


Abstract
Objectives: To investigate trends in hemoglobinopathies following the establishment of a mandatory premarital screening program (MPMSP) in the southern region of Saudi Arabia, where they are considered highly predominant.
Methods: A retrospective analysis was performed on data from 32,130 high-performance liquid chromatography (HPLC) tests between November 2017 and October 2020. The data was obtained from the Hematology section, Laboratory Department, Armed Forces Hospital, Southern Region.
Results: Despite the establishment of the MPMSP, our data showed that sickle cell disease remains a predominant hemoglobinopathy accounting for more than 7% of total tests in Southern Saudi Arabia. Observed HPLC hemoglobin fractions among the tested population showed a reduction in Hb A mean indicating a high rate of hemoglobin abnormalities. In addition, the prevalence of hemoglobin variants, including sickle cell and thalassemia, was higher in the younger population born after the MPMSP than in older subjects.
Conclusion: Even with the implementation of the MPMSP, hemoglobin abnormalities remain prevalent in southern Saudi Arabia. A longer time frame is recommended to verify the validity of the program.
Hemoglobinopathies are a group of relatively common inherited disorders caused by either quantitative or qualitative defects in hemoglobin (Hb) synthesis. According to the World Health Organization, people carrying hemoglobinopathies constitute more than 5% of the human population; 300,000-400,000 children are born yearly with very serious hemoglobinopathies.1,2 Although hemoglobinopathies were originally found only in the Middle East and in areas of Asia and Africa, the enormous migration of people between countries has led to hemoglobinopathies being spread all around the world.3 Nonetheless, the Kingdom of Saudi Arabia (KSA) still has a large population with hemoglobinopathies, and is even considered to have the highest incidence among countries in the Middle East.4
The Hb molecule has 2 parts, heme, and globin; the latter consists of 2 α-like and 2 β-like globin chains, the portion affected in hemoglobinopathies. Among hemoglobinopathies, the most common types are thalassemia and sickle cell anemia (SCA), where KSA is considered to have the highest prevalence rate among regions in the Middle East.5 Sickle cell anemia poses a continuous significant cause of elevated mortality and morbidity in KSA,6 while data concerning the mortality rate associated with thalassemia in the country are yet lacking.7 Thalassemia is caused by defective production or complete absence of globin and is divided into 2 types according to which type of globin is affected: α-thalassemia (α-Thal) and β-thalassemia (β-Thal). Within the α-Thal type, there are 4 subtypes, defined by the number of genes deleted: α-Thal silent (only one gene), thalassemia trait or minor (2 genes), Hb H (3 genes) and Hb Bart’s (4 genes).8 The β-Thal type can be divided into minor and major, with β-Thal minor resulting from only one gene being impaired and β-Thal major (also termed β-Thal disease) from the reduction or complete absence of both genes.9 Patient outcomes in thalassemia can be improved through better management by healthcare providers. Currently available strategies include transfusion therapy, using iron chelators to prevent iron overload, increasing Hb F production, and splenectomy.10 Meanwhile, SCA is the most common genetic blood disorder. It is characterized by the glutamic acid at the sixth amino acid position in the β-globin gene being replaced by the less polar amino acid valine, which decreases Hb solubility and causes it to become easily polymerized when deoxygenated.11 Those having Hb S/Hb A status are termed carriers. The carrier state is normally asymptomatic, but there is growing evidence of possible organ damage among older carriers;12 meanwhile, sickle cell disease (SCD) may cause serious health issues and become life-threatening.11 Unfortunately, even with superior care being provided, life expectancy in cases of SCD is still reduced by 30 years.13 Management strategies that can be used for SCD include reducing crisis rates with hydroxyurea, regular erythrocyte transfusion, and stem cell transplantation.10,13
High-performance liquid chromatography (HPLC) has become the method of choice for screening or confirmation of hemoglobinopathies.14 The developed method provides sensitive, specific, and reproducible results that, in combination with family history and hematological parameters, help physicians to confirm diagnosis of a hemoglobinopathy.15 In addition, HPLC is important for investigating the prevalence of hemoglobinopathies, which in turn aids the management and prevention of these diseases. As mentioned, KSA is a country known to have higher prevalence of hemoglobinopathies, and several studies have examined their prevalence in various cities throughout the country. A retrospective study based on premarital screening by Memish and Saeedi examined the prevalence of SCD and β-Thal over a 6-year period, identifying a total of 70,962 SCA patients, which comprised 4.5% of all examined people.4 β-thalassemia was identified as having a prevalence of 1.8% (29,006 patients) among tested people, confirming higher prevalence of hemoglobinopathies in the Saudi population.4 Yet another study examined the prevalence of SCD and β-Thal in KSA using data obtained from premarital screening and genetic counseling programs (PMSGC), determining rates of approximately 49.6 SCA patients and 13.6 β-Thal patients for every 1000 people examined.5 Although studies have shown the prevalence to decrease over time, those numbers are still considered to be high. Within KSA, the eastern and southwestern areas are known to have the highest prevalence.16 Several countries have implemented different programs to increase hemoglobinopathies awareness among the population and control the prevalence of hemoglobin abnormalities; for example, thalassemia awareness campaigns have been successfully implemented in Cyprus, Greece, and Italy.17 In Italy, however, the campaigns and premarital counseling led only to a temporary reduction in thalassemia cases in the 70-80s.17 In Sardinia, several strategies seeking to control the prevalence of hemoglobinopathies have been implemented by providing a hub and spoke network along with introducing education on thalassemia in secondary school. Premarital screening and genetic counselling programs were established and implemented in 8 middle eastern countries. This program offers premarital genetic counseling to couples at risk for hemoglobinopathy disorders and is considered as a mandatory step before receiving a marriage license.18 The program was first introduced in KSA in 2001 and become mandatory by 2004.5 Following launching the program, KSA showed a marked reduction in the number of at-risk marriages and predict to observe a considerable decrease in the burden of the genetic disease in the upcoming years.5 The present study examined current prevalence rates in the Southern Region using HPLC data obtained from the Armed Forces Hospital. Data from this study may help in developing current plans to assess the prevalence rate of hemoglobinopathies in the Southern Region.
Methods
The retrospective study was carried out in the Department of Hematology, Armed Forces Hospital, Southern Region, KSA. A total of 32,780 tests examined using HPLC, (Variant II™, β-Thalassemia Short Program; Bio-Rad Laboratories, Hercules, CA, USA) from November 2017 to October 2020 were extracted from the digital archives of general screening in the Hematology Unit of the Department of Laboratory of a reference hospital that provides medical services for Ministry of Defense employees in the Southern Region of KSA. To prevent false-positive Hb S and thalassemia, subjects less than 6 months old were excluded, leaving 32,130 included tests. The total tests by year were as follows: November 2017 to October 2018 was 9701; November 2018 to October 2019 was 13950; November 2019 to October 2020 was 8481. Diagnosis of Hb variants was made according to the Hb Variant Interpretation Guide by the Department of Hematology, Armed Forces Hospital, Southern Region, KSA.
Subjects having an A2 value of more than 4% but less than 10% were considered to have possible β-Thal traits, while subjects having an F value of more than 45% with no Hb A fraction detected were considered to have possible β-Thal major. Participants that were H-prep positive were considered to have α-Thal. Those with an S value of less than 45% and without transfusion history were considered to have the sickle cell trait, and those with an S value of more than 45% as having sickle cell disorder. The population with the β-Thal trait may include some cases with the Hb S trait, as Hb A2 may rise in both. S-β-Thal is suspected if % Hb S is >% Hb A, and not on % Hb S alone.
The inclusion criteria comprised all HPLC tests performed in the Hematology Unit of Armed Forces Hospital in the Southern KSA from November 2017 to October 2020. The exclusion criteria comprised all results for individuals less than 6 months old.
Ethical approval (Rec-No: AFHSRMREC/2020/Clinical Lab Sciences/441) for this study was obtained from the Ethics Committee of the Armed Forces Hospital, Southern Region, KSA. The data of this retrospective study was extracted from the Department of Hematology, Armed Forces Hospital, Southern Region, KSA.
GraphPad Prism was used for analyses (GraphPad Prism version 9.00 for Mac, GraphPad Software, San Diego CA). Data were represented as numbers, percentages, mean and median.
Results
Data showed that SCD was much more prevalent among tested cases than β-Thal major during the 3-year study period (Table 1). Results of observed HPLC hemoglobin fractions were presented in Table 2 showing that Hb A mean is reduced indicating for increased rate of Hb abnormalities. The prevalence rate of Hb abnormalities including SCD, sickle cell trait, β-Thal major, and β-Thal minor varied throughout the study period, shown in Table 3. While November 2018 to October 2019 included a much higher number of tests than the other 2 years, the percentage of positive tests less varied between years.
- Prevalence rates for sickle cell disease and beta-thalassemia major in Southern Region, Saudi Arabia from November 2017 to October 2020.
- Observed High-performance liquid chromatography (HPLC) hemoglobin fractions among the tested population over 3 years from November 2017 to October 2020.
- Prevalence rates for sickle cell disease, sickle cell trait, ß-thalassemia major and ß-thalassemia minor over time in Southern Region, Saudi Arabia from November 2017 to October 2020.
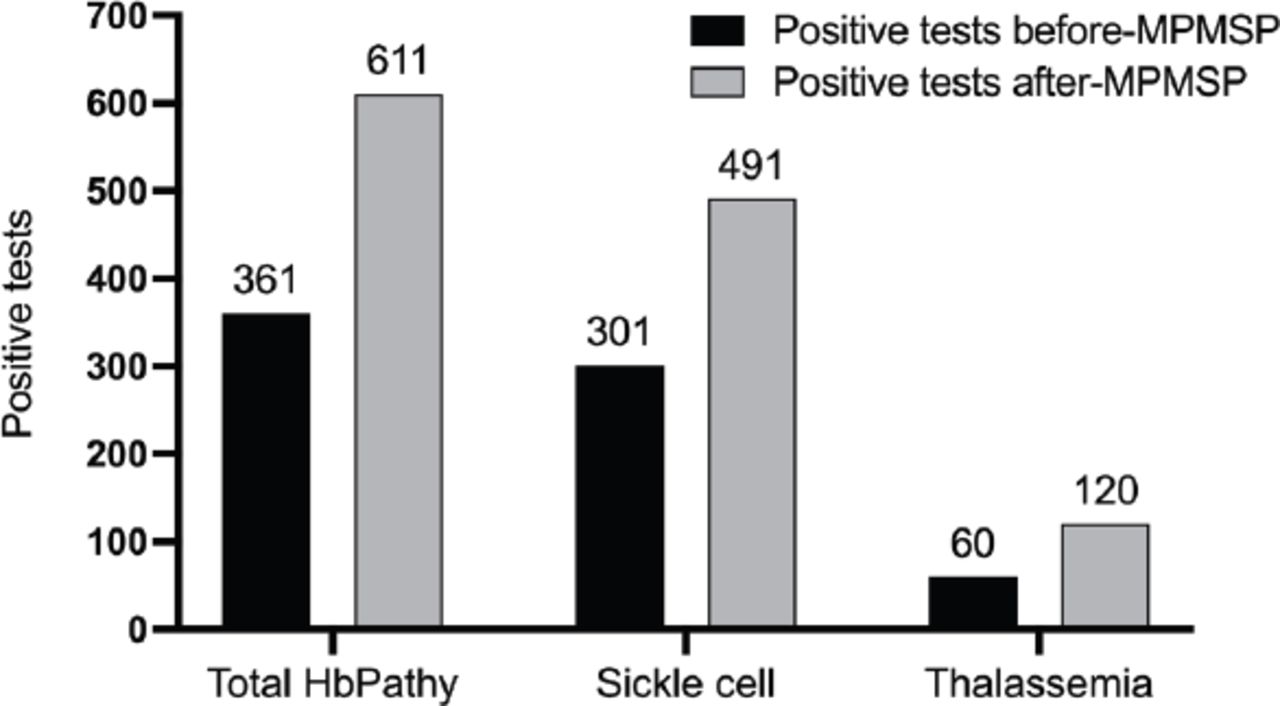
Figure 1 compares the prevalence of positive tests for Hb abnormalities before and after implementation of the mandatory pre-marital screening program (MPMSP). The results were surprising as Hb S and thalassemia showed an increase in prevalence among subjects born after initiation of the program. Specifically, 8.8% had Hb S and 2.1% had thalassemia after program start, compared to 5.4% and 1.1% respectively before its establishment.

- Comparison of prevalence rates for hemoglobin (Hb) abnormalities between positive tests before and after establishment of the mandatory premarital screening program (MPMSP).
Discussion
Genetic disorders causing Hb abnormalities are by far the most common monogenic diseases. Children having serious Hb disorders are born each year in middle-income countries.19 Among Middle Eastern countries, KSA is considered to have a high rate of Hb disorders,5 with SCD and β-thal being particularly common and highly observed in the eastern and southern regions of KSA.5 As hemoglobinopathies are among the most serious and costly disorders, the government of KSA established the PMSGC program in 2004, which aims to improve quality of life, reduce the incidence of these disorders, and even eradicate Hb abnormalities from the Arabian Peninsula.5 The present study set out to evaluate trends in disease rate and provide an update on Hb disorders in one of the regions where they are most highly prevalent. To this end, data were obtained from HPLC screening tests performed from 2017 to 2020 at one of the biggest hospitals in the Southern Region. These data comprise the total number of requested tests, and include age, genderr, and Hb variant status. Thus, it is possible to predict trends in disorder prevalence following the establishment of the program.
Recent studies have investigated the prevalence of Hb abnormalities in several regions.5,20,21 Interestingly, Alsaeed et al examined the distribution of disorders throughout KSA on a large cohort obtained from 2011 - 2015 PMSGC data and observed a reduction in those with β-thal traits over the 5-year study period. The same study identified a β-thal prevalence of 13.6 per 1000, 12.9 per 1000 for β-thal trait, while the prevalence of β-thal major was 0.7 per 1000.5 Sickle cell disease had a higher prevalence than β-thal, and furthermore remained constant from 2011 to 2015.5 Our study observed a higher prevalence for Hb S than for thalassemia, which is consistent with the prior report.
In the present study, we aimed to investigate trends in Hb disorders in a region where genetic defects in Hb are prevalent. A total of 32,130 HPLC tests were requested during the 3-year study period. Sickle cell disease was more prevalent than β-thal, comprising 7.2% (n=2301) versus 0.01% (n=5) of the total tests obtained. Additionally, as the MPMSP in KSA was established by 2004, we specifically investigated the presence of Hb variants in subjects ≤17 years old to predict the possible prevalence of Hb disorders following initiation of the program. The program is obligatory for obtaining a marriage license and tends to increase awareness of Hb disorders among couples seeking to get married. As such, the prevalence of Hb disorders was expected to decline in the years following 2004. However, the observed rate of Hb variants in subjects aged ≤17 years old was high, being nearly double that from before the MPMSP (10.9% compared to 6.5%). This increase is not consistent with the program objectives but aligns with the findings of a prior study.5 The discrepancy between these findings and the MPMSP objectives might be due to several factors, including consanguineous marriage, which is known to be common in the southern region of KSA. Furthermore, the program cannot restrain couples who decide to marry even when approval is not granted. However, we cannot conclude that the actual rate is higher, as offspring born after initiation of the MPMSP might have parents who married before 2004.
The persistent high prevalence may be attributable to allowing couples who have unsuccessful premarital screening for hemoglobinopathies to marry even if they are not granted a permit or marriage certificate. Such cases are common among families who find premarital screening inappropriate for social and/or religious reasons, and this practice can reduce the benefit of prenatal diagnosis, as abortion is not widely accepted among families in KSA.
Although our data relied on one resource, the Armed Forces Hospital, Southern Region, they provide an important update to observations as the hospital receives patients from all southern-region cities, including Jazan, where sickle cell anemia is predominant.
Study limitations
The primary limitation of this study was its shorter timeframe due to limitations in accessing data for previous years. Though our retrospective analysis was performed on provided HPLC tests over 3 recent years, further studies on larger sample size and a longer timeframe starting from the establishment of the MPMSP may adequately observe the outcomes of MPMSP. Another limitation concerns the unavailability of hematological data as the majority of hemoglobinopathies are characterized by anemia of ranging degrees.
In conclusion, this study investigated the prevalence of hemoglobinopathies in the southern region of KSA after the MPMSP was made obligatory for obtaining a marriage license. The disorders trended higher in younger subjects born after 2004. This study provides an update on the status of Hb disorders and extends our knowledge of trends with respect to prior reports. Further studies spanning a longer time frame are recommended to verify the outcomes of the PMSGC program.
Acknowledgment
The authors are grateful to the Department of Laboratory, Armed Forces Hospital, Khamis Mushayt, Saudi Arabia for their cooperation in this study. The authors would like to thank Servicescape (www.servicescape.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 6, 2021.
- Accepted June 6, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.