


Abstract
Objectives: To examine the androgen receptor (AR) status in colorectal cancer (CRC) patients by the immunohistochemical method and to correlate the findings with all available clinicopathological parameters of prognostic significance.
Methods: Archival tumor samples were studied using immunohistochemistry for AR expression in 324 patients with CRC. Patients were diagnosed at the Pathology Department at a tertiary care Hospital, Al-Madinah Al-Munawarah, Saudi Arabia, between January 2006 and December 2017.
Results: There is a complete lack of AR expression in normal colonic mucosa; however, AR was expressed in 16 cases (40%) of colorectal adenoma. In CRC, AR expression was high in 118 cases (36.4%). There were no significant correlations between AR expression and gender, age, tumor histologic type, and tumor location. However, AR expression revealed a significant correlation with tumor size (p=0.026), tumor differentiation (p=0.047), American Joint Committee on Cancer (AJCC) staging (p=0.043), lymph node positivity (p=0.018), lymphovascular invasion (p=0.018), and distant metastasis (p=0.049). In univariate Kaplan-Meier survival analysis, there was a significant (p=0.002) difference in overall survival between AR positive and negative tumors in favor of the latter. In multivariate (COX) models, high AR expression (p=0.002), AJCC (p<0.001), and lymphovascular invasion (p<0.001) were the only significant independent prognostic indicators of overall survival in CRC.
Conlusion: Our study showed that the patients with higher AR expression had a significantly poorer survival rate, AR expression had the potential to be a prognostic marker of CRC.
The androgen receptor (AR) belongs to the group of nuclear receptors and functions as a transcription factor that binds to DNA and thus regulates gene expression. Androgens (mainly testosterone) are hormones that bind to AR and are essential for the development of the male reproductive system and secondary sexual characteristics.1 Some of the non-reproductive organ tissues of both males and females are also subject to androgen regulation.2 Due to its role in the development of the prostate, AR has been used as a primary target of endocrine therapy in prostate cancer (CaP). Inhibition of AR signaling has been reported to have major benefits for patients with CaP.3 Androgen receptor has been studied in detailed recently in relation to CaP from a molecular perspective4 as well as its expression in patients with diabetes,5 the role of stromal AR in the development and progression of CaP,6 and in drug discovery.7 Androgen receptor has also been thoroughly studied for its role in breast carcinoma;8,9 as well as in urothelial/bladder carcinoma.10,11 Moreover, some studies have addressed the role of AR in different organs and systems (example: penile carcinoma),12 the cardiovascular system,13 and fibrosarcoma.14 Similarly, the role of androgens has also been studied in the gastrointestinal tract and colorectal carcinoma (CRC) by a number of studies.15,16
The aim of this study was to examine the AR status in CRC patients by the immune-histochemical method and to correlate the findings with all available clinicopathological parameters of prognostic significance.
Methods
This retrospective study involved 324 cases of CRC diagnosed at the Department of Pathology, King Fahad Hospital, Al Madinah Al Munawarah, Saudi Arabia between January 2006 and December 2017. All clinical and histopathological data of the patients were collected from the patients’ medical records and included gender, age, tumor type, size, site, grade, lymphovascular invasion, lymph nodes status, metastasis stage, and the American Joint Committee on Cancer (AJCC) stages of CRC. Clinical and pathological data of patients are shown in Table 1. Forty cases of colorectal adenoma and 20 normal colonic mucosa cases were used as controls. The inclusion criteria was histologically confirmed invasive CRC cases, including CRCs cases with distant metastasis, whereas the exclusion criteria were in-situ lesions, recurrences, benign lesions, and metastatic lesions. All total colectomies, hemi-colectomies, and excision specimens were included in the analysis. The study did not involve patients’ personal information or any implication upon the management. Therefore, according to the principles of the Helsinki Declaration, no ethical approval was mandatory for this study.
The clinicopathological features of 324 colorectal carcinoma cases.
Immunohistochemical procedures
Tissue cores were extracted from archival blocks of the primary CRC and used in the construction of tissue miniarrays (TmAs) using Elkablawy and Albasri’s17 modified TmA technique as follows: a semiautomatic metal puncher with a 5 mm punch tip was used as a TmA manual kit to punch and extract the tissue cores from prewarmed paraffin blocks from the main donor tissue blocks. The cores were manually transferred, organized, and attached to a standard block mold with glue and filled with liquid paraffin to build TmA blocks. We then cut 4 micrometer-thick sections of tissue from the TmA blocks, mounted on poly-l-lysine-coated slides and subjected them to immunohistochemistry (IHC) using the Avidin Biotin detection system, as directed by manufacturer guidelines. Immunohistochemistry was carried out using an automatic system (Bench-Mark XT; Ventana Medical Systems, Inc., Tucson, AZ, USA). The antibody used was a rabbit anti-AR monoclonal antibody (diluted 1:100 in blocking solution; Clone SP107, Ventana Inc., Tucson, AZ, USA). A sample of normal prostatic tissue was used as a positive control for the anti-AR antibody. Negative controls were accomplished by replacing the primary antibody with serum.
Interpretation of immunohistochemical staining
Cells were considered positive for AR when distinct nuclear yellow to brown staining was identified. The immunostaining was reviewed independently, and the average score was taken. The level of AR overexpression was calculated by combining an estimate of the percentage of immunoreactive cells (quantity score) with an estimate of the staining intensity (staining intensity score) as follows. No staining was scored as 0; 1-10% of cells with positive staining were scored as 1; 10-50% as 2; 50-70% as 3; and 70-100% as 4. Staining intensity was rated on a scale of 0 to 3 as follows: 0=negative (no staining); 1=weak; 2=moderate; and 3=strong. The percentage and intensity scores were multiplied to produce a weighted score (WS) for each specimen. The final expression score was expressed as follows: ‘-’ for a WS of 0; ‘+’ for WS 1-3; ‘++’ for WS 4-6; and ‘+++’ for WS > 6. For statistical analysis, the cases that scored as ‘-’ and ‘+’ (low WS) were combined and then compared to the cases that scored as ‘++’ and ‘+++’ (high WS).
Statistical analysis
Statistical analyses were performed using the Statistical Package for Social Sciences version 22.0 for Windows (IBM Corp, Armonk, NY, USA). Frequency tables were analyzed using the Chi-square and Fisher’s exact tests to determine the association between the AR expression and the variable clinicopathological parameters. The cumulative patient survival was assessed by the Kaplan-Meier method. Finally, the long-rank test was used for comparison of the survival curves. In order to assess the value of AR as an independent factor independently associated with survival, multivariate survival analysis was performed using the Cox proportional hazards regression model controlling for confounding by the following variables: gender, age, tumor type, size, site, grade, lymphovascular invasion, lymph nodes status, metastasis stage, and the AJCC stages. In all tests, a p value of ≤0.05 was regarded as statistically significant.
Results
Androgen receptor expression profiles
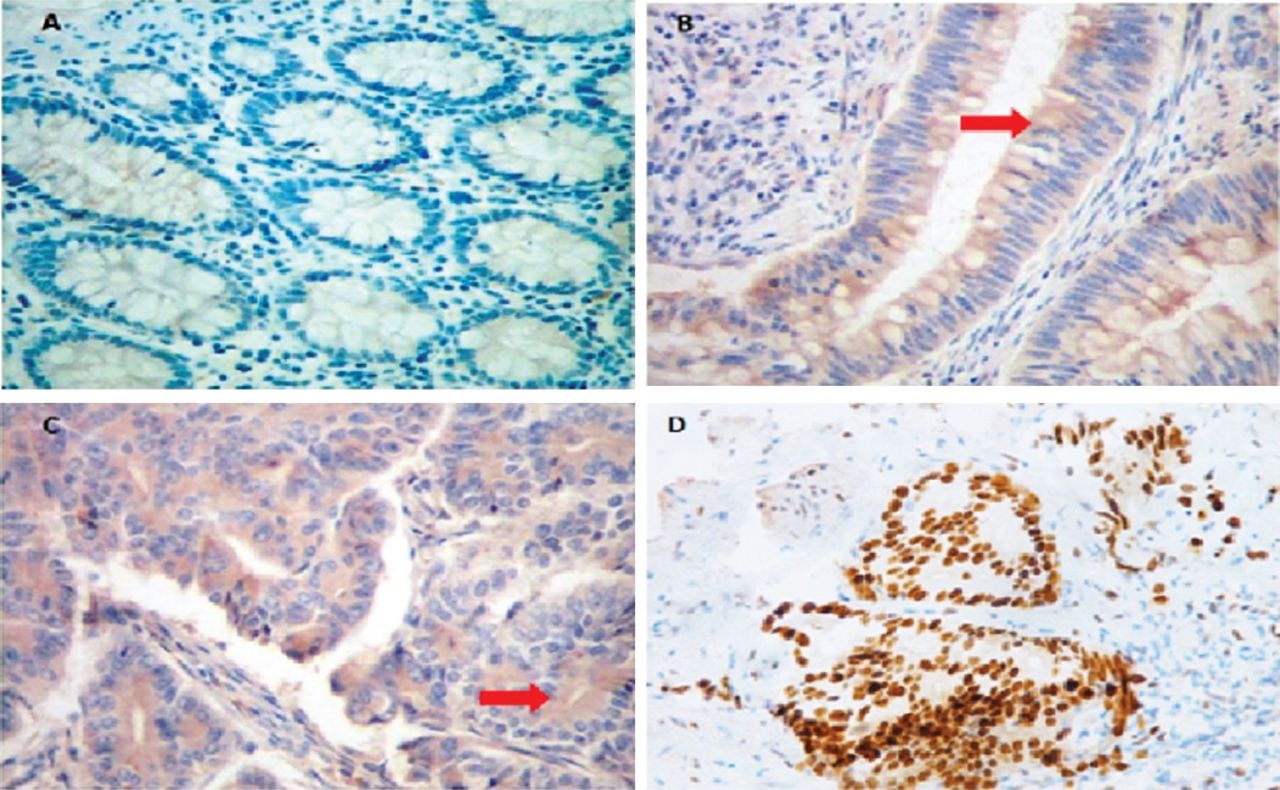
A complete lack of AR expression was shown in normal colonic mucosa; however, AR was expressed in 16 cases (40%) of colorectal adenoma. In CRC, AR expression was high in 118 cases (36.4%) and low in 206 cases (63.6%) (Figure 1).

Photomicrograph of different patterns of androgen receptor (AR) expression by immunohistochemistry in A) normal colonic mucosa showing a negative expression of AR, B) colorectal adenoma showing cytoplasmic expression of AR in the tumor cells, C) Colorectal carcinoma showing intense cytoplasmic expression of AR in tumor cells, and D) a control sample from prostatic adenocarcinoma showing intense nuclear expression of AR in the tumor cells. Arrows indicate cytoplasmic expression of AR.
Expression of androgen receptor and its correlation with clinicopathological variables
No significant correlations were shown between AR expression and gender, age, tumor histologic type, or tumor location. However, AR expression revealed a significant correlation with tumor size (p=0.026), tumor differentiation (p=0.047), and AJCC staging (p=0.043), as well as metastatic parameters (exmaple: lymph node positivity; p=0.018), lymphovascular invasion (p=0.018), and distant metastasis (p=0.049). The relation of AR expression to clinicopathological variables as summarized in Table 2.
Relation of androgen receptor immunoexpression to clinicopathological parameters.
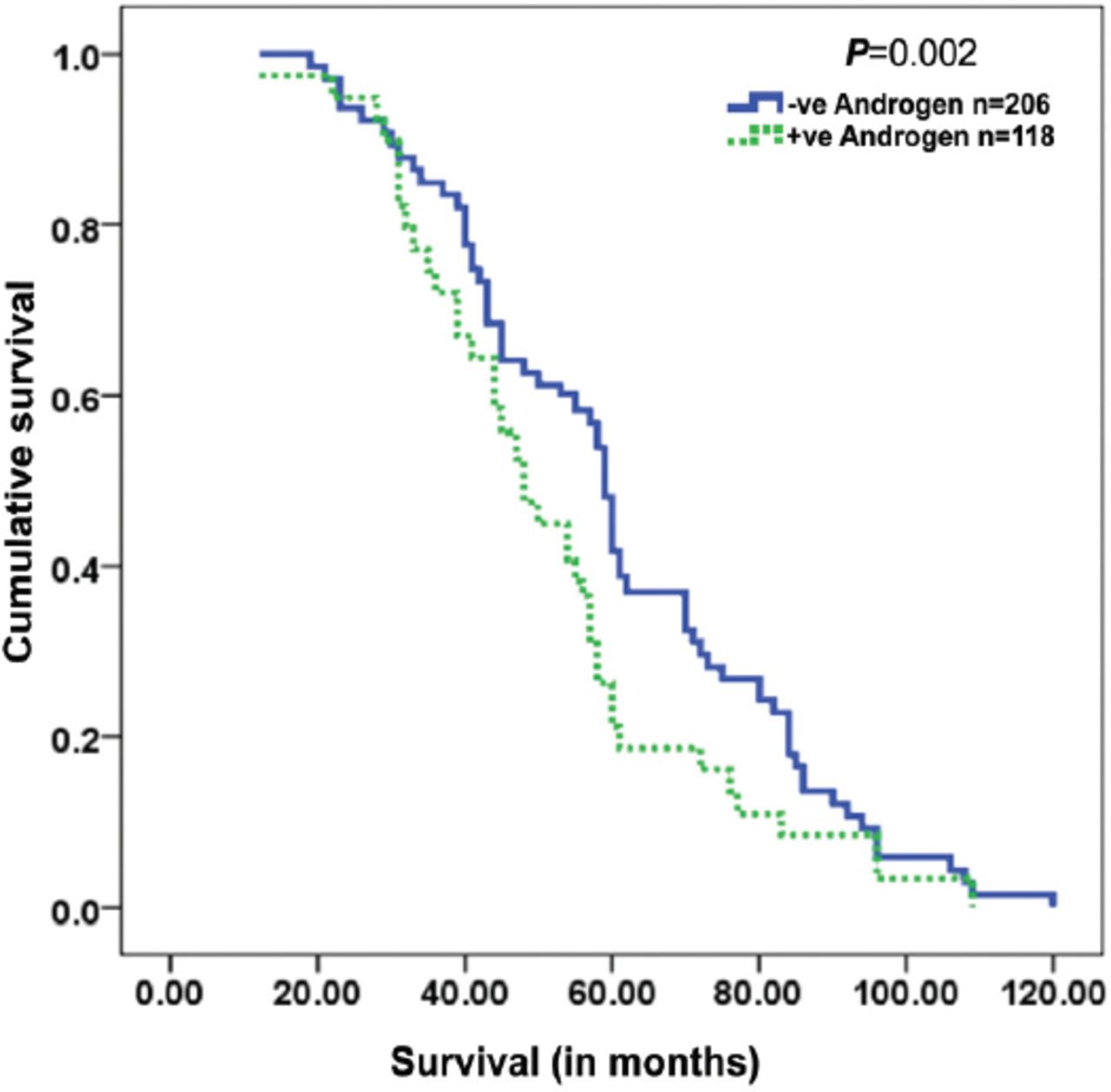
The significant features associated with survival for the patients are summarized in Table 3. The survival curve for the AR immunoprofile is provided in Figure 2. Significantly short survival was observed in patients with high AR overexpression compared to patients with low AR overexpression (p=0.002). High AR expression (p=0.002), AJCC classification (p<0.001), and lymphovascular invasion (p<0.001) were the only significant independent prognostic indicators, as calculated by multivariate analysis of the Cox regression model.
Test statistics for equality of survival distribution for prognostic factors examined in 324 colorectal carcinomas. A multivariate-Cox proportional hazards regression approach to the overall survival.

Kaplan- Meier survival curves showing significant overall lower survival functions for high AR expression in colorectal cancer cases.
Discussion
Androgen receptor is a receptor belonging to the group of nuclear receptors. Androgens are essential for the development of the male reproductive system and secondary sexual characteristics1 and morphogenesis of male reproductive organs (the epididymis, seminal vesicle, prostate, and penis) are determined by androgens during embryogenesis.18 These androgen-dependent signals and downstream events are crucial not only for developmental processes but also processes of diseases, such as hypospadias and CaP.18 Aberrant AR activity is promoted by irregularities of the binding partner or mutations, which can present as a number of clinical manifestations that include androgen insensitivity syndrome as well as CaP. In the latter case, treatment generally involves deprivation therapies interfering with AR action.19 Due to the main function of androgens in the development and growth of genital organs, including both primary and secondary sexual properties, AR has been extensively studied in a number of related disorders to block the effects of androgens, especially neoplasia, such as urothelial cancer,20-24 penile carcinoma,12 as well as CaP.9 Various results have shown that AR has distinct and contrasting roles in each cell type within many hormone-related tumors. Androgen receptor has been found to be a stimulator in bladder, kidney, and lung metastases and as a suppressor in prostate and liver metastases.25
Extensive work on AR has been carried out particularly concerning CaP. Androgen receptor has been used as a primary target of endocrine therapy in CaP.26 A number of excellent reviews have been published in the literature regarding the role of AR in CaP.14,16 Overexpression of AR in CaP has also been recently studied in diabetes mellitus type 2, due to reported poor survival of CaP diabetic patients.5 The inhibition of AR signaling has been shown to have major benefits for patients with CaP.3
As mentioned, AR has also been significantly studied in urothelial cancers, as these are more common in males than in females, and preclinical evidence points toward correlation of the activation of AR in urothelial cancers.10,20 Thus, the expression of AR in non-muscle-invasive bladder cancer was studied, which predicted the preventive effect of androgen deprivation therapy on tumor recurrence.23
Iacopetta et al,27 from Italy, published a detailed review on the role of AR in breast carcinoma in light of recent study indicating an emerging hormonal target in breast cancer that has clinical benefits in both estrogen receptor (ER) positive and ER negative tumors. Due to failure of hormonal and herceptin therapies in triple negative breast cancers (TNBC), a special interest has been shown in anti-androgen therapy in the AR positive TNBC cases. Safarpour et al28 found more than one-third (36%) AR positive cases in 50 TNBC cases and have thus recommended a routine assessment of AR in TNBC. Although some scientists have reported that AR expression predicts a decreased survival in the early stages of TNBC,29 phase 2 clinical trials on anti-AR therapy have shown benefits to some degree in AR positive TNBC.30,31
The latest GLOBOCAN 2018 update reported that the world cancer burden was 18.1 million new cases and 9.6 million cancer deaths in 2018.32 Colorectal cancer is one of the leading cancers in the world today, fourth in the rank of incidence rate; it is second only to lung cancer in cancer mortality rates.33 Colorectal cancer incidence appears to be lower in developing Asian and African countries as compared to the developed countries, and the KSA belongs to a low CRC incidence region. However, CRC is still the second most common cancer, after, according to the latest Saudi cancer registry.32 According to the latest regional hospital pathology-based study from Madinah, CRC was diagnosed in an advanced stage in the majority of case.34
Due to the high prevalence of CRC in the western world, as well as globally, extensive study is in progress to learn more on CRC regarding its prevention, diagnosis, and management. Some of the latest studies focused on improved detection methodologies (stool analysis for genetic changes), prediction of recurrence (identification of genes associated with growth and spread), immunotherapy, BRAF mutation target therapies, new drugs, and palliative care.35
For example, a UK-based study of a large number of patients (n=2624) analyzed the ploidy and digital tumor-stromal morphometry. This study concluded that these novel biomarkers could identify risks for recurrence and mortality in CRC patient sub-populations and could be helpful in the choice of adjuvant therapy of these CRC patients. This study was based on the methodology of automated digital imaging systems and analysis of microsatellite instability of DNA extracted from paraffin-embedded tumor tissue.36 However, despite these advanced techniques and markers that have been studied recently, comparatively less study was found in relation to hospital and patient-based studies for AR in the western world, and no data was available on AR in the CRC patient population in this country and region.
To find some study on hormones and their receptor status in CRC-including ER, PR, steroid, and glucocorticoid receptors-research had to be examined from almost half a century ago. In 1979, Alford et al37 from the USA, studied only 33 patients and concluded that some large bowel cancers might be endocrine dependent. They found AR in approximately 26% of the cases. In 1980, Mehta et al38 worked on chemically induced CRC in rat models and suggested that gender steroids were involved in carcinogen-induced colon tumorigenesis and that the action was mediated by their association with gender steroid-specific receptors. Similarly, Izbicki et al39 worked on experimentally induced colon carcinogenesis in rat models, albeit specifically studied the AR. They concluded that the carcinogenesis of CRC was only mildly affected by any manipulation of androgens. Scientists from M.D. Anderson Cancer Center, USA, working on colon cancer cell lines suggested that estrogen and glucocorticoid hormones might play an important role in the growth of colon carcinoma cells; in contrast, androgen and progesterone hormones appeared to be less relevant in CRC carcinogenesis and growth.40
The first significantly large patient-based study on AR was published from France in 1991. In a hospital patient cohort of 94 patients, they found AR in 98% of normal large bowel mucosa and 96% of CRC mucosa.41 However, they commented that the elevated AR in normal mucosa was not related to any known function of androgens in the digestive tract. Additionally, study from Brazil found complete negativity of AR in both normal and tumor mucosa. This study was only 22 CRC cases, and the methodology performed was a charcoal dextran assay.42
In contrast, this present study included 324 CRC cases, along with 40 cases of colorectal adenoma and 20 cases of normal mucosa as controls. A complete absence of AR was found in the normal mucosa; however, 40% of cases of adenoma revealed 40% AR positivity. Some level of positivity was found in all the CRC cases (example: high activity in approximately one-third of the cases and low activity in the remaining two-thirds).
These results are in the middle of almost all-positive AR results by Meggough et al41 from France and Brentani et al42 from Brazil. Explaining these contrasting results is difficult; however, the possibilities include the differences in methodologies, such as hybrid ligand methodology for AR measurement43 and charcoal dextran assay by Brentani et al.42 However, recent study utilizing the latest methodologies at genetic levels in vivo and vitro raises the possibility of different types of AR (membranous and cytoplasmic types).39 The membranous type of AR appears to trigger a strong apoptotic response.44 This same group of scientists, extending the study in the field of AR in CRC, have concluded that AR activation inhibits both in vitro and in vivo survival signals.45 These differences have also been addressed on the basis of altered expression of AR isoforms in CRC.46
Regarding the correlation of AR expression and various clinicopathological parameters in this present study, a significant correlation of AR expression was found with tumor size, differentiation, AJCC stages, and metastatic parameters, raising the possibility that AR positivity in CRC is an indicator of aggressive behavior of the tumor as well as its metastatic potential. Unfortunately, no study of this type and caliber could be found in recent or remote literature after extensive study. Similarly, a significantly short survival was found in patients with high AR overexpression; the independent prognostic markers were found to be high AR expression, AJCC stages, and lymphovascular invasion.
In conclusion, AR expression was performed in a large cohort of CRC patients, utilizing an immunohistochemical technique on microarray samples. Significant correlation of high AR expression was found with a number of clinicopathological and prognostic parameters, including short survival. Similar studies should be performed to validate these results. These studies could help scientists to develop better therapeutic approaches to target AR-mediated signals and better fight AR-sensitive cancers.
Acknowledgment
We gratefully acknowledge the Deanship of Scientific Research, Taibah University, Al Madinah Al Munawarah, Kingdom of Saudi Arabia, for their constant encouragement and support. We would also like to thank Scribendi (https://www.scribendi.com) for the English Language editing of the manuscript.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 12, 2019.
- Accepted July 11, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.