


Abstract
Objectives: To examine the influence of emergency department (ED) waiting time estimate provision on the satisfaction of patients.
Methods: This was a randomized controlled trial at King Abdulaziz Medical City, Riyadh, Saudi Arabia between September 2017 and May 2018. It included 18 to 70 years old Arabic-speaking acute care patients. After being divided into 2 groups, the intervention group alone was provided waiting time estimates. Both groups answered 2 questionnaires evaluating their satisfaction and illness perception before and after seeing a doctor.
Results: One-hundred patients were included. No significant difference found in waiting time satisfaction scores between groups (intervention (5.92/10±3.13), control (5.45/10±3.38), p=0.476). Demographics and illness perception had an insignificant impact on satisfaction. Waiting time estimate was preferred by most participants (70%).
Conclusion: Providing waiting time estimation did not affect satisfaction but was preferred to have in the ED by most.
Emergency departments (EDs) have an essential role in the provision of medical care to critically ill patients. The increasing demand for health care services due to rising populations and limited availability of primary care contributes to busy EDs.1 These factors have led to long waiting times among EDs internationally, including Saudi Arabia where this study was conducted.1 Another determinant of hospital overcrowding is providing medical care for aging and critically ill patients. The pronounced increase in complex diseases may result in ED boarding, which occurs when patients stay in the ED even after being admitted to inpatient services.1 With increased boarding of inpatients in the ED, the capacity to see new patients in the ED is decreased and often ED waiting times increase.1 Patients’ satisfaction is influenced by waiting time which also reflects the quality of services at the hospital. Increased waiting times could lead to increased stress and frustration among patients and healthcare providers in addition to increasing the number of patients who leave without being seen (LWBS).1,2 A previous study on ED patients suggested that patients’ satisfaction could be enhanced by providing estimates of the expected waiting time.3 A study in the United States (US) supports this recommendation, as the majority of patients included would prefer the presence of a time tracker display that estimates the time a patient has to wait before being seen by a physician.4 After the provision of waiting time estimates, this study analyzed patients’ satisfaction with their ED waiting time and checked whether it was affected by their demographic variables or perceived severity of illness. The purpose of this study was to investigate whether providing an estimation of the waiting time affects patients’ satisfaction and perception of waiting times in an adult ED.
Methods
This was a randomized controlled trial conducted in King Abdulaziz Medical City (KAMC), Riyadh, Saudi Arabia an academic tertiary care center with approximately 17,0005 adult ED visits per month. The ED uses the Canadian Triage and Acuity Scale (CTAS) to prioritize patients. Canadian Triage and Acuity Scale classifies patients in 5 levels of acuity from most critical, CTAS level one, where immediate life-saving intervention is required, to level 5, which is a non-urgent, stable condition without anticipated resources, except oral or topical medications.6 In the KAMC ED, CTAS levels 1 and 2 patients were immediately sent to the resuscitation unit, and level 5 patients were sent to an urgent care clinic. Triage was carried out by the nursing staff at the reception. Most CTAS levels 3 and some level 4 patients were sent to beds in an acute care unit. Canadian Triage and Acuity Scale level 3-4 patients were assessed by a triage physician immediately after they register and based on their ambulatory status and their potential need for care in a stretcher will determine whether patients will be assigned to the acute care unit or an ambulatory rapid assessment and management unit. Patients aged 18 to 70 years old and had a CTAS level of 3 or 4 who were assigned to the acute care unit were eligible for the study. The study excluded non-Arabic-speaking patients. When the study investigators were available, a sample of every other patient was taken. After obtaining written informed consent, patients were consecutively allocated to either the control or intervention groups. Both groups were asked to complete questionnaires before and after being seen by the ED doctor. A waiting time estimate was given to the intervention group only. To detect a difference of 10% in satisfaction scores with a 95% confidence level and 5% precision for a population of 17000, a sample of 70 patients was required. We included 100 patients to improve the robustness and account for possible missing data.
Data were collected after obtaining an approval at the Institutional Review Board from King Abdullah International Medical Research center. Data were collected using 2 questionnaires (Appendix 1) by the coinvestigators who enrolled patients during morning, evening, and night shifts and during workdays, weekends, and holidays to limit the effect of convenience sampling biases. The first questionnaire was given to patients at their assessment time in the triage area. The first questionnaire, which was adapted from a previous study,4 collected patients’ demographics, education level, acceptable waiting hours, perceived severity of symptoms, level of concern about symptoms, number of each patient’s ED visits, and their preference for the presence of a time tracker. The questionnaire was translated into Arabic and validated by a panel of experts in addition to a pilot study of 20 patients. After obtaining consent from patients and answering the first questionnaire, the coinvestigators only informed the intervention group with a time estimate. For the purpose of this study, the waiting time was defined as the duration from the time of registration in the ED to the time the patient was seen by the treating physician. Time estimates were determined using the average time needed to see previous patients during the same shift as obtained from the hospital information system. The second questionnaire was given to both groups after they had been seen by a doctor in the acute care unit. This questionnaire collected patients’ satisfaction and their perception of their waiting time.
Statistical analysis
Data analysis was carried out using the Statistical Package for Social Sciences, version 21.0 (IBM Corporation, Armonk, NY, USA), and a p-value of less than 0.05 was considered statistically significant. A beta error rate of 20% was chosen while calculating the sample size, and this resulted in an 80% statistical power. Data were presented as the mean (M) and standard deviation (SD), which was determined after the data collection for continuous variables, including age and waiting time. Percentages were used to describe categorical variables. Independent t-test was used to compare independent categorical variables with dependent continuous variables. Spearman’s rank coefficient was used to determine correlations.
Results
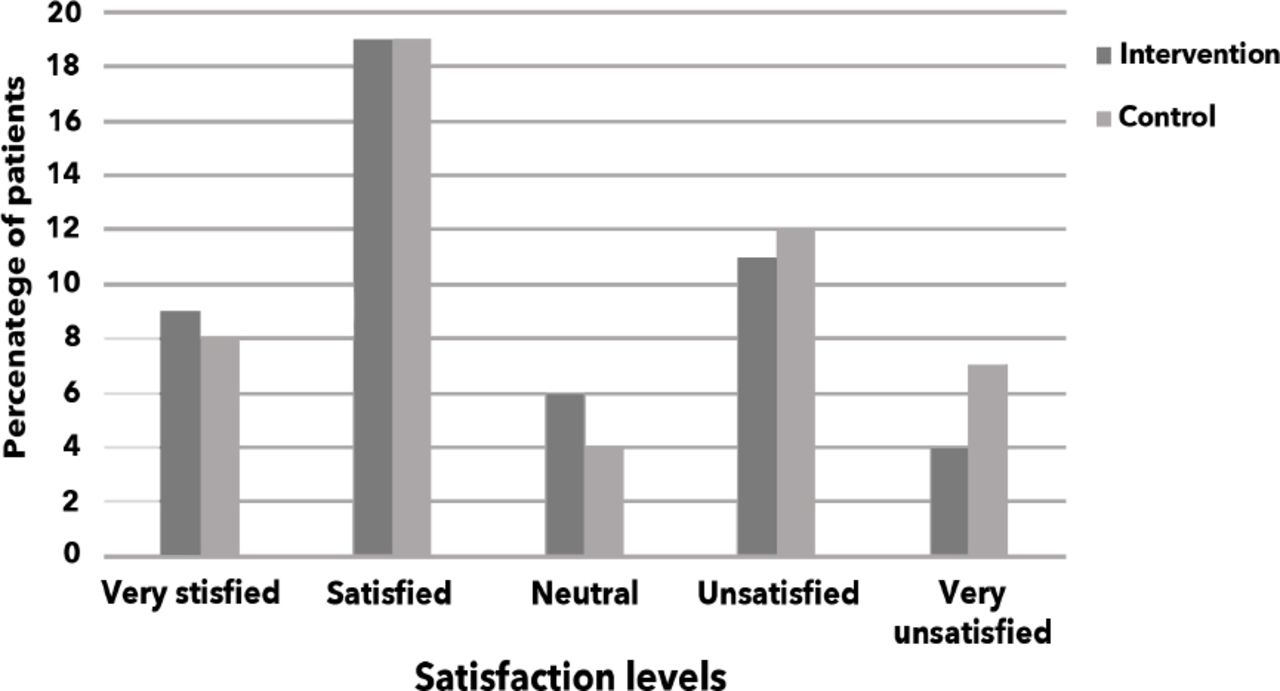
The study included 100 patients. The mean age of the sample was 38 years old females (67%). Demographics of the study sample and their perception of illness severity are shown in Table 1. Forty-one percent of patients reported that this was their first visit to an ED, while 28% have come 2 to 3 times before this visit. The presence of an ED waiting time display was preferred by 70.6% of patients, while 13.7% did not want a display, and 15.7% were unsure. The mean waiting time for the study sample was 70.54 minutes (min) (SD=41.73). The mean difference between the actual and estimated waiting times (actual-estimated) was -3.86 min (SD=41.11). Fifty-one patients were assigned to the intervention group and were given their estimated waiting time, and the remaining 49 patients were included as the control group. The characteristics of both groups were comparable. Statistical difference was not significant between the 2 groups for the perception of illness, frequency of ED use, their actual waiting times, or preference for knowing their expected waiting times at baseline. Patients’ satisfaction with their waiting times is shown in Table 1. Providing the estimated waiting times was not associated with a significant change in patient satisfaction with waiting times t (97)=0.715, p=0.48 (Figure 1). This was consistent within the subgroups of gender, age, education level, perception of illness severity, and level of concern. Providing the estimated waiting time did not significantly alter the patient satisfaction when subgroups with a short (<60 min), medium (60 to 90 min), and long (>90 min) waiting times were examined. Results were the same when Likert scale data were analyzed using nonparametric tests.
Patient demographics and perception of illness severity (N=100).

Patients’ satisfaction with their waiting time in the intervention and control groups.
There was a significant negative correlation between patients waiting time and satisfaction (rs=-0.35, p=0.0004). However, there was no significant correlation between satisfaction with waiting time and age, gender, education level, perception of disease severity, or level of concern.
Discussion
This study shows that the majority of ED patients prefer knowing their expected waiting time. Despite this preference, knowing their expected waiting times did not significantly alter their satisfaction with their waiting time. A previous survey study in the same ED found that waiting time was the only modifiable factor independently associated with patient satisfaction and suggested that providing a time estimate may, therefore, improve patient satisfaction.3 A study in an ED surveyed patients about their preference for having their waiting time estimates available also found that a majority (63%) preferred having their ED waiting time estimates.4 Another study in the US found that neither patients’ satisfaction with their waiting times nor the overall rating of their emergency department visit improved after an intervention that included providing waiting time estimates.7 However, both satisfaction scores were improved when comparing patients to whom delays were communicated to those whose delays where not communicated.8
While there are limitations to the meaningfulness of subjective survey questions,9 we feel that the reproduced finding that the majority of patients have a preference for the provision of waiting time estimates should not be discounted. It is possible that simply knowing the expected waiting time might not be enough to change patients’ perceptions and improve their experience. Additional steps to adjust expectations, reduce uncertainty, or improve feedback may be required to reach the desired effect. The discrepancy between expected actual waiting times (the disconfirmation model) has been shown to improve customer satisfaction in other service industries.10 Although few retrospective studies in EDs suggested that satisfaction increases if performance on waiting time exceeds the patients’ expectations, we have not found any prospective evaluations of this model in the healthcare setting.11,12 Improving feedback while waiting by showing progress or activities being performed has also been demonstrated to improve satisfaction in other industries.13,14
Study limitations
Our study’s main strengths were that it was appropriately powered, used a validated questionnaire, and had a random intervention assignment. However, it was conducted in a single center and used convenience sampling. We also excluded non-Arabic speaking patients and patients over 70 years old. Our sample’s level of education was relatively low. These factors may limit the generalizability of our findings. Future repetition of the study in different settings may help address these concerns. Further research on other mechanisms to improve the waiting time experience in EDs might further clarify which interventions are the most useful for improving patients’ satisfaction.
In conclusion, this study shows that despite the clear preference for patients to know their expected waiting time, providing this time estimate has no significant impact on patients’ satisfaction. However, given the limitations to the generalizability of the results, we recommend that this study be repeated in different cultural settings to assess the effect of waiting time estimates on the satisfaction of ED patients.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 27, 2020.
- Accepted June 24, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.