


Abstract
Objectives: To investigate the relationship of the neutrophil lymphocyte ratio (NLR) and the platelet lymphocyte ratio (PLR) with lung involvement and total lung severity score (TLSS) in computed tomography (CT) of patients with coronavirus disease -19 (COVID-19) and to evaluate their clinical usability.
Methods: Basic laboratory, clinical features and imaging data of patients was obtained by examining the file and archive records of our hospital. According to the findings of lung CT scan at the time of diagnosis among COVID-19 patients, 2 groups were formed.
Results: The NLR was 2.22±11.15 and the PLR was 142.77±387.10 in patients with COVID-19 pneumonia. The NLR was 1.88±7.47 and the PLR was 130.65±203.6 8 in patients without COVID-19 pneumonia. The differences in the NLR and the PLR were determined to be statistically significant between the 2 groups. A positive correlation was observed between NLR and PLR (r=0.225, p=0.010) and TLSS (r=0.244, p=0.005).
Conclusion: This study showed that the NLR and PLR values can be 2 inflammatory markers that can be used to evaluate lung involvement and disease severity in COVID-19 patients. At the time of initial diagnosis and during follow-up, these markers can give an idea in terms of prognosis, together with other clinical findings and markers.
Pathogenic viruses in the coronavirus family have caused major epidemics in the past 20 years.1-3 Coronavirus disease -19 (COVID-19) was identified as a severe acute respiratory syndrome coronavirus -2 (SARS-CoV-2); the World Health Organization (WHO) has accepted COVID-19 to be a pandemic.4-7 This disease is classified based on the severity of its clinical symptoms. While COVID-19 generally progresses with asymptomatic or mild-to-moderate symptoms, sometimes it can result in respiratory failure, multiple organ disfunction, or even death.8 Thorax computed tomography (CT) scan, which is used to diagnose the disease and determine the severity of lung involvement, plays a key role in clinical management. While the basal lower lobe of the lung is shown to be affected in CT in the literature, the most frequent patterns seen in a thorax CT are ground glass opacities, paving stones, consolidation, inter lobuler septal thickening, a pleural band, and a reticular pattern.9
There is a large number of studies on thorax CT focusing on the lung lobes and segments; these are used to evaluate the prognosis and clinical course of the disease by creating a total lung severity score (TLSS).10-13 Moreover, indicators, for instance, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and leukocyte, ferritin, and D-dimer levels, are studied in the laboratory to evaluate the period during which the infection is active. In recent studies, these markers have been shown to be related to the course of the disease and its prognosis. Throughout the duration of the disease, neutrophilia, lymphopenia, and variable platelet levels can be seen.14 Neutrophils and platelets, which are among the immune system components found in the complete blood count, have a key role in host defense. The active cells cause the secretion of cytokines, which lead to the activation of these cells and other defense system cells. In this process, apoptosis of lymphocytes results in lymphopenia.15-17 As a result of this vicious cycle, the number of neutrophils, platelets, and lymphocytes changes, as do their ratios to each other. Lately, the neutrophil lymphocyte ratio (NLR) and the platelet lymphocyte ratio (PLR) have evolved into the most frequently used markers in infectious diseases. In some studies, these markers were reported to be related to the intensity of the COVID-19.18-22
Computed tomography is expensive and includes x-rays. In this study, we aimed to evaluate the use of cheaper and more effective markers, NLR and PLR, in detecting lung involvement and severity in COVID-19 patients, and their usability in routine clinical workflow by comparing them with CT findings.
Methods
Our study used real-time polymerase chain reaction (RT-PCR) to evaluate the nose and throat samples of 215 patients that were determined with COVID-19 between March 10, 2020 and June 1, 2020.This study was consistent with Helsinki Declaration. After taking the Instutional Reviewer Board approval from our local ethical committee; basic laboratory, clinical features, and imaging data of the patients were obtained by examining the files and archive records of Yunus Emre State Hospital, Eskişehir, Turkey.
The patient groups who was under the age of 18, had any systemic disease and did not have the lung CT scan, was not included in the evaluation. Patients who were found to have developed super infection during clinical follow-up were excluded from the evaluation as they may cause errors in the statistical evaluation. We included only COVID-19 patients in our study to determine whether NLR and PLR could be a marker to detect lung involvement and severity of COVID-19.
According to CT scan findings at the time of initial diagnosis, 2 groups were constructed. Group 1 consisted of cases with 131 COVID-19 pneumonia on CT findings. Group 2 consisted of 84 cases without COVID-19 pneumonia in their CT findings. Total lung severity score was obtained in group one from the data reported in the literature. The TLSS showed involvement ranging from 0-4. Lung involvement patterns of score: 1 (0-25%), score: 2 (25-50%), score: 3 (50-75%), and Score: 4 (75-100%) were accepted as involvement of each lobe. The total score was 20.13
In group one, the TLSS was calculated by evaluating the involvement levels of cases with COVID-19 pneumonia. Furthermore, the lung involvement patterns and distribution of the affected lobes were determined in the group. In the laboratory data, complete blood count, CRP, ESR, ferritin, and D-dimer levels were examined and NLR and PLR were calculated. Finally, the laboratory and imaging findings were compared between the 2 groups.
Thorax CT scan was implemented on a 16-detector CT scanner (Emotion; SIEMENS). All patients were scanned in trendelenburg position. Computed tomography images were then collected throughout a single inspiratory breath-hold time. The examining array was from the top of lung to first lomber vertebral body level. Thorax CT scan parameters: x-ray tube parameters 120KVp, 350mAs; rotation time of -0.5 second; pitch -1.0; section thickness -5mm; intersection space -5mm; supplementary reformation with sharp coil kernel and a slice thickness of 1.5 mm
The complete blood count have been implemented in the equal tester, Mindray BC-6200, which is regularly controlled each month in the chief laboratory of our hospital. Standard tubes with stable amount of ethylenediamine–tetraacetic acid have been used. The white blood cell, neutrophil, and lymphocyte counts were archived and the NLR was measured from these markers.
Statistical analysis
The analysis of our study was performed using the Statistical Package for Social Sciences (IBM Corp., Armonk, NY, USA). Results were presented as mean±standard deviation (SD) or median (minimum - maximum), mean while categorical variables were indicated as number (n) and percent (%). Homogeneous distribution of the groups was assessed using Kolmogorov-Smirnov test. Homogeneous distribution parameters were evaluated using the Student t-test, one-sided ANOVA test in independent groups, Tukey honestly significant difference (HSD) test was used in the inter-group post-hoc evaluation, non-homogeneous distribution parameters were evaluated using the Mann-Whitney U-test, while categorical variables were reviewed by Chi-square test. The Spearman’s correlation test was used for correlation analyses. The comparison of sensitivity and specificity was evaluated by receiver operating characteristic (ROC) curve graphics. Stepwise linear regression was carried out with the dependent variable TLSS and independent variables NLR, PLR and the others parameters. A p-value <0.05 was considered significant.
Results
The median age of the COVID-19 cases was 44.6±16.0 (range: 18-83); 102 (47.4%) of the patients were women and 113 (52.6%) were men. In group one, lobar distribution and lung involvement patterns was presented in Table 1. Lung involvement was detected in the CT of 131 (60.9%) patients; lung involvement was not detected in the CT of 84 (39.1%) patients. This finding was correlated with the results reported in the recent literature. The most prominent lung involvement pattern was ground glass opacity.
- The baseline imaging characteristics of the COVID-19 patients with CT findings (n=131).
The age and gender characteristics of the cases with and without COVID-19 pneumonia are summarized in Table 2. The NLR was 2.22±11.15 and the PLR was 142.77±387.10 in group 1. The NLR was 1.88±7.47 and the PLR was 130.65±203.68 in group 2. The differences in the NLR and the PLR were determined to be statistically significant among the 2 groups (Table 2).
- Comparison of laboratory features of COVID-19 patients with and without CT findings.
The NLR, PLR, and other parameters are shown in Table 3, a positive relation was demonstrated between NLR (r=0.225, p=0.010) and PLR (r=0.244, p=0.005) and TLSS.
- The correlation between CRP, ferritin and the other markers according to TLSS in patients with COVID-19.
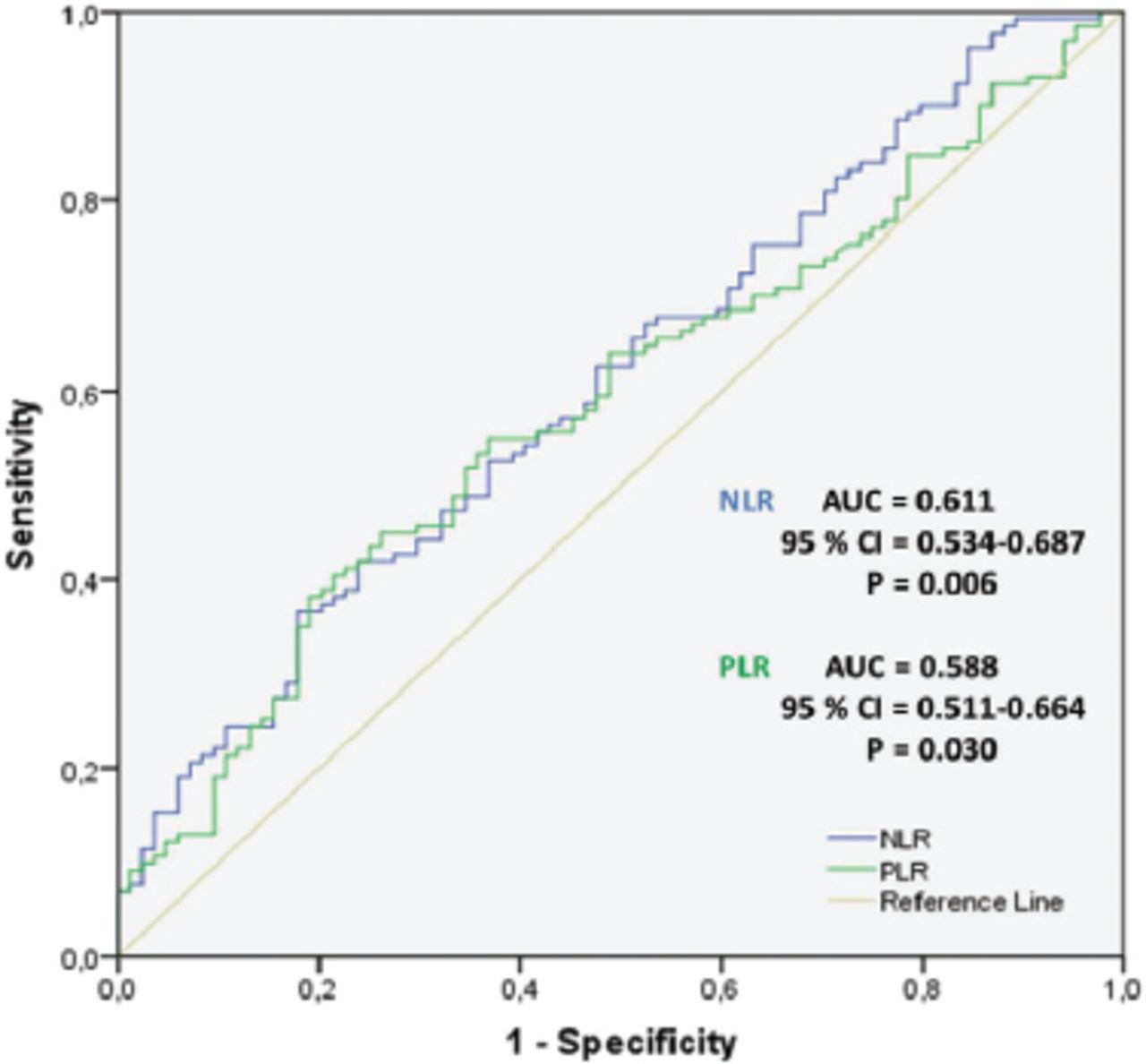
Among the COVID-19 patients, NLR showed lung involvement by ROC curve analysis, with a cut-off value of 1.87, a sensitivity of 62%, a specificity of 52%, and p=0.006 (area under the curve [AUC]: 0.611, 95% confidence interval [CI]: [0.534-0.687]). Platelet to lymphocyte ratio had a cut-off value of 125.47 with a sensitivity of 64%, a specificity of 52%, and p=0.030 (AUC: 0.588, 95% CI: [0.511-0.664]) (Figure 1).

- Receiver-operating characteristic curve of neutrophil lymphocyte ratio (NLR) and platelet lymphocyte ratio (PLR) for predicting patients with lung involvement of coronavirus disease -19 (COVID-19) in in the study population. AUC: area under the curve, CI: confidence interval
Stepwise regression analyses showed that there was an independent relationship between NLR (β=4.370, p=0.036), PLR (β= -4.161, p=0.024), and TLSS. When the relationship of NLR and PLR to TLSS was evaluated using linear regression analysis, it was seen that NLR (β=4.370, p=0.036) and PLR (β= -4.161, p=0.024) predicted TLSS independently of various variables (Table 4).
- Linear regression analysis for TLSS in patients with coronavirus disease -19 (COVID-19).
Discussion
In this study, we evaluated the relationship between NLR and PLR in COVID-19 patients and lung involvement and disease severity using CT scans. Our findings showed that both NLR and PLR were higher in COVID-19 patients with lung involvement in comparison to those without lung involvement. Moreover, we found a relationship between NLR and PLR and TLSS in patients with lung involvement on CT.
Although the RT-PCR test is the gold standard for the diagnosis of COVID-19 patients, lung CT can be used to support the diagnosis and treatment follow-up in these patients. Furthermore, it is known that the evaluation of the lung in CT may show abnormalities before the RT-PCR test.23 Xiang et al,24 reported that the CT scans in COVID-19 patients could enable the monitoring of dynamic changes in lung involvement to evaluate the density, stage, and severity of pulmonary lesions. Furthermore, it was determined that idea scoring system could be used to assess the clinical course and severity of the disease by considering the lobe and segment involvement in the lung using CT. Li et al,25 evaluated the relationship between the severity of the disease and the TSS performed by evaluating the lung involvement of over 5 lobes on CT. They found that the TSS was high in severe and critical cases. Zhang et al,26 scored lungs topographically by evaluating the lung at 5 levels. They showed that thorax CT scoring can predict systemic involvement and prognosis. Yang R et al,27 reported that, in COVID-19 patients, the severity of pulmonary involvement can be evaluated quickly and objectively using the CT severity score. Zhang et al,28 showed that the severity of lung infiltrations detected in lung CT scans might be related to laboratory parameters in the early and later stages of the disease. In the same study, they evaluated COVID-19 patients radiologically in 4 stages (the early, progressive, peak, and absorption stages). They found that there were statistically significant differences in lymphocyte values in the neutrophils and thrombocytes at these stages; they also reported that there is a correlation between neutrophil counts and TLSS in the early and advanced stages of COVID-19.
More than 50% of the bone marrow is responsible for the production of neutrophils. These cells are the first line of defense in the immune system. Neutrophils play an active role in the production of many lyticenzymes, free oxygen radicals, and cytokines. The role of cytokines is very important in the pathogenesis of many infectious diseases, especially COVID-19.15-17 Neutrophils and platelets are involved in the production of cytokines, and cytokines also contribute to the activation of neutrophils and platelets. Studies have shown that platelets play an active role in inflammation and they have regulatory properties on the immune system.29 After this complex process occurs, changes in lymphocyte levels can be observed. In COVID-19 patients, it is thought that lymphopenia may develop due to the attack of lymphocytes expressing the angiotensin-converting enzyme receptor by SARS-CoV-2, with the apoptosis of lymphocytes that increase secondary to the inflammatory process and the released cytokines. Moreover, lymphocyte proliferation defects can be observed as a result of metabolic disorders, such as the reticulo endothelial system (such as the spleen and thymus) and possible hyperlactic acidemia.18-20 When neutrophils, platelets, and lymphocytes are evaluated in COVID-19 patients, it is predicted that inflammatory markers, such as NLR and PLR, which are composed of these components, may cause some changes in this disease.
Qu et al,21 found that the increased PLR values in COVID-19 patients were associated with the clinical course of the disease and the length of hospital stay. In the same study, they reported that the cytokine storm, which is among the most important complications of COVID-19, affected the platelet and PLR levels. Yang et al,22 found that NLR may be related to the severity of the infection and that a high NLR is an independent prognostic biomarker for COVID-19 patients. In their semi-quantitative segmental CT scoring study, Yang et al,22 compared the initial thoracic tomography of the patients. They confirmed that the thorax CT score was higher in COVID-19 patients than non-severe patients and that the first CT scan could be used in the triaj of the patients.27 Chan et al,29 evaluated a total of 20 studies in their meta-analysis and reported that NLR and PLR can be used as independent prognostic markers of disease severity in COVID-19.
When neutrophils, thrombocytes, and lymphocytes are evaluated in COVID-19 patients, it is predicted that inflammatory markers, such as NLR and PLR, which consist of these components, may result in some changes in this disease.
In our study, NLR and PLR results were higher in patients with lung involvement in comparison to those without lung involvement. This was correlated with the TLSS, the evaluation of lung findings in CT with ROC analysis, and linear regression analysis, suggesting that NLR and PLR may be markers that can be used in the follow-up of disease severity in COVID-19 patients.
Study limitations
This is a retrospective study and the data is based on the CT findings and laboratory values of the patients at the time of initial diagnosis. Moreover, the effects of the control CT findings and the treatments applied on the bone marrow were not evaluated.
In conclusion, there are many studies related to lung involvement and severity of COVID-19; some of them claimed that thoracic CT showed lung involvement and severity of COVID-19, others claimed that PLR and NLR showed lung involvement and severity of COVID-19. This study verified that NLR and PLR values can be 2 inflammatory indicators that can be used to demonstrate lung involvement and disease severity in COVID-19 patients. With these results, NLR and PLR can be among the indicators that can be used to figure out disease severity in COVID-19 patients when supported by different prospective studies.
Acknowledgment
The authors gratefully acknowledge Scribendi (www.scribendi.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 16, 2021.
- Accepted September 30, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.