


Abstract
Objectives: To compare risk factors and clinical outcomes among COVID-19 patients with or without diabetes in the United Arab Emirates (UAE).
Methods: Data of 350 COVID-19 positive patients, admitted to Al Kuwait Hospital in Dubai, UAE, from February to May 2020 was collected retrospectively, including demographic data, clinical symptoms, blood tests, as well as radiographical assessments, and clinical outcomes of COVID-19. The design of the study is a retrospective cohort study.
Results: COVID-19 patients with diabetes belong to an older age group, had a higher percentage of male patients, exhibited more lymphopenia and neutrophilia, and higher ferritin levels. Additionally, patients with diabetes presented fever and shortness of breath (SOB), displayed more bilateral airspace consolidation and opacities in their chest x-ray and CT scans, compared to non-diabetics. A higher percentage of critical, ICU-admitted, and death of COVID-19 cases in the diabetic group was also reported. This was along with a concomitant increase in C-reactive protein, procalcitonin, and lactate dehydrogenase levels.
Conclusions: Diabetes is considered a comorbidity as diabetic patients showed more severe COVID-19 symptoms that led to critical clinical outcomes such as ICU admission and death.
Severe acute respiratory distress syndrome virus (SARS-CoV-2) another member of beta-coronaviruses, is very closely related to the SARS-CoV, that was reported in 2002.1 Coronavirus-19 (COVID-19) infection caused by SARS-CoV-2 virus was first reported last December in Wuhan, China.2 Subsequently, it was declared a global pandemic by the World Health Organization (WHO). SARS-CoV-2 utilizes several host receptors for cell entry in the lungs such as angiotensin-converting enzyme 2 (ACE2) and the cellular serine protease TMPRSS2.3-6 Angiotensin-converting enzyme 2 is expressed in various organs including lung and alveolar epithelial cells, which makes them more susceptible to COVID-19 viral infection.7
Clinical symptoms of COVID-19 could vary from fatigue, fever, cough, headache, nasal congestion, dyspnea, nausea, and diarrhea.1 These symptoms could progress into pneumonia and acute respiratory distress syndrome (ARDS) that is accompanied by neutrophilia, lymphopenia, and thrombocytopenia.8-11 Since COVID-19 was associated with inflammation, there was an elevation in some markers such as C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and proinflammatory cytokines.8,12
Diabetes mellitus (DM) has been reported as one of the comorbidities for disease progression and mortality of COVID-19.13 This has been reported by studies on COVID-19 patients in China, where 19% had diabetes and 42% of the deaths due to SARS-CoV-2 were in patients with diabetes.14,15 This is similar to SARS infection, where hyperglycemia and diabetes were among the many risk factors associated with the severity and death related factors.16,17 Also, the COVID-19 patients who developed ARDS had more comorbidities than those who did not develop ARDS, where diabetes was the second most frequent comorbidity.18 Several factors could be contributing to this high risk observed in diabetes.First, the hyperglycemic environment in diabetes increases the susceptibility to infections.19,20 In addition, the impairment of the immune system in diabetes could be a contributing factor in their vulnerability to COVID-19 infection. Furthermore, patients with DM have reduced pulmonary capacity, especially in poor control status of the disease and hence, would increase their vulnerability to respiratory infections, such as in the case of COVID-19.21
In the United Arab Emirates (UAE), the International Diabetes Federation (IDF) has reported that the prevalence of diabetes reached almost 15%, which continues to rise at a faster rate than the MENA region.22,23 Hence, the aim of this study was to identify the differences in the demographic factors, biochemical characteristics, risk factors, and clinical outcomes among diabetic and non-diabetic COVID-19 patients in the UAE.
Methods
Data of a total of 350 COVID-19 positive patients (diabetics n=111, non-diabetic=239) was collected retrospectively, who were admitted to Al Kuwait Hospital, Dubai, UAE from February - May 2020. Ethical approval for this study was obtained from the Ministry of Health and Prevention Research Ethics Committee (MOHAP/DXB-REC/MMM/NO.44/2020), and the study was performed according to the principles of Helsinki Declaration. The design of the study is a retrospective cohort study.
The clinical data included age, gender, medical history of diabetic status and illness severity, as well as the recent history of travel or contact with COVID-19 case. Also, the presence or absence of symptoms was documented including fever, myalgias, fatigue, anorexia, headache, confusion, rhinorrhea, sore throat, cough, sputum production, hemoptysis, shortness of breath, nausea, vomiting, diarrhea, anosmia, and ageusia. Blood tests including neutrophil count, lymphocyte count, white cell count (WCC), ferritin, hemoglobin (Hb), lactate dehydrogenase (LDH), CRP, procalcitonin and coagulation tests (D-dimer and the international normalized ratio [INR]). Also, liver and kidney function tests were collected. Liver function tests included albumin level, alanine aminotransferase (ALT), aspartate aminotransaminase (AST), serum bilirubin, and alkaline phosphatase level (ALP). The renal function tests included urea and creatinine levels as well as the estimated glomerular filtration rate (eGFR) that was calculated for all the patients using the modification of diet in renal disease (MDRD) equation. Radiographical assessment using chest x-ray and computed tomography (CT) tests were performed for most of the subjects.Additionally, data regarding the factors for severe illness and the previous history of cardiovascular disease (CVD), hypertension, stroke, cancer, chronic kidney disease, and chronic lung diseases, was retrieved. Also, deterioration of clinical status was reported including intensive care unit (ICU) admission, need for mechanical ventilation, and death.
Severity of COVID-19 infection was classified based on the following criteria, as previously described.24 The patient is placed in the mild to moderate group if there was no pneumonia or mild pneumonia, while the severe patients were those that had dyspnea, respiratory rate ≥30/min, blood oxygen saturation ≤93% in resting state, ratio of partial pressure of arterial oxygen (PaO2) to fraction of inspired oxygen (FiO2) ≤300 mm Hg, and lung infiltrates >50% within 24-48 hours. The critical patients were those that had a respiratory failure, septic shock, or multi organ dysfunction/failure.
Statistical analysis
The cohort was divided into diabetic and non-diabetic COVID-19 patients. The values represent mean ± SEM for the continuous variables, or percentage relative to the total number of patients in each group for the categorical variables. Statistical analysis was performed using GraphPad Prism 6 software (GraphPad Software, San Diego, CA, USA). Student’s t-test was used to assess the differences between diabetic and non-diabetic patients for the continuous variables, while the Chi-square test was used for the categorical variables. P-value <0.05 was considered statistically significant.
Results
Gender, age, and risk factors associated with COVID-19
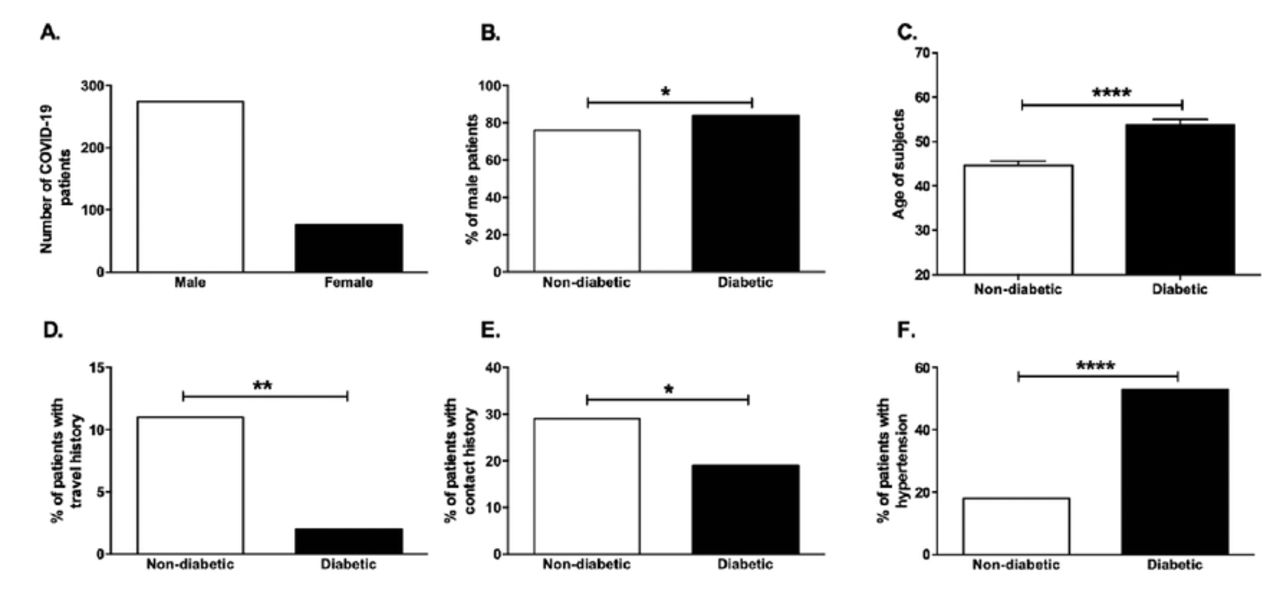
As shown in Figure 1A, the number of male subjects that were positive for COVID-19, was twice as many as the female COVID-19 subjects. Additionally, the percentage of male subjects in the diabetic COVID-19 group was higher than that in the non-diabetic COVID-19 group (Figure 1B, p<0.05). When comparing the age of COVID-19 patients, it was found that the age of the individuals in the diabetic group (53.73±12.79) was significantly higher than the non-diabetic (44.64±14.38) COVID-19 patients (Figure 1C, p<0.0001).
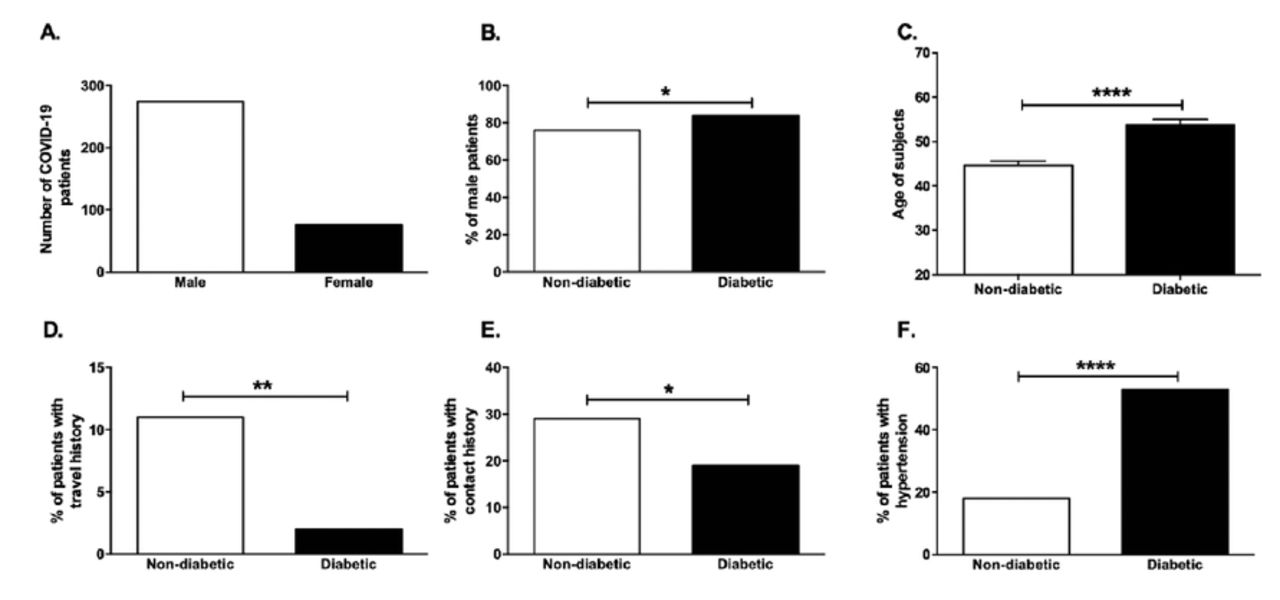
- Gender, age, and risk factors associated with COVID-19 infection. Bar graph showing A) the number of male and female of COVID-19 positive patients, B) the percentage of male subjects in the diabetic and non-diabetic COVID-19 patients. C) Age, D) travel history, E) contact history were compared between diabetic and non-diabetic COVID-19 patients. F) percentage of patients with hypertension. *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001
Out of the factors associated with COVID-19 exposure, travel history or contact with COVID-19 patient could be a great source of COVID-19 infection. As shown in Figures 1D & 1E, it seems that the percentage of people with a travel history and contact with COVID-19 patients was much lower in the diabetic group (p<0.01 and p<0.05). Several risk factors are associated with COVID-19 including CVD, hypertension, cancer, prior stroke, chronic lung disease, and chronic kidney disease. Among these factors, hypertension was found to be more present in the diabetic group of COVID-19 patients (53% in diabetic versus 18% in non-diabetic), as shown in Figure 1F (p<0.0001). All these characteristics were summarized in Table 1.
- Demographic data and comorbidities of the diabetic and non-diabetic COVID-19 patients included in the study.
Clinical symptoms and blood laboratory tests of COVID-19 subjects
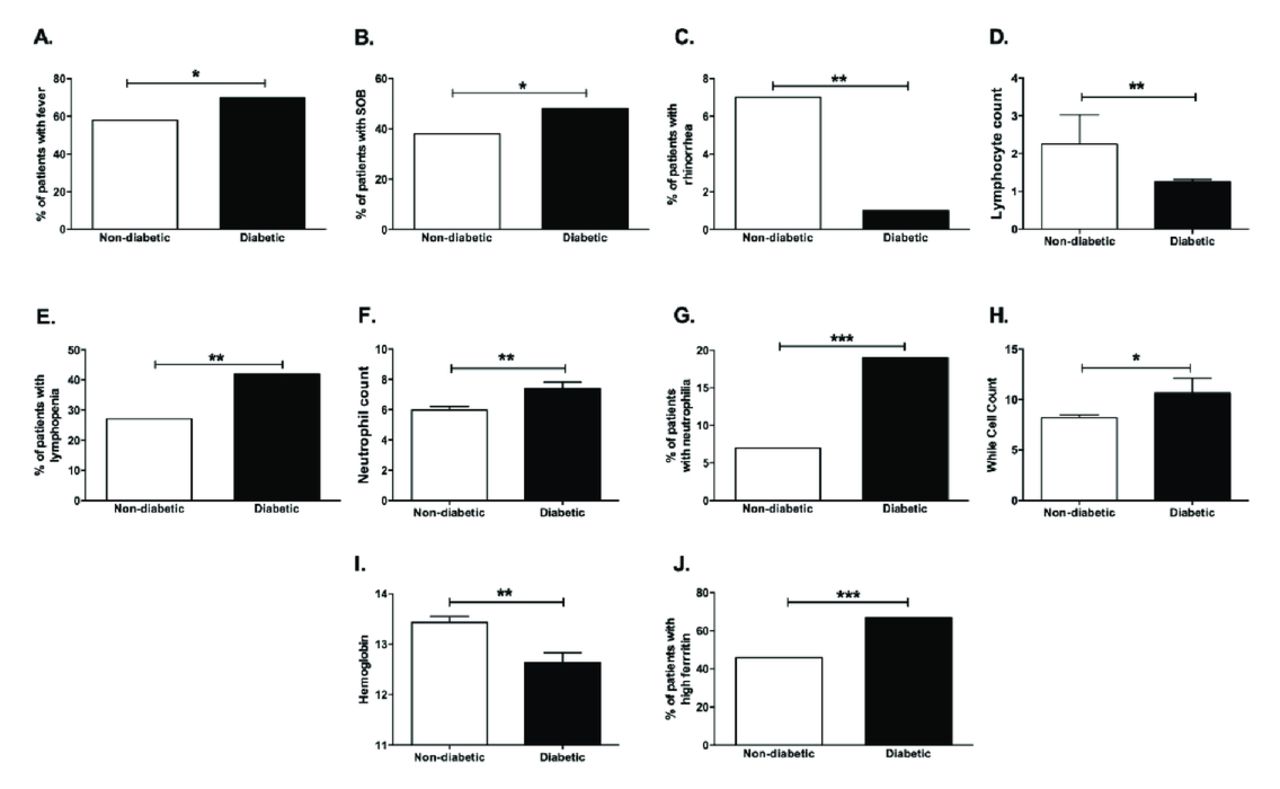
Interestingly, there was a difference in the clinical symptoms associated with COVID-19 between diabetic and non-diabetic patients. For example, fever (70% in diabetic versus 58% in non-diabetic, p<0.05) and shortness of breath (SOB), 48% in diabetic versus 38% in non-diabetic (p<0.05), were found to be more present in diabetic patients compared to non-diabetic COVID-19 patients (Figure 2A & 2B). On the contrary, it seems that the less common feature, rhinorrhea, was reported less in diabetic compared to non-diabetic COVID-19 subjects (p<0.01) (Figure 2C). These findings suggest that diabetic patients tend to have more symptoms of lower respiratory tract infections than upper respiratory tract infection symptoms. However, there was no significant difference between the 2 groups when comparing the following symptoms: cough, sore throat, diarrhea, myalgia, anorexia, nausea, fatigue, and vomiting (data not shown, summarized in Table 2).

- Clinical symptoms and blood laboratory tests of COVID-19 subjects. Percentage of COVID-19 patients with A) fever, B) shortness of breath (SOB), C) rhinorrhea in diabetic and non-diabetic groups. D) Lymphocyte count, E) percent of patients with lymphopenia, F) neutrophil count, G) percent of patients with neutrophilia, H) white cell count (WCC), I) hemoglobin, J) percent of patients with high ferritin were compared between diabetic and non-diabetic COVID-19 patients. *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001
- Clinical symptoms, disease severity markers, and radiographic data of the diabetic and non-diabetic COVID-19 patients included in the study.
Looking at the laboratory blood tests; lymphocyte and neutrophil counts were found to be highly altered in COVID-19 infection. It seems that there was a marked reduction in the lymphocyte count (Figures 2D & 2E, p<0.01), in diabetic (1.256±0.6693) compared to non-diabetic COVID-19 patients (2.255±11.83). On the other hand, as shown in Figures 2F & 2G, there was a significant neutrophilia in diabetic COVID-19 (7.395±4.567) patients compared to non-diabetics (5.971±3.808, p<0.01). However, there was an increase in the total white cell count (WCC) in diabetic COVID-19 patients (10.65±15.36) compared to non-diabetics (8.225±4.064), as shown in Figure 2H (p<0.05). Another blood test would be the assessment of hemoglobin levels (Hb), where it was found to be lower in the blood of diabetic (12.63±2.110) individuals compared to non-diabetics (13.43±1.839, p<0.01), (Figure 2I). Also, as expected, high levels of ferritin were reported in the diabetic group of COVID-19 patients (Figure 2J, p<0.001).
Renal and liver function blood tests in COVID-19 diabetic subjects
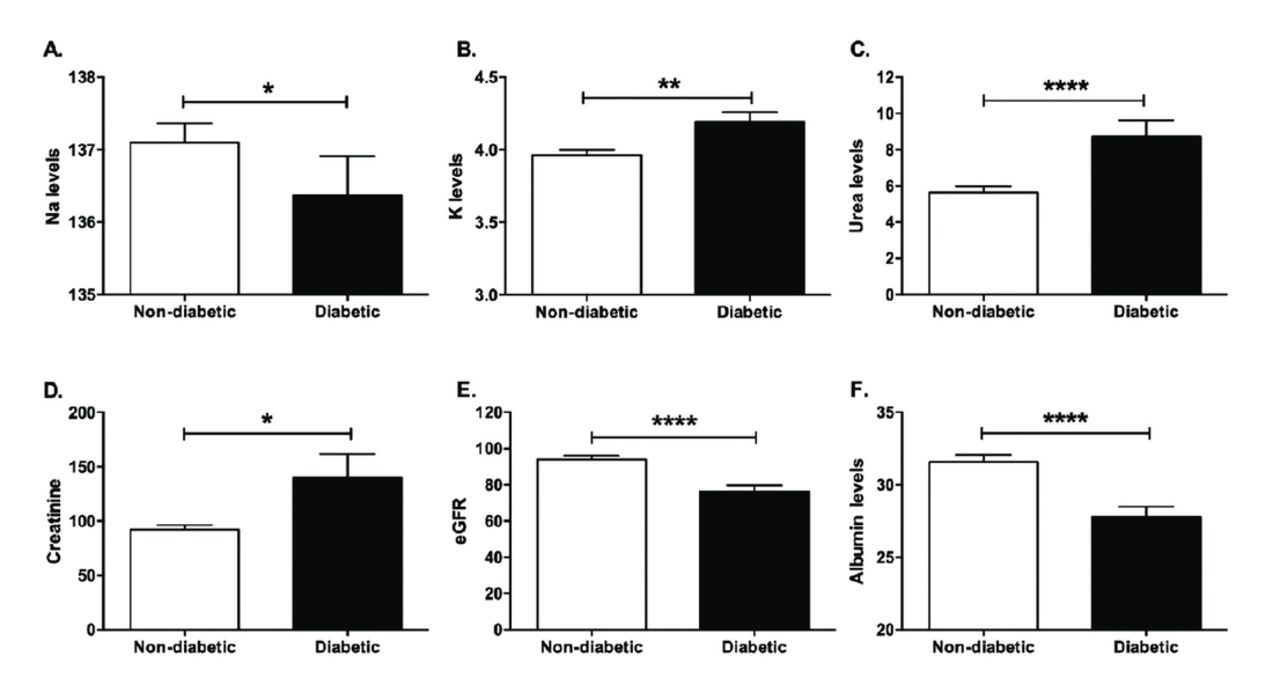
It is worth mentioning that nephropathy is one of the complications of DM. Thus, it is not surprising that the data showed that there was a significant hyponatremia (diabetic: 136.4±5.687, non-diabetic: 137.1±4.122, Figure 3A, p<0.05), hyperkalemia (diabetic: 4.191±0.7182, non-diabetic: 3.963±0.5484,p<0.01, Figure 3B), and increased blood urea (diabetic: 8.722±9.491, non-diabetic: 5.632±5.376, p<0.0001, Figure 3C), in the blood of diabetic COVID-19 patients compared to non-diabetics. This has been further supported by the increased levels of creatinine (diabetic: 139.6±231.7, non-diabetic: 92.12±65.74, p<0.05, Figure 3D), lowered eGFR (diabetic: 76.35±34.28, non-diabetic: 94.10±29.81, p<0.0001, Figure 3E) and hypoalbuminemia (diabetic: 27.79±7.43, non-diabetic: 31.58±7.588,p<0.0001, Figure 3F) in diabetic COVID-19 subjects.
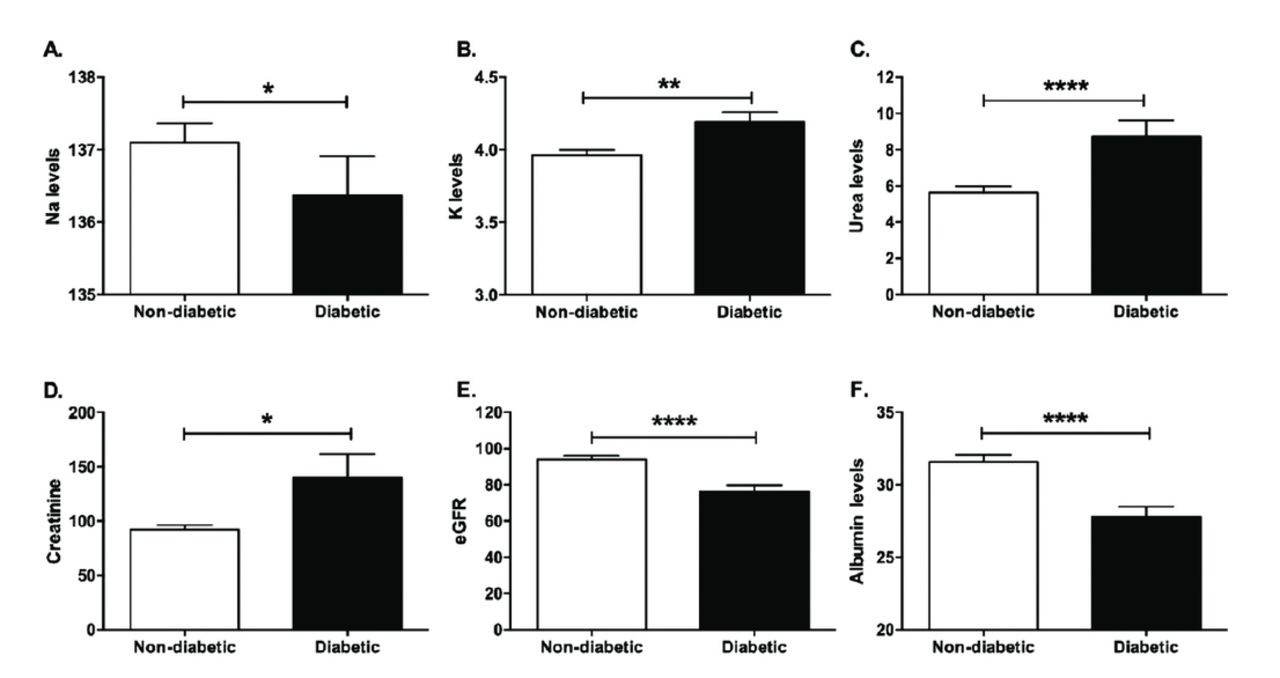
- Renal and liver function blood tests in COVID-19 subjects. A) sodium: Na levels, B) potassium: K levels, C) urea D) creatinine E) eGFR, and F) albumin were compared in the diabetic and non-diabetic groups. * p<0.05, ** p<0.01, *** p<0.001, ****p<0.0001
On the other hand, the liver function blood tests such as ALT, AST, ALP, and bilirubin did not show any difference between the 2 groups, suggesting that there was no change in the status of the liver in diabetic and non-diabetic COVID-19 patients. All these laboratory and blood tests were summarized in Table 3.
- Blood, renal, and liver tests of the diabetic and non-diabetic COVID-19 patients included in the study.
Radiological assessment of diabetic COVID-19 patients
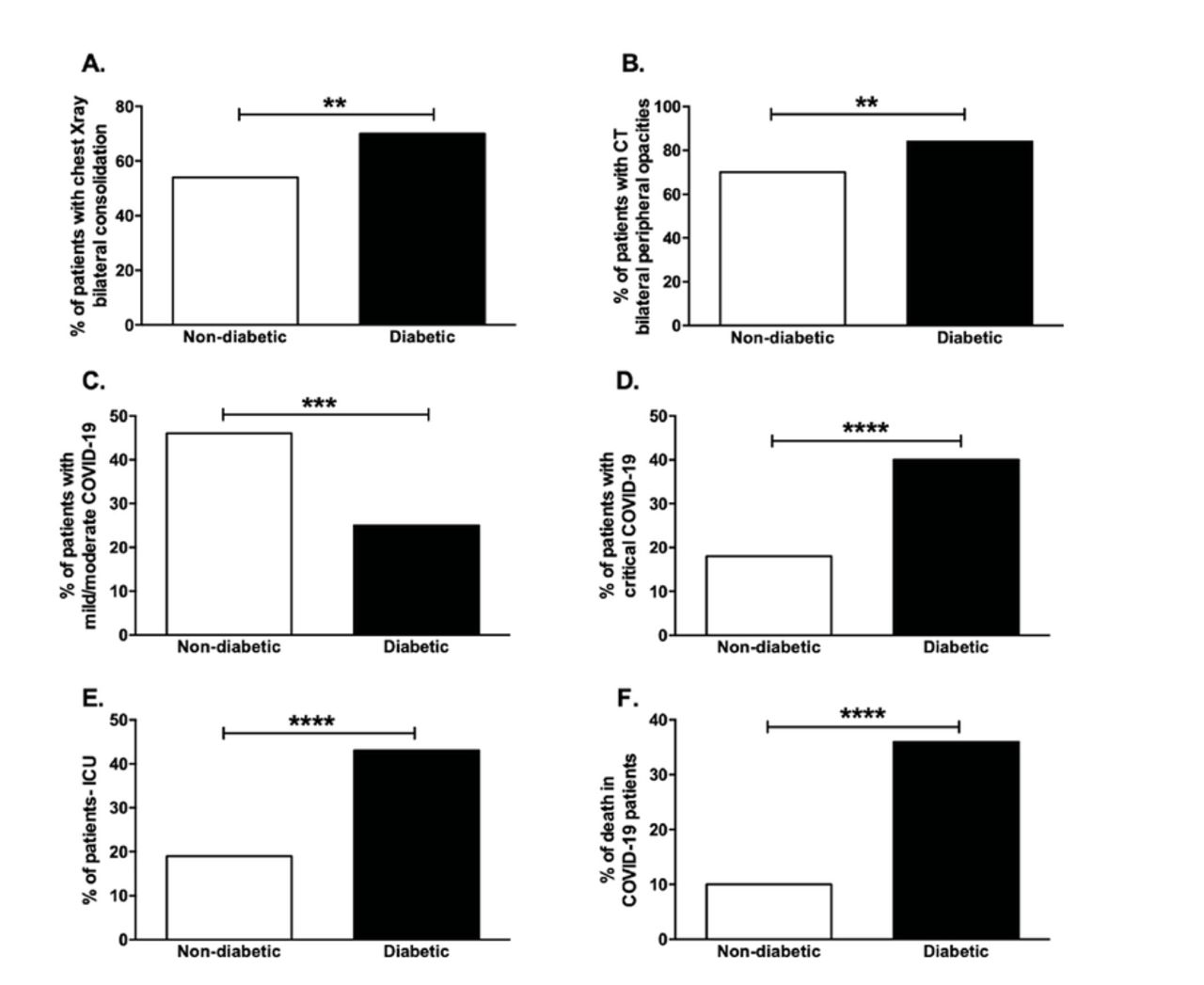
The main affected organ during the course of COVID-19 infection is the lung. Our data show that diabetic COVID-19 patients displayed more bilateral airspace consolidation in their chest x-ray (70% in diabetic versus 54% in non-diabetic, p<0.01, Figure 4A) and more bilateral peripheral ground-glass opacities as shown in the CT scans (84% in diabetic versus 70% in non-diabetic, p<0.01, Figure 4B). Cumulatively, diabetic COVID-19 patients exhibit more signs of pulmonary damage as complications of COVID-19 infection (summarized in Table 2).
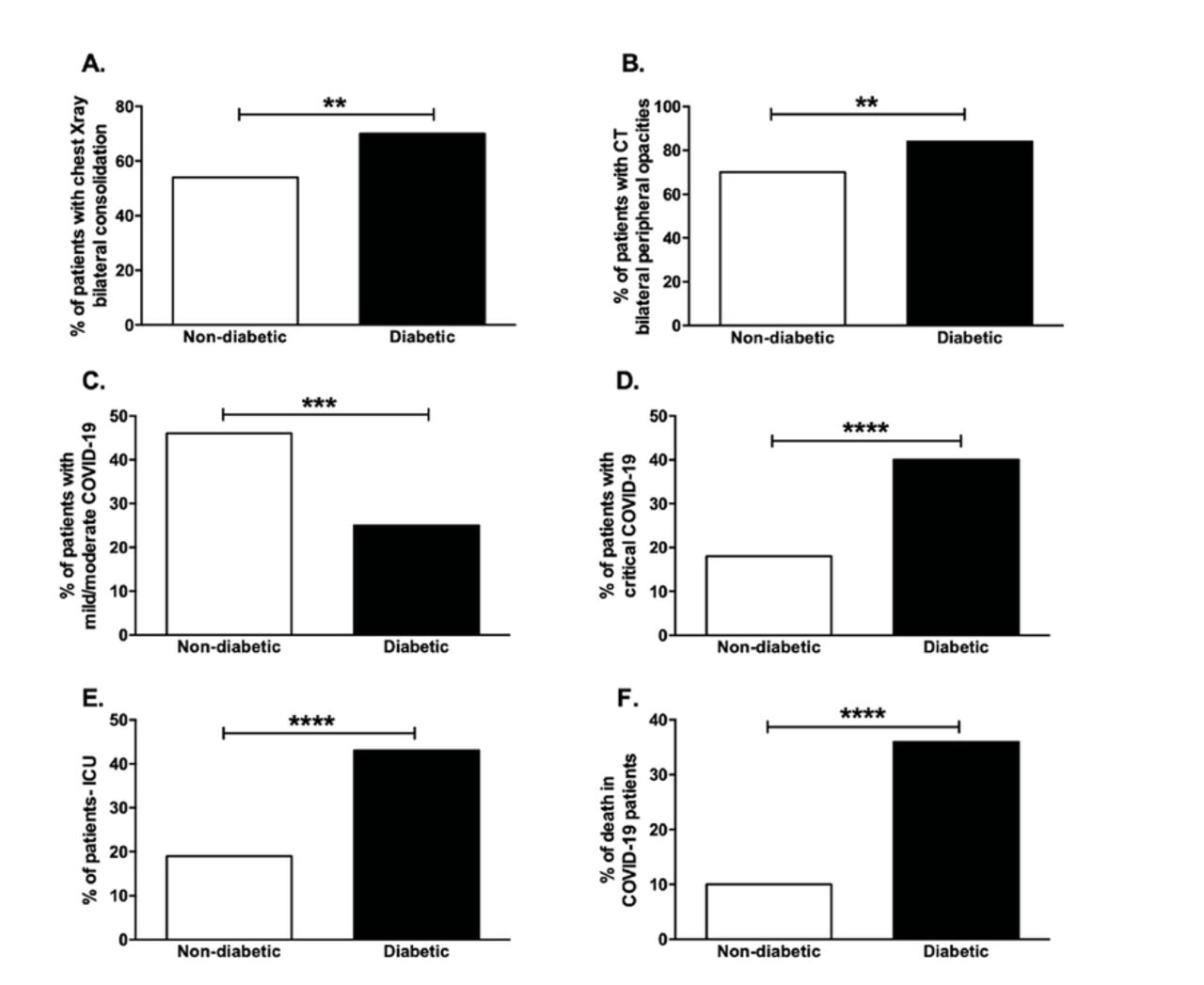
- Radiological assessment and clinical outcomes of diabetic COVID-19 patients. The percentage of patients with A) chest x-ray showing bilateral consolidation and B) CT scan showing bilateral peripheral ground-glass opacities was compared in diabetic and non-diabetic COVID-19 patients. The percentage of COVID-19 patients with C) mild/moderate and D) critical clinical outcome as well as the percentage of E) those admitted to ICU and F) death in COVID-19 were compared in diabetic and non-diabetic groups *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001
Clinical outcomes in diabetic COVID-19 patients
Since diabetes is associated to be a comorbidity and risk factor of COVID-19, it was important to investigate the differences in the severity of COVID-19. Our data showed that there was a lower percentage of mild/moderate (25% in diabetic versus 46% in non-diabetic, p<0.001, Figure 4C) and a concomitant higher percentage of critical (40% in diabetic versus 18% in non-diabetic, p<0.0001, Figure 4D) COVID-19 cases in the diabetic group. This further explains that there was a higher percentage of ICU cases (43% in diabetic versus 19% in non-diabetic) and death cases (36% in diabetic versus 10% in non-diabetic) in the diabetic group of COVID-19 patients (both p<0.0001, Figures 4E & 4F). However, there was no significant difference in the duration of COVID-19 illness before presentation to the medical care between the diabetic and non-diabetic COVID-19 subjects (data not shown in Table 4).
- Illness severities and clinical outcomes of the diabetic and non-diabetic COVID-19 patients.
Disease severity markers in diabetic COVID-19 patients
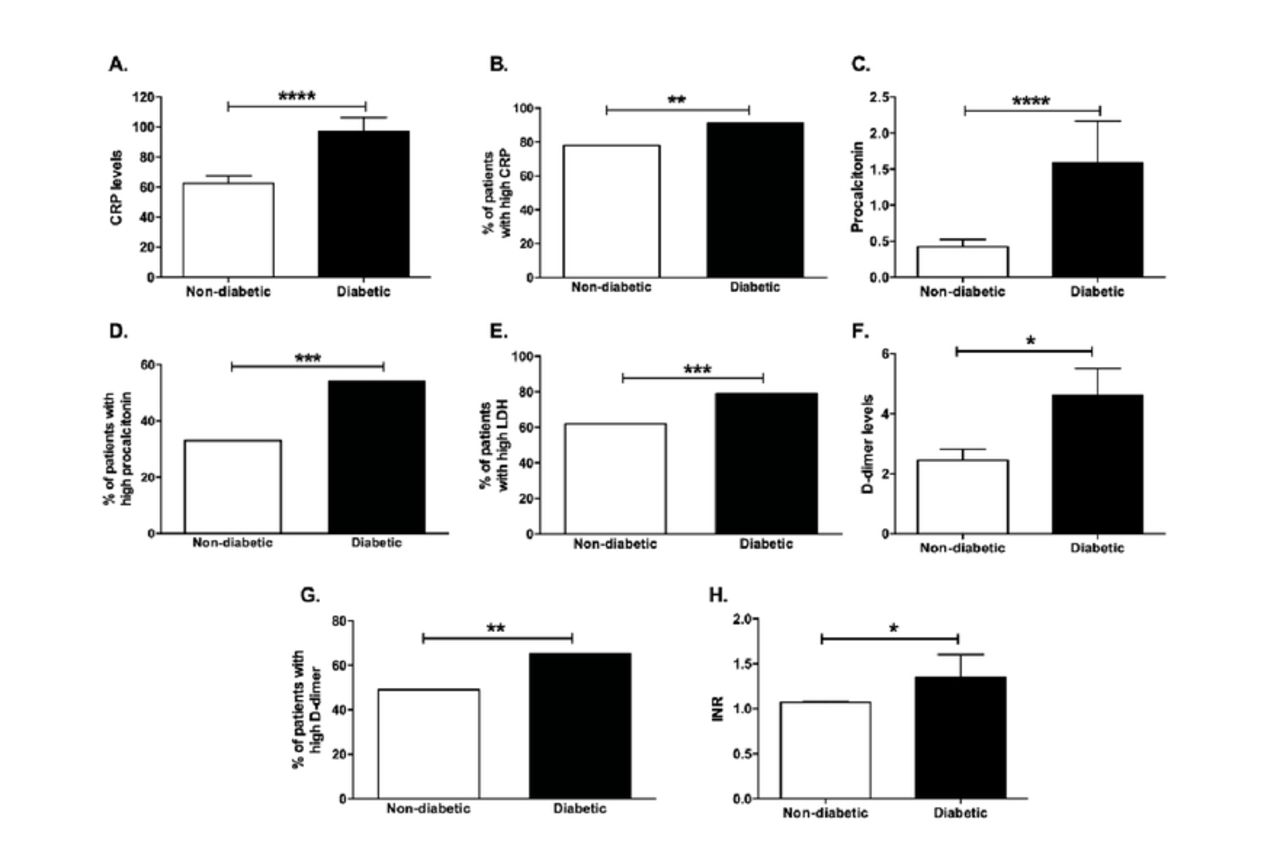
One of the markers that is crucial for assessing inflammation and infection, is CRP. As shown in Figures 5A & 5B, the CRP levels were significantly higher in the diabetic group (97.23±96.39) compared to the non-diabetic (62.45±79.65, p<0.01) COVID-19 patients, indicating that they have more severe forms of COVID-19 infection. Likewise, procalcitonin, an infection marker, was significantly elevated in diabetic COVID-19 patients (diabetic: 1.587±5.974, non-diabetic: 0.4242±1.474, p<0.01, Figures 5C & 5D). Along with that, a higher percentage of diabetic COVID-19 patients had high blood levels of LDH (79% in diabetic versus 62% in non-diabetic, p<0.001), as shown in Figures 5E.

- Disease severity and coagulation markers in COVID-19 patients. A) CRP, C) procalcitonin, F) D-dimer, and H) INR levels in diabetic and non-diabetic COVID-19 patients. The percentage of patients with B) high CRP, D) high procalcitonin, E) high LDH, and G) high D-dimer in diabetic compared to non-diabetic COVID-19 patients. *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001
Since diabetes could be a cause of vascular complications, it was interesting to assess some of the coagulation markers. D-dimer levels were significantly higher in diabetic COVID-19 patients (diabetic: 4.612±9.093, non-diabetic: 2.449±5.062, p<0.05), as shown in Figures 5F & 5G. Other coagulopathy blood tests revealed that there was a significant increase in the INR of diabetic COVID-19 patients (diabetic: 1.349±2.566, non-diabetic: 1.070±0.1523, p<0.05, Figure 5H). However, there was no significant difference in platelet levels between the diabetic and non-diabetic COVID-19 patients.
Discussion
Diabetes has been reported as one of the comorbidities for disease progression and mortality of COVID-19.13,14 Since UAE has a high prevalence of diabetes,22,23 and it has been recently reported by the official government press release that 40% of the UAE’s COVID-19 fatalities had diabetes, then it was crucial to look at the differences among the diabetic and non-diabetic COVID-19 patients. Diabetes could present a risk factor due to the increase in the serum ACE2 as shown in non-obese diabetic (NOD) mouse model as well as DM patients.25,26 Additionally, patients taking inhibitors of angiotensin-converting enzyme (ACEIs) and angiotensin II receptor blockers (ARBs) had an overexpression of ACE2, the known entry receptor for SARS-CoV-2.27
Gender differences were previously reported to affect the clinical outcomes and mortality of SARS-CoV-2 infected individuals, where males were at a higher risk than females.28 This was further supported by the findings in this study, where the number of male subjects was twice as many as the female COVID-19 subjects. Additionally, the diabetic patients belonged to an older age group, thus posing another risk factor that could increase their susceptibility to COVID-19 infection.29 The topmost comorbidity associated with COVID-19 is hypertension;30 thus, it was not surprising to find that diabetic patients had associated risk factors such as hypertension. It seems that comorbidities (diabetes and hypertension) make the patients more vulnerable in comparison to other risk factors including travel history and contact with COVID-19 patients.
Not only that, diabetic COVID-19 patients show more severe and profound clinical symptoms including fever and SOB, which is further confirmed by high levels of LDH levels as a sign of reduction of oxygen saturation in those patients. This was accompanied by pulmonary defects such as chest x-ray bilateral airspace consolidation and CT ground-glass opacity, pointing out that diabetic COVID-19 patients exhibit more signs of pulmonary damage as complications of COVID-19 infection. This goes in line with previous data where diabetic patients exhibited diverse multifocal features in their CT lung images.31 This could be attributed to microvascular damage in diabetes that leads to a complicated alveolar-capillary network in the lungs.32 Another reported piece of evidence indicating vascular complications and coagulation dysfunctions in diabetes was the increased levels of the coagulopathy markers D-dimer and INR, where D-dimer was previously linked to high mortality rates of COVID-19.33
There has been a strong association between diabetes and COVID-19 severity,34 which was further supported by our data where an increase in the percentage of critical, ICU and death was observed in the diabetic COVID-19 cases. Our findings go in line with data reported by Soliman35 where diabetic patients showed a more critical presentation as well as higher ICU admission. Furthermore, the results of this study match the retrospective cohort study carried out in Wuhan, China in terms of laboratory, radiologic, complications, and clinical outcomes on diabetic COVID-19 patients.36
Blood/serum laboratory tests such as CRP, procalcitonin, and LDH were previously described as reliable biomarkers for the probability and degree of infection and inflammation especially in COVID-19.37-39 In this study, the levels of these markers were much higher in the diabetic group of COVID-19 patients.Also, high serum ferritin was observed which goes in line with previous data where individuals with diabetes exhibited elevated serum ferritin levels and hence have a higher probability to experience serious complications from COVID-19.40 Other blood indicators include the disproportionality of WCC such as lymphopenia and neutrophilia that have been linked to COVID-19 diagnosis and prognosis.5,41 Indeed, lymphopenia, neutrophilia, and an increase in WCC was more profound in diabetic COVID-19 patients compared to non-diabetics. Cumulatively, these findings indicate that patients with diabetes have a more severe form of COVID-19 infection.
SARS-CoV-2 was reported to induce hemolysis leading to reduced hemoglobin and hence oxygen transport.42 Anemia is a common clinical feature of diabetic patients,43 and this supports our findings where COVID-19 diabetic patients had a much lower Hb compared to non-diabetics. Additionally, this decline in Hb level might be attributed to the conversion of Hb to glycosylated hemoglobin HbA1c, a known marker in the blood of patients with diabetes.44 Chronic kidney disease was associated with severe forms of COVID-19 infection.45 Besides, kidney damage could occur as a complication of diabetes.46 Hyponatremia, hyperkalemia, increased blood urea and creatinine, lowered eGFR,and hypoalbuminemia were reported in diabetic COVID-19 subjects, other possible reasons for reaching critical stages of the infection.
Study limitation
One limitation of this study could be the absence of investigating the effect of the control of sugar levels in diabetic patients in COVID-19 infection.
In conclusion, diabetic patients showed more severe symptoms that could lead to critical clinical outcomes of COVID-19 infection and cause ICU admission or even death.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. Dr. Fahda Alokaily is a member of the Editorial Team, and was therefore excluded from any final editorial decisions regarding this paper.
- Received December 23, 2020.
- Accepted January 12, 2021.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.