


Abstract
Objectives: To identify the sociodemographic and clinical predictors of uncontrolled diabetic patients, to identify high-risk and people with impaired glycemic control, to establish more effective strategies for reducing morbidity and mortality.
Methods: This case-control study of 8209 enrolled patients were included from the diabetes registry by Chronic Illness Center (CIC), Family and Community Medicin, Prince Sultan Military Medical City, Riyadh Saudi Arabia between February 2019 and February 2020. Cases are defined as patients with type II refractory diabetes having persistent HbA1c >9, not reach adequate glycemic control despite intensified therapy under specialist care (CIC) for at least 6 months. Controls were defined as patients with Hba1c ≤9. Multivariable regression analysis was used to identify predictors for patients with the persistent outcome of HbA1c >9%.
Results: Overall, a total of 1152 cases and 4555 controls were included. Patients with refractory diabetes were younger (mean: 58.5, standard deviation [SD]: 11.7) and females (63.4%). Duration of diabetes (13.3, SD: 7.4, p<0.001) and the mean value of low-density lipoprotein (LDL) (2.7, SD: 0.91, p<0.001) were significantly higher in the refractory group. The findings from the final model revealed that with every unit increase in age (odds ratio [OR]: 0.97, [95% confidence interval [CI]: 0.96-0.98]) and body mass index the odds of having refractory diabetes significantly reduced by 0.97 times (OR: 0.97, [95% CI: 0.95-0.99]). While with every unit increase in the duration of diabetes (OR: 1.03, [95% CI: 1.01-1.05]), systolic blood pressure (OR: 1.01, [95% CI: 1.00-1.02]) and LDL (OR: 1.42, [95% CI: 1.23-.62]) the odds of having refractory diabetes significantly increased by 1.03 and 1.42 times respectively compared to controls when adjusted for gender, albumin creatinine, diastolic blood pressure.
Conclusion: The findings from this study helped classify the predictors of refractory patients with diabetes. Understanding refractory patients’ predictors may help to develop new therapeutic strategies to boost their glycemic status safely.
Registries may help in developing more effective strategies to manage patients who fail to achieve optimal glycemic control despite adequately prescribed interventions, even being treated under a specialist care setting.1 Such types of resistant patients are termed as functional refractory patients and need strong monitoring to prevent them from developing long term complications of type II diabetes mellitus (T2DM).2 Such refractory patients reflect that, despite the oral and injectable treatments to control higher levels of blood glucose, such patients do not achieve glycemic control despite continuing, inclusive, evidence‐based treatment.3-5 Moreover, such refractory patients are at higher risk of diabetes-related complications such as microvascular disease and cardiovascular mortality, which may ironically deteriorate with more rigorous therapeutic measures.6
Such refractory patients may be found with disproportionate distribution in specialist care clinics and may demonstrate features that may help in foreseeing their outcome and may exemplify a group of individuals with certain barriers to care and specialized clinical and sociodemographic characteristics.6 Such patients might respond to aggressive glycemic control measures with higher mortality when compared to other patients with T2DM. Patients who do not achieve sufficient glycemic control notwithstanding strengthened therapy under specialist care represent an essential, but inadequately studied group that has newly been shown to carry a greater mortality risk than diabetic patients.6 Further, the natural history of diabetes and the features of these functionally refractory patients have not been well-characterized. Therefore, such types of patients need to be vigilantly monitored by establishing a surveillance system in the form of registries. Different studies in the literature have investigated the characteristics of such refractory patients and researchers both in developed and developing countries have explored the determinants of refractory patients in their respective settings and populations by establishing registries.3-5
The results of a systematic literature survey were recently published by an author in which investigators checked all published diabetes population registries to analyze the published registries for patient characteristics and their outcomes.2 The literature search identified 13 diabetes registries whose databases recorded outcomes of specialist care.2 The analysis of the published registries provides insights into the predictors of refractory patients and challenges faced by them.2 Although, one of the main strengths of this survey was the inclusion of the large LMC Diabetes & Endocrinology Registry and its representation of patients from multiple regions in North America, the findings of the registry might not be generalizable to the population in middle east countries such as Saudi Arabia. Therefore, it is important to explore and investigate the predictors of refractory diabetic patients using the hospital or population-based diabetes registry (DR) data of Saudi Arabia, where one third (32.1%) of the people are affected by T2DM.7
A large hospital-based Saudi National Diabetes Registry, which is electronically built for diabetic patients, sponsored by King Abdulaziz City for Science and Technology, Riyadh, Saudi Arabia retrieves data from medical files.8 Besides, Chronic Illness Center (CIC), Family and Community Medicine, Prince Sultan Military Medical City (PSMMC), Riyadh, Saudi Arabia initiated the first DR among all military hospitals with support of the Quality Department in Medical Services Directorate (MSD), Ministry of Defense as a part of the Diabetes Improvement Project Task Force. One of the main objectives of this hospital-based DR is to strengthen diabetes surveillance, to manage the individuals diagnosed with diabetes promptly, and to provide a support system to clinicians for making an evidence-based decision.8
In addition to evaluating patterns in demographic and clinical features and outcomes of diabetic patients, registry data may be useful in calculating the proportion of refractory diabetic patients who, while being actively treated, have impaired glycemic control. In addition, the data can also be useful in exploring and interpreting Saudi Arabia’s characteristics and predictors of refractory T2DM patients. We used the data from the current registry data to explore the sociodemographic and clinical predictors of refractory patients using a case-control approach.
The main objective of this study was to identify the sociodemographic and clinical predictors of uncontrolled diabetic patients (refractory) registered with the CIC, PSMMC. This research would enable Saudi Arabia’s health care providers to identify high-risk and disadvantaged people with impaired glycemic control and to establish more effective strategies for reducing their morbidity and mortality and enhancing their quality of life.
Methods
This case-control study cases were included from the data registry formulated by CIC in PSMMC between February 2019 and February 2020. The total number of patients enrolled in the DR was 8209. Cases were defined as individuals with refractory diabetes that is having persistent glycated hemoglobin (HbA1c) >9 for at least 6 months, which defined as patients who do not reach adequate glycemic control despite intensified therapy under specialist care (CIC) for at least 6 months and despite ongoing, comprehensive, evidence-based care from update guideline of American Diabetes Association while controls were taken from the same registry having T2DM with Hba1c ≤9 for more than one year. We included all patients who were diagnosed with T2DM regardless of age or gender. Further, these were only those patients who were followed at the CIC, PSMMC. In contrast, patients with type 1 DM and pregnant women were excluded from the study.
The diabetic registry was the main source of the data for the cases and controls that aimed to collect data on patients with T2DM. The registry started in 2019 and the data were available until February 2020. The DR began in February 2019 with data collected manually until February 2020 and data was migrated to a web-based data (Oracle). Throughout the regular patient visits/year the status of registered patients is regularly updated with updates of any new complication(s) such as diabetic nephropathy and status of renal function.
During their daily visits, the clinic staff and nurse specialists began tracking their patients. Registration was initially carried out on paper forms and submitted electronically to CIC-DR staff to input into a database set. The DR portion included demographic data of the patient clinical data of the patient, anthropometry, laboratory investigation, usage of facilities, and risk factors. Since this was a case-control study so there was a potential for recall bias and we overcame this bias by recording data from the registry on all sociodemographic and clinical characteristics instead of asking for data from patients retrospectively. Moreover, to overcome the interviewer bias, we kept the staff blind to the status of cases and controls to collect data without introducing information bias.
All categorical variables are presented as frequency and percentages while continuous variables as mean and standard deviation (SD). Chi-square and independent t-test has been used to see the differences among cases and controls. Logistic regression was used to estimate the predictors of refractory diabetes. Variables with p-value of 0.25 and less at univariable were included in multivariable models.
Statistical analysis
We developed 2 models to assess the predictors of refractory DM. Both models were grounded and developed based on the p-value of univariable analysis, which was set to ≤0.25. For both models, we used logistic regression to understand the relationship between important proposed predictors and refractory DM. In the first model, we assessed the relationship between refractory DM and predictors such as age, duration of DM, body mass index (BMI), and low-density lipoprotein (LDL) adjusting for gender and albumin/creatinine ratio. Since we hypothesized to adjust the aforementioned variables for one demographic (gender) and one clinical variable (albumin/creatinine ratio), we did not report the adjusted OR for gender and albumin/creatinine ratio. Similarly, we took additional step and assessed the relationship between refractory DM and predictors such as age, duration of DM, BMI, and LDL adjusting for gender, albumin/creatinine ratio, and systolic BP. Therefore, adjusted results are only shown for the proposed variables (age, duration of DM, BMI, and LDL) in the both models rather than for those variables that were either insignificant in the univariable analysis or were used as variables to be conditioned on (gender, albumin/creatinine ratio, and systolic BP). Results are presented as odds ratio (OR), adjusted odds ratio (AOR) along with 95% confidence intervals (95%CI).
Results
A total of 1152 cases with refractory diabetes and 4555 patients with HbA1c level <9 as controls were included in the final analysis. Patients with refractory diabetes were significantly young (mean: 58.5, SD: 11.7) were females (63.4%). No difference was found for mean BMI (p=0.139), blood pressure, and albumin creatinine ratio (p=0.06). Duration of diabetes was significantly more in the refractory group (13.3, SD: 7.4, p<0.001). Likewise, the mean value of LDL was significantly high among the refractory group (2.7, SD: 0.91, p<0.001) (Table 1).
- Baseline characteristics of patients with refractory diabetes (n=5708).
Looking at the trend of HbA1c level at each visit we found that at each visit there was an increase in the mean HbA1c values among the refractory group (1st visit: 9.7, 4th visit: 10.1) (Figure 1), at each visit (visit 1-4) refractory patients had a significant increase in mean HbA1c values compared to controls (Table 2).
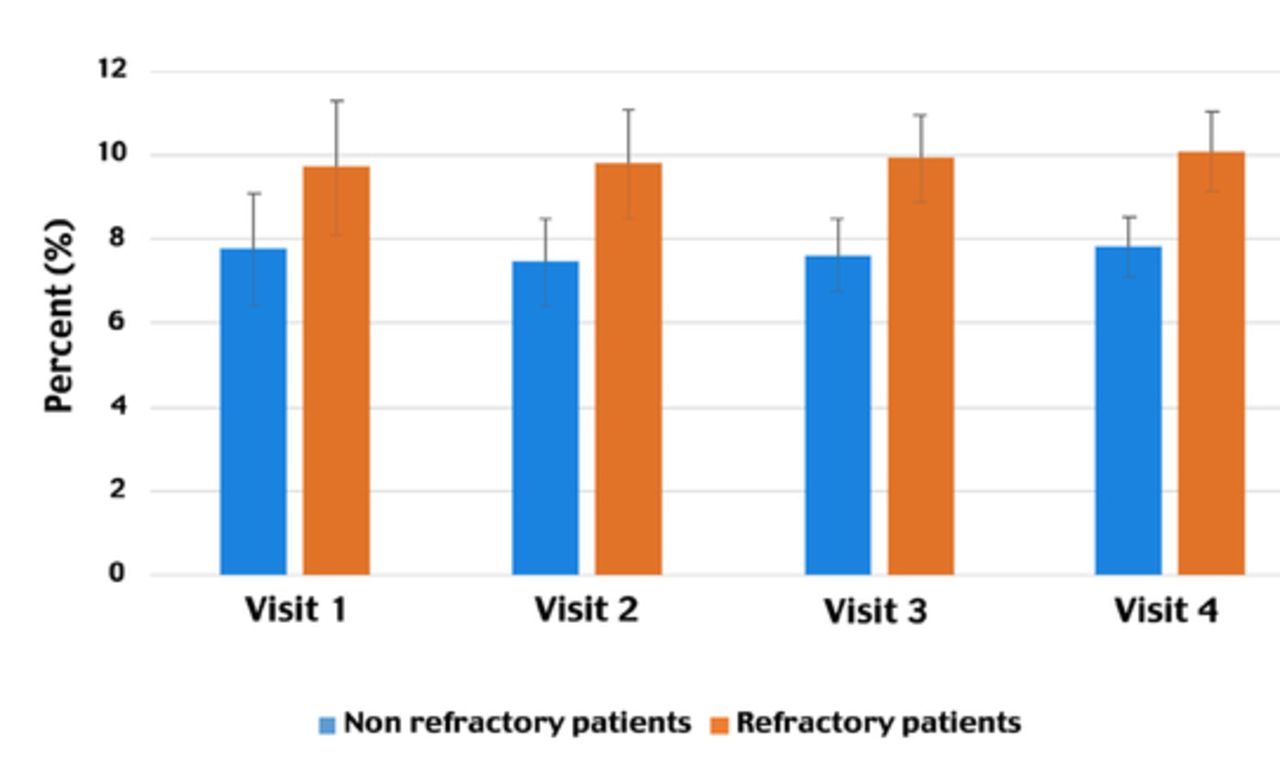
- Change in HbA1c levels among refractory patients (n=1153). Trend of glycated hemoglobin levels for patients by visit.
- Change in mean HbA1c among patients with refractory and non-refractory diabetes (n=5708)
With every unit increase in age and BMI, the odds of having refractory diabetes significantly reduced by 0.98 and 0.99 times respectively. The female gender had 33% more odds of having refractory compared to males. With every unit increase in the duration of diabetes, LDL, and albumin creatinine the odds of having refractory diabetes significantly increased by 1.01, 1.30, and 1.00 times respectively compared to the controls. Two adjusted models were run, model one included all the variables with a p<0.25 at univariates and we found that after adjusted for gender and albumin creatinine ratio, with every unit increase in age and BMI the odds of having refractory diabetes significantly reduced by 0.97 times. While with every unit increase in the duration of diabetes and LDL, the odds of having refractory diabetes significantly increased by 1.03 and 1.42 times compared to controls. When the model was adjusted with all the variables included in model one along with systolic and diastolic blood pressure, we found that increasing age and BMI had protective adds of having refractory diabetes and duration of diabetes, systolic BP and LDL were significant predictors of refractory diabetes (Table 3).
- Predictors of refractory diabetes (n=1153).
Discussion
We used the data from a large hospital-based registry for T2DM in Saudi Arabia to understand the predictors of refractory patients, who are at a high risk of developing diabetes complications. Early detection and screening of such patients are crucial steps to identify barriers to glycemic control and deliver more focused and patient-centered care effectively to reduce diabetes morbidity and mortality. The findings from the final model, adjusted for gender, albumin creatinine, and diastolic blood pressure, illustrated that as the age and BMI of the patients’ increases, the tendency of a patient to become refractory reduces, meaning that younger patients with lower BMI were found to be refractory with poor glycemic control. Additionally, patients with longer duration of diabetes, higher levels of LDL, and high systolic blood pressure were more likely to be refractory patients when compared to their counterparts.
The study findings regarding the duration of DM and age are consistent with findings from the Canadian registry, which reported that younger diagnostic age and longer diabetes duration were associated with refractory status later in their lives.2 Another study from Ontario Canada demonstrated consistent findings regarding age and duration of diabetes.9 The Third National Health and Nutrition Review Survey (NHANES III: 1988-1994) indicated that younger patients were more likely to have an elevated HbA1c level, although there was no substantial correlation between age and HbA1c levels in the predominantly white population.10 The Canadian registry also found a negative correlation between BMI and refractory status.2 Our study findings regarding patient’s age and elevated LDL levels are consistent with the Singaporean diabetes database.11 However, our findings regarding BMI contradict the findings from the Singaporean diabetes database, where authors found higher BMI to be correlated with the refractory status of the patients, defined in that study as HbA1c >8.0%.11 Since higher BMI indicates obesity, which is more likely to be associated with poor glycemic control, protective findings related to BMI should be interpreted with caution. Authors in few other studies also found that patients’ age was inversely associated with glycemic control, whereas the duration of diabetes was positively associated with glycemic control.12,13
It is unclear why younger patients are refractory than older patients because in Saudi Arabia, everyone regardless of age, has equal access to medical care provided by the public sector. However, older patients may be more motivated to take care of their diabetes, more compliant with medications, and eat a healthy low-fat diet.14 Conversely, younger patients may not consider DM important and be less adherent to medication, lifestyle, and diet restrictions. The persistence of HbA1c elevation in younger individuals could be due to inadequately low doses of medication or uncommon use of mixed drug regimens.15 Such behaviors might result in poor glycemic control thus forcing these patients to become refractory. For example, a study conducted by Song et al16 in 2009, reported that the management of diabetes was inadequate among the early-onset T2DM cohort and these young patients were at higher risk of poor glycemic control at an earlier stage. Lastly, younger patients are more obese than older patients with resultant higher insulin resistance, therefore, may need more aggressive therapy to achieve glycemic control.11 Descriptive findings from our DR demonstrated that females are more obese than males. Although the premise regarding women and younger patients being more obese than men and older patients respectively seems to contradict with our study findings on BMI being more protective, it is likely that protective study findings for BMI could be due to chance and need to be explored further in the studies. Therefore, we recommend that our findings, regarding BMI, need to be interpreted cautiously.
Likewise as expected, longer duration of diabetes might make one’s physiological system less responsive to medications thus resulting in poor glycemic control, which is consistent with other studies including the Canadian registry.17-19 A study conducted by Juarez et al,20 reported that patients who were diabetic for more than 10 years were more than 9 times likely to have poor glycemic control than those who were diabetic for 3 years.20 Longer duration of diabetes is associated with being a refractory patient because of progressive impairment of insulin secretion due to β-cells failure and eventually decrease in insulin secretion, which becomes less responsive to diet or and oral agents.21 Lastly, our findings regarding the association between raised LDL levels and high systolic blood pressure with refractory status are consistent with other studies.24,25 The mechanism of dyslipidemia in T2DM has been explained based on insulin resistance that distorts the lipoprotein lipase to hepatic lipase ratio resulting in increased LDL-cholesterol levels.22 One of the studies of 2,200 T2DM patients showed that HbA1c had a direct and significant correlation with cholesterol, triglycerides, and LDL and an inverse correlation with HDL.24
Study limitations
The DR database is one of the largest of any special care as chronic illness center DR among family medicine center in Saudi Arabia that caters to diabetic patients from across Saudi Arabia, with diverse age groups, and socioeconomic status. Besides, uniform data collection procedures in hospitals contributed to data consistency. Although due to the nature of the registry database, a causal relationship between the independent and dependent variables could not be established, the information from the registry can be helpful to generate hypotheses that can be tested in further studies. Because the registry included both new cases and cases coming for follow-up, therefore, we collected information on both independent and outcome variables simultaneously. Thus, based on the available information, we cannot establish temporality; however, we recommend investigating the temporal relationship between independent variables and refractory DM using the data from this registry or by conducting separate longitudinal studies. Lastly, the findings of this registry can be generalized to other regions of Saudi Arabia. Our research, however, has some limitations. We did not study important variables, such as the history of patients with hypoglycemia, method of treatment (oral vs. insulin), non-adherence to treatment, physical activity, and dietary intake. Our analysis was adjusted for the covariates that differed between the groups, but there may have been other unmeasured or unknown differences between the groups for which we could not adequately adjust. There were missing data of BMI and albumin/creatinine ratio because the data for these variables were collected after the registry commenced rather than at the conception of the registry. Also, the DR is considered as guidance to identify gaps that could occur in terms of collecting data during the process and rectify the same gaps accordingly.
In conclusion, the findings from this registry data have helped to classify the predictors of diabetic refractory patients in Saudi Arabia with impaired glycemic control. This, in turn, will provide clinicians with an organized framework to establish cost-effective and creative strategies for these patients that do not need specialists on their own. In addition, recognizing the predictors of functionally refractory patients could help to establish new treatment modalities and services such as comprehensive care for uncontrolled diabetic patients to safely improve their glycemic status through a multidisciplinary team approach. In exchange, this would prevent complications such as cardiovascular death, stroke, and microvascular disorders like retinopathy, neuropathy, and nephropathy from occurring in patients. Disease management services could play a role in increasing the feedback of diabetes counselors or computerized monitoring systems. Diabetes management and glycemic regulation for the population can be enhanced in Saudi Arabia by applying these techniques to both specialist and primary care levels. Provided the current obstacles in achieving glycemic targets for diabetic patients in Saudi Arabia, these findings on refractory patients should be helpful to plan for specialist care in the primary care setting. Moreover, continuous endeavors should be made to establishing and strengthening such registries, with the principal goal of providing ongoing feedback to clinicians and caregivers.
Withdrawal policy
By submission, the author grants the journal right of first publication. Therefore, the journal discourages unethical withdrawal of manuscript from the publication process after peer review. The corresponding author should send a formal request signed by all co-authors stating the reason for withdrawing the manuscript. Withdrawal of manuscript is only considered valid when the editor accepts, or approves the reason to withdraw the manuscript from publication. Subsequently, the author must receive a confirmation from the editorial office. Only at that stage, authors are free to submit the manuscript elsewhere.
No response from the authors to all journal communication after review and acceptance is also considered unethical withdrawal. Withdrawn manuscripts noted to have already been submitted or published in another journal will be subjected to sanctions in accordance with the journal policy. The journal will take disciplinary measures for unacceptable withdrawal of manuscripts. An embargo of 5 years will be enforced for the author and their co-authors, and their institute will be notified of this action.
Acknowledgment
The authors would like to thank the Medical Services Directorate Quality Department for their vision, guidance and support towards the development of the first Diabetes registry in Military Hospital among Primary Care Centers. We are indebted to the General Executive Director of Prince Sultan Military Medical City, Riyadh, Kingdom of Saudi Arabia, Major General Dr. Saud Al Shlash; to all the clinicians including physicians, clinical pharmacists, nurses, diabetic educators, dietitians, social workers, Diabetes Registry coordinators (Anwar Al Ataibi and Amal Al Otaibi); to Ms. Reuof Bushnag from the Wazrat Health Care Centers; to the in-charge of Wazrat Health Care Center, Dr Azzam Al Otaibi, and to Dr. Mohammed AbdulMogith; to the deputy-in-charge of Wazrat Health Care: Dr. Nawaf Al Okail, for their support to establishing this program and to their team of colleagues from the Prince Sultan Military Medical City, Information Technology, Riyadh, Kingdom of Saudi Arabia, Mrs. Wafa Al Bahlal, Salman Al Otaibi, Peer Shareef, Murad Saeed, and Mr. Fedda Hussein for their dedication to establishing new electronic Diabetes Registry Program. The authors acknowledge Researchofy (www.researchofy.com/) for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 6, 2020.
- Accepted December 30, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.