


Abstract
Objectives: To re-draw attention to the unnecessary prescribing of antibiotics.
Methods: We monitored nasopharyngeal colonization by 3 potentially pathogenic bacteria, Streptococcus pyogenes, Streptococcus pneumoniae, and Haemophilus influenzae type b in 81 children between the ages of 6 and 7 years who attended the same primary school. The children’s health status was also monitored, without using antimicrobial treatment for healthy/asymptomatic carriers. Nasopharyngeal swabs were collected on 6 occasions during autumn months, from mid-September to mid-December 2016. The children who fell ill during the study were treated at the Ear, Nose and Throat Clinic, Sisters of Mercy University Hospital Center, Zagreb, Croatia.
Results: Four hundred and sixty-three nasopharyngeal swabs were collected. Each child had at least one positive swab result. Bacterial colonization with Streptococcus pyogenes had the highest colonization rate. During the study, 83% of the children were healthy/asymptomatic carriers with no clinical signs of disease, while 17% became ill. The statistical results showed that the increase in all examined bacteria was statistically significant.
Conclusions: Our study results showed that positive bacterial findings in nasopharyngeal swabs from clinically healthy carriers were not an indication for antibiotic therapy.
Nasopharyngeal (NP) colonization by potentially pathogenic bacteria (PPB), such as Streptococcus pyogenes (Group A streptococcus [GAS]), Streptococcus pneumoniae (SP), Haemophilus influenzae type b (Hib), Moraxella catarrhalis (MC), and Neisseria meningitidis (NM), is especially high in children under 5 years of age attending day-care centres,1-3 and common in children aged between 5 and 15 years.4,5 These pathogens can cause a wide spectrum of illnesses, from upper respiratory tract infection to invasive diseases, or the colonization can be asymptomatic.6-11 Children who are healthy/ asymptomatic carriers (HC) are a potential source of infections, and for that reason many pediatricians often prescribe antibiotics to them for fear of outbreak of a disease and its spread.12,13
Methods
This study monitored the incidence of NP colonization by GAS, SP, and Hib in 81 children between the ages of 6 to 7 years, and children health status, without using antimicrobial treatment for HC. Informed consent was obtained from all parents whose children had been included in the study.
The study protocol has been approved by the Committee on Ethics of the Department of Otorhinolaryngology and Head and Neck Surgery, Sisters of Mercy University Hospital Center, Zagreb, Croatia (EP-18818116-11). All procedures in this study, involving human participants, were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Nasopharyngeal swabs (NPS’s) were collected in the same primary school from the same number of children; 27 children from each of 3 classes, on 6 occasions, twice monthly, during the autumn months, following the summer holidays, from mid-September to mid-December 2016. No child had been vaccinated with Pneumoccocal vaccines or Hib vaccine before the study. These vaccines are not on the list of mandatory vaccines in our country, so parents decide whether to vaccinate their children or not. Standard microbiological procedures were used to identify GAS, SP, and Hib.14 The children who became ill during the study were treated and monitored at the Ear, Nose, and Throat (ENT) Clinic, Sisters of Mercy University Hospital Center, Zagreb, Croatia and had NPS’s collected in the acute phase of the disease, and 5 days after the end of antibiotic therapy.
Statistical analysis
Nasopharyngeal colonization of GAS, SP, and Hib, and all bacteria together showed a trend of growth during 6 points of swab collection.
GAS - growth trend is shown by the linear regression function y = 5.2 + 5.80 * x (y: GAS, x: time); the regression coefficient is statistically significant (t(4)=29.0, p<0.001).
SP - growth trend is shown by the linear regression function y = 6 + 3.29 * x (y: SP, x: time); the regression coefficient is statistically significant (t(4)=7.753, p=0.0015).
Hib - growth trend is shown by the linear regression function y =4.8 + 2.06* x (y: Hib, x: time); the regression coefficient is statistically significant (t(4)=7.060, p=0.0021).
All bacteria together - growth trend is shown by the linear regression function y = 16 + 11.14 * x (y: swabs, x: time): the regression coefficient is statistically significant (t(4)=34.883, p<0.001).
In the time period between the 6 NPS collecting, the number of children who fell ill was almost the same, thus, there were no statistically significant differences.
Results
A total of 463 NPS’s were collected; from 81 children at the 1st and 2nd visit, 76 children at the 3rd visit, 75 children at the 4th visit, 73 children at the 5th visit, 77 children at the 6th and final visit. Children who were out of school on the date of swab collection were absent for various reasons. Results showed that 83% of included children were HC’s, while 17% (13 children) became ill between visits.
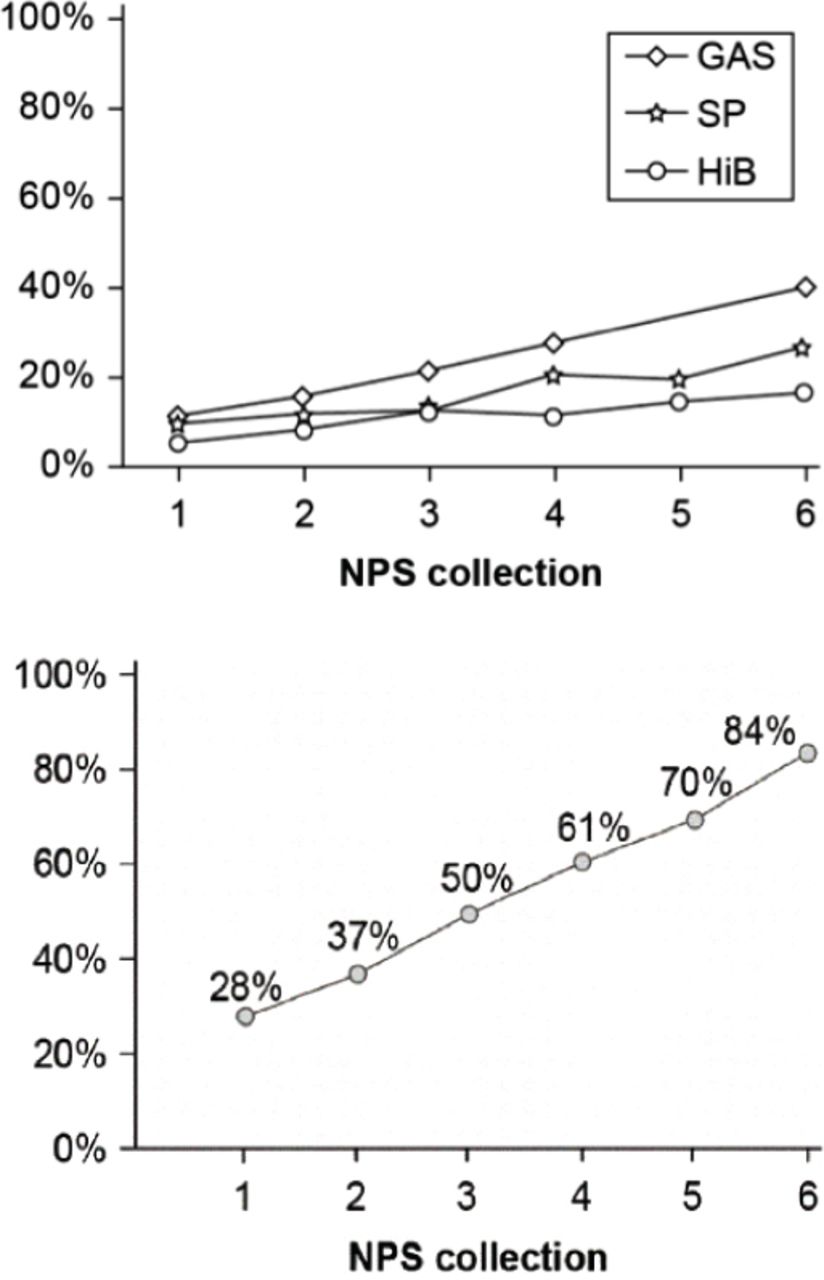
The lowest bacterial colonization was recorded in September, at the first swab collection visit (28% of children colonized by GAS, SP, and Hib), and it increased at each subsequent visit. Colonization by all 3 bacteria peaked at the end of the study, in December (Figure 1A, Figure 1B); 84% of children were colonized by GAS, SP, or Hib (Figure 1B).

Graph showing the A) colonization of GAS, SP and Hib at each NPS collection visit and the B) combined colonization of GAS, SP and Hib at each NPS collection visit. GAS - Group A Streptococcus, Hib - Haemophilus influenzae type B, NPS - nasopharyngeal swab, SP - Streptococcus pneumoniae
Group A streptococcus, SP, and Hib colonized and recolonized the nasopharynx of each HC at different time intervals. Each child had at least one positive NPS during the study. Most positive swabs had a single bacterium isolated (GAS, SP, or Hib), while 2 different bacteria were isolated from 9 NPS’s, and 3 bacteria in a single NPS (Table 1). Group A streptococcus was the most commonly isolated bacteria at all 6 time points, increasing from 12% at the first visit, to 40% at the final visit. Streptococcus pneumoniae increased from 10% at the first visit, to 27% at the final visit, and Hib increased from 6% at the first visit, to 17% at the final visit (Table 1, Figure 1A).
Number of present children, and the number and percentage (%) of isolated bacteria in a single nasopharyngeal swab during all 6 nasopharyngeal swab collections.
Before the onset of the disease 7 of 13 children were HC’s: 3 children were GAS carriers, 3 children were SP carriers, and one child was Hib carrier, without showing any clinical signs of disease (Table 2). The same bacteria that were detected before and during the disease were isolated in 3 HC’s, while a different bacteria was isolated in 4 HC’s (Table 2). At the beginning of the illness, a NPS was taken from all of these children at our ENT Clinic. The results showed that all of them had one bacteria in a single NPS and they underwent antibiotic therapy; 6 children had Streptococcal pharyngitis caused by GAS, 4 children had acute otitis media (AOM): 3 AOM caused by SP, one AOM caused by Hib; 3 children had acute tonsillitis/pharyngitis caused by Hib. The duration of antibiotic treatment was determined according to the clinical status of children and the antibiogram. A follow-up NPS taken 5 days after the end of antibiotic therapy showed normal flora (NF) in 8 children, who afterwards rejoined their classes. Group A streptococcus was re-isolated in 3 children who had Streptococcal pharyngitis, SP was re-isolated in 2 children who had AOM. In these children the antibiotic therapy was repeated. A follow-up NPS taken 5 days after the repeated therapy showed NF in all children, and they rejoined their classes (Table 2). At the next planed visit, 5 of 13 re-joined children were again HC’s without showing any clinical symptoms of disease. One bacterium was isolated in a single NPS in 4 children, and 2 different bacteria were isolated in a single NPS from one child. Since the study ended at the final visit, the number of children that potentially started to show symptoms of illness after that time point is unknown.
Review of 13 children who became ill during the study with diagnoses / Nasopharyngeal swab findings before disease onset, on disease onset, and after antibiotic therapy.
Discussion
Many cases of sporadic outbreaks of diseases in day-care center or schools have prompted antibiotic prescription to whole groups/classes of children in which the outbreaks occurred. Unfortunately, further follow-up swabs following the antimicrobial treatment showed bacterial recolonization in most children.1-5,12,13
Our study started at the beginning of the school year when children returned from summer holidays and lasted until the beginning of winter holidays (mid-September to mid-December 2016). The results showed a low incidence of NP bacterial colonization at the first and second swab collection visit. The number of carriers increased at each subsequent visit. The highest colonization rates were recorded at the final visit (Figure 1A, Figure 1B). The increase in NP bacterial colonization during the study occurred because bacterial transmission between children is much higher when they are at school in close contact with each other, as opposed to when they are on holidays. The statistical treatment of results of the bacterial NP colonization has shown that the increase in all examined bacteria during 6 NPS collections was statistically significant. The children who became ill during the study were treated at our ENT Clinic with antibiotic therapy, since PPB were isolated in NPS from each of them. It remains unclear why these children became ill during that period rather than earlier or later. This study monitored bacterial colonization, but not the invasiveness of carried strains. In comparison to other studies, our results did not show a significant difference.1-5,10-13 However, even though many studies related to NP colonization by PPB in children attending day-care centers/schools showed similar results, we have to be aware that the results of future studies may differ from ours. For that reason, we find that such clinical research should continue in order to determine uniform guidelines for the medical treatment of healthy carriers.
In conclusion, our 3-month study monitored the colonization of 3 PPB (GAS, SP, Hib) in nasopharynxes of children attending the same primary school, as well as their health statuses. Statistical evaluation of results has shown statistically significant increase of nasopharyngeal colonization by all 3 examined bacteria. Despite the large number of carriers, especially towards the end of the study (84%), disease outbreaks were sporadic in all 3 classes. Based on our research, we find that positive bacterial findings in NPS’s from clinically HC’s are not an indication for antibiotic therapy.
The results of our work are meant to help pediatricians in deciding whether or not to prescribe antibiotics to children who are HC’s.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 6, 2019.
- Accepted February 8, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.