (Table 1).
Timeline of summary of the case.
Discussion
Association between dermoid ovarian cyst and AIHA is still a rare phenomenon7 with a limited number of cases reported in the literature. Ovarian teratomas are relatively common, but the incidence of associated hemolytic anemia is low.
This phenomena was reported by West-Watson and Young8 but reported cases are still limited especially in pregnancy. There are different hypothesis describing the immunological reaction triggered by the tumor. Several reports support the hypothesis that the tumor produces antibodies against red blood cells. Antibody production seems to cease immediately after tumor removal in almost all reported cases.7
Glucocorticoids and splenectomy known as the mainstay of treatment of AIHA. In our case; however, it proved to be ineffective. An improvement was seen only after tumor removal.3-6 Payne et al9 in 1981 have carried out a literature review of cases reported as dermoid cysts with AIHA, and collected around 19 cases. Sixteen patients responded favorably to tumor removal alone. Negligible response to steroids was reported in 3 patients who required dermoid removal to achieve full response. Antibodies were reported to disappear in 2 weeks to 7 months after tumor removal, which may be considered as a confirmation of the association.9 Our patient was pregnant, and literature review did not reveal any case of AIHA due to a dermoid cyst, diagnosed in pregnancy. In fact, cases of AIHA during pregnancy, caused by factors other than dermoid cysts, have been reported late in pregnancy, and lay emphasis on good response to corticosteroids and blood transfusion.5
Autoimmune hemolysis in pregnancy complicates 1 in 50000 pregnancies.10 In most cases uneventful maternal recovery with good fetal outcome has been reported, except in a few cases caused by autoimmune diseases like systemic lupus erythematosus.10 Owing to a lack of similar cases in literature, maternal and fetal course was closely followed, with clinical monitoring of maternal condition by symptoms and laboratory investigations, and keeping a watch for possible fetal anemia. An obstetric ultrasound showed fetal pericardial effusion at 37 weeks of gestation. However, the fetus was born in a good condition, with normal echocardiography 2 weeks after birth. Unfortunately, the maternal condition did not improve and she required repeated blood transfusions post delivery. Laparoscopy dermoid cystectomy was carried out, after which, complete recovery of the mother took place (Figure 2).
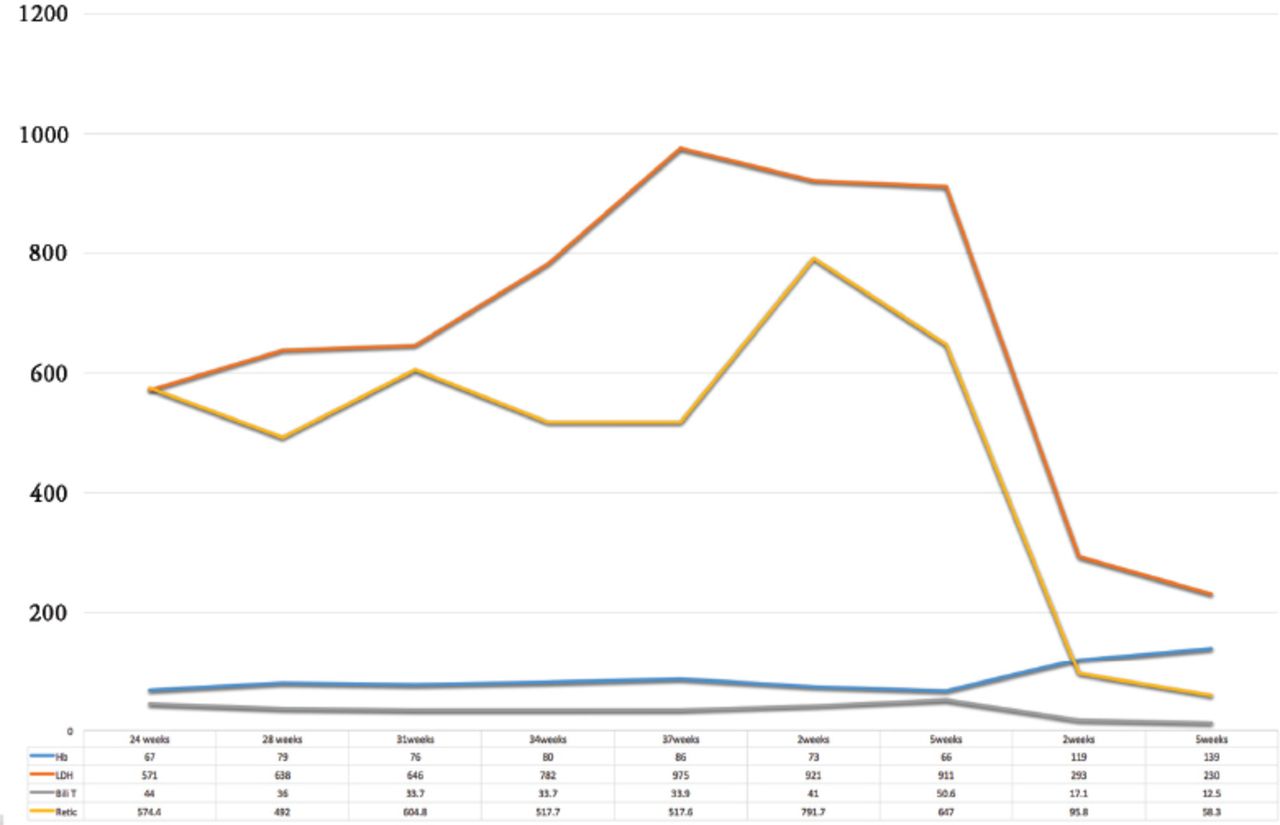
Laboratory results. Hb - hemoglobin (g/dl). LDH - lactate dehydrogenase (U/L), Bili T - total bilirubin, Retic - reticulocyte percentage
In conclusion, AIHA caused by a dermoid cyst is a rare condition. However, in light of similar case reports and review of the existing literature, it would be reasonable to conclude that in the presence of AIHA and ovarian teratoma, surgical excision should be considered. However, it should be kept in mind that this association may occur during pregnancy. Furthermore longer follow, up duration is needed to actually prove that the ovarian tumor resection led to persistent resolution of AIHA.
Acknowledgment
We would like to acknowledge Dr. Hytham Alsum, Consultant, Maternal Fetal Medicine, National Guard Health Affairs, Riyadh, Kingdom of Saudi Arabia and the Editage.com for the English editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company
- Received September 8, 2018.
- Accepted March 20, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.