


Abstract
Objectives: To evaluate the diagnostic utility of self-collected saliva in coronavirus desease-19 (COVID-19) screening procedures.
Methods: A total of 6 databases were reviewed from their inception until August 2021. Sensitivity and specificity were measured by extracting items (true-positive, true-negative, false-positive and false-negative) from each paper. We evaluated the diagnostic accuracy based on Quality Assessment of Diagnostic Accuracy Studies, version 2.
Results: A total of 41 studies were included in the final analysis. The diagnostic odds ratio (OR) of self-collected saliva was 196.2022 (95% confidence interval [CI]: 117.8833-326.5546). The area under the summary receiver operating characteristic curve was 0.955. For detecting COVID-19, self-collected saliva had a moderate sensitivity of 0.8476 [0.8045-0.8826] and positive predictive value of 0.9404 [0.9122-0.9599] but high specificity of 0.9817 [0.9707-0.9887] and negative predictive value of 0.9467 [0.9130-0.9678]. In a subgroup analysis, the diagnostic accuracy of self-collected saliva tended to be higher for symptomatic (vs. asymptomatic) examinees.
Conclusion: Although naso/oropharyngeal swab tests are the most accurate and important diagnostic tools, the saliva-based testing method can be used as a suitable alternative test, with the advantages of increased patient convenience, efficient testing, and the need for fewer medical staff and resources. In particular, simple collecting method such as drooling or spitting without coughing would be effective in evaluating the symptomatic patients.
PROSPERO no.: CRD42021279287
Since first detected in 2019, the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic is still ongoing. This newly discovered coronavirus has a high ability to be transmitted from person to person through respiratory aerosols, droplets, or vomitus.1 More than 80% of patients infected by coronavirus disease-19 (COVID-19) show symptoms similar to influenza infection or pneumonia. Therefore, most patients do not require hospitalization.2 Because of these features of COVID-19, significant viral transmission from mildly symptomatic and non-hospitalized patients is concerning.3 However, COVID-19 can cause severe morbidity or mortality in the elderly, immunocompromised patients, and those with comorbidities such as heart disease, obesity, and diabetes.4
Although there are a few known treatments for COVID-19, strict isolation of confirmed patients based on accurate diagnosis of COVID-19 is the key to overcome the pandemic, given the circumstances that only few treatment methods are available.5 Generally, the definitive diagnostic test of COVID-19 relies mostly on detection via reverse transcription quantitative polymerase chain reaction (RT-qPCR) carried out in respiratory samples.6 However, the collection of naso/oropharyngeal swab samples can cause nasal pain to the examinees, and health care personnel performing the test should be equipped with individual protective equipment to protect them against the risk of virus exposure.7 Testing using self-collected saliva methods have been reported to have several advantages of convenience and safety compared with the naso/oropharyngeal swab method because it eliminates close contact when obtaining a sample and the necessity of personal protective equipment. In addition, saliva collection is painless and thus, minimizes inconvenience for the examinees.8 Recently, published studies have reported that saliva specimens could be an alternative to naso/oropharyngeal specimens, but the evidence is still limited.9 It is important to clarify the diagnostic power of saliva for COVID-19 to improve the convenience to examinees and inspectors when mass rapid examination is required. Therefore, the aim of this study was to define the diagnostic accuracy of RT-qPCR from saliva compared to naso/oropharyngeal swab results.
Methods
This meta-analyses and systematic reviews used terms such as COVID-19, coronavirus, coronavirus disease-19, severe acute respiratory syndrome coronavirus-2, saliva, nasopharyngeal swab, oropharyngeal swab, PCR, and diagnostic accuracy as keywords. Database from PubMed, the Cochrane Central Register of Controlled Trials, Embase, Web of Science, SCOPUS, and Google Scholar were searched. Only papers written in English were reviewed. All references of the included articles were assessed to confirm that no significant studies were neglected. Two reviewers independently reviewed candidate studies, conducted title, abstract, full-text reviews, and inclusion of the final agreed papers.
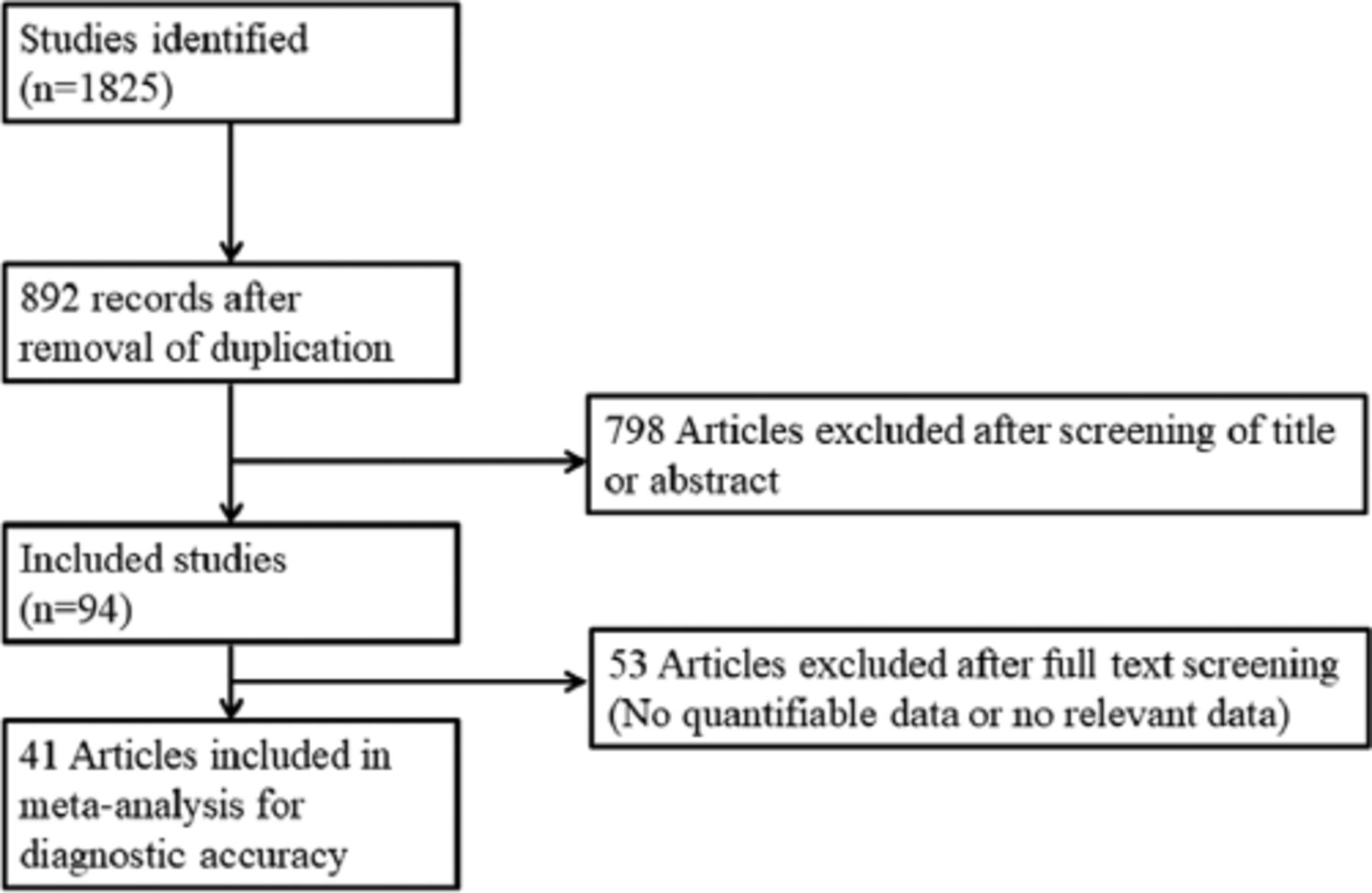
The present study includes: i) prospective or retrospective study protocol; from ii) cases of COVID-19 suspected symptoms or asymptomatic population screening, using iii) index test: RT-qPCR in self-collected saliva specimens to detect SARS-CoV-2, with iv) reference standard (comparator test) of RT-qPCR in naso/oropharyngeal specimens to detect SARS-CoV-2, and v) qualified articles for sensitivity and specificity analysis (Appendix 1). We excluded reviews, case reports, and studies with low diagnostic power in saliva specimens. The search flow diagram was presented in Figure 1.
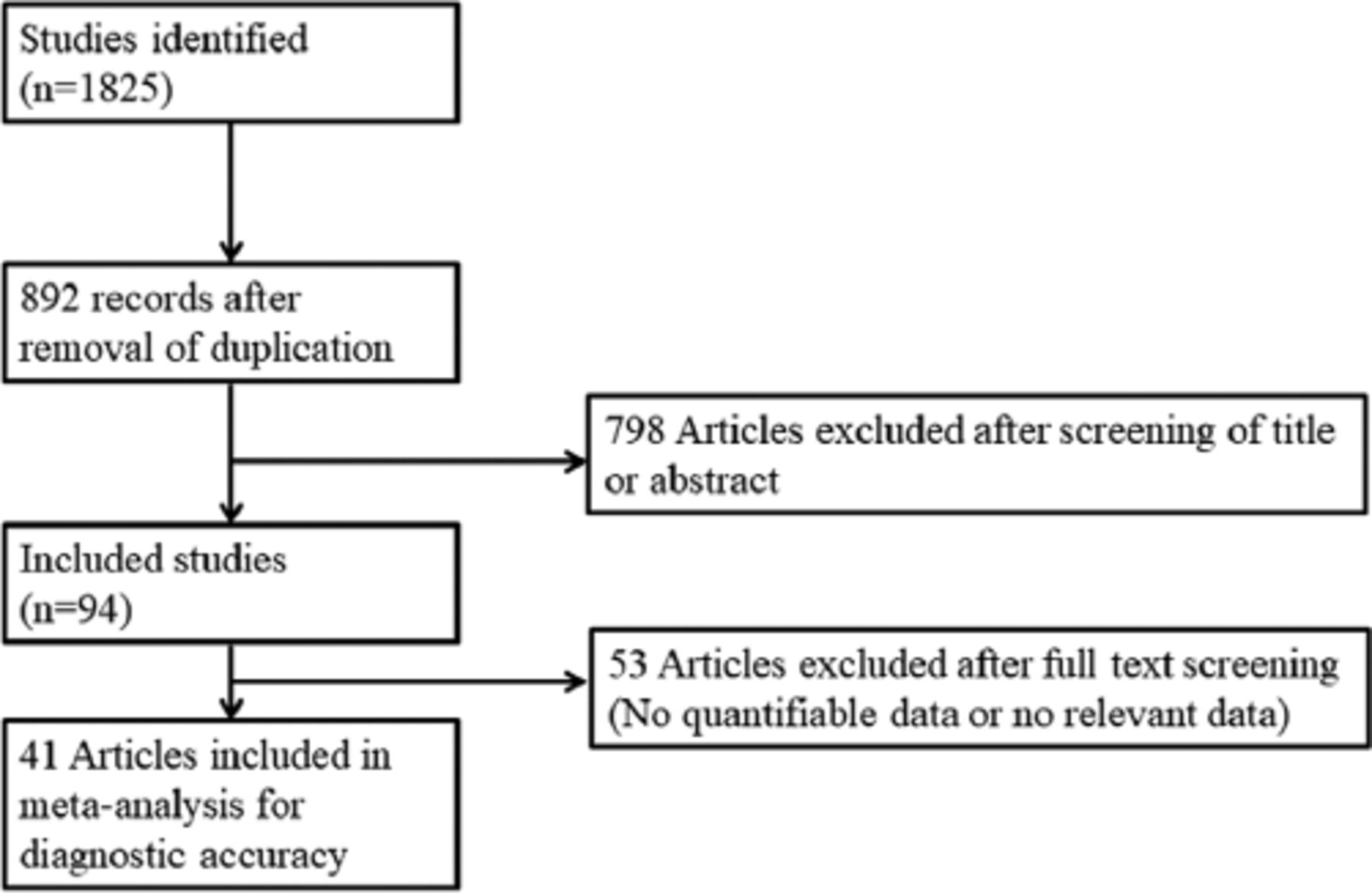
- Summary of the search strategy.
We calculated the area under the curve (AUC) of summary receiver operating characteristic (SROC) curve designed from diagnostic accuracy (namely, diagnostic odds ratio [DOR]).7,8,10-48
Diagnostic odds ratio was defined as true positive x true negative / false positive x false negative, within 95% confidence interval (CI) from a random effect model with intra- and inter-study variations. The higher the value of DOR, the better the performance of the diagnostic method. Diagnostic odds ratio of one means it is not assured whether the disease is present. We calculated the log of DOR to examine an approximate normal distribution.49 The SROC method derives both sensitivity and specificity through meta-analysis. The SROC curve moves towards the left upper quadrant (namely, sensitivity and specificity to 1 [100%]) as the discriminative force increases. Area under the curve ranges from 0-1 with higher value indicating superior performance. We estimated and compared the accordance of RT-qPCR results between the saliva and naso/oropharyngeal swab samples using Cohen’s kappa coefficient (κ). Data of true-positive, true-negative, false-positive, and false-negative values used to calculate the AUC and DOR were collected. The qualitative agreement across sample types (naso/oropharyngeal swab and saliva specimen) was assessed.
Quality examination was carried out by Quality Assessment of Diagnostic Accuracy Studies tool, version 2.
Statistical analysis
We used the version 3.6.1 of R software for statistical analysis (R Foundation for Statistical Computing, Vienna, Austria) and Q statistics for homogeneity analysis. Citation management was conducted by EndNote version 20.1 (Clarivate Analytics, PA, USA). Summary receiver operating characteristic curves were drawn from forest plots of sensitivity, specificity, negative predictive value (NPV), and positive predictive value. Coefficients were converted to Fisher’s exact values for normal distribution and variance stabilization between different sample types. After completing the meta-analysis, Fisher’s exact values were converted back to the intra-class correlation coefficient to aid in the interpretation of the results.50
Results
The present meta-analysis included 41 studies of 14,011 patients. Appendix 2 summarizes the participant characteristics and Appendix 3 shows the quality analysis of methods.
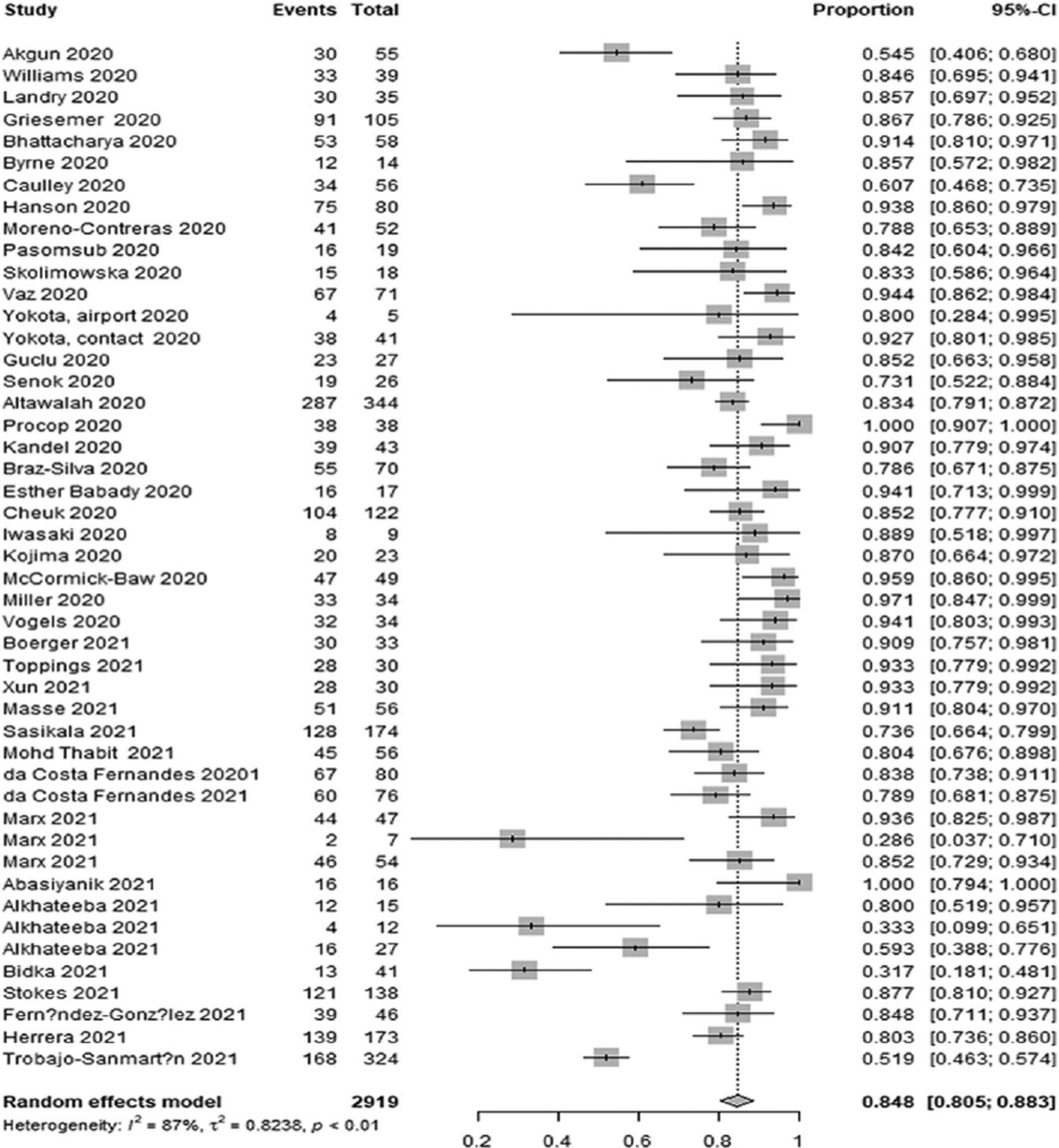
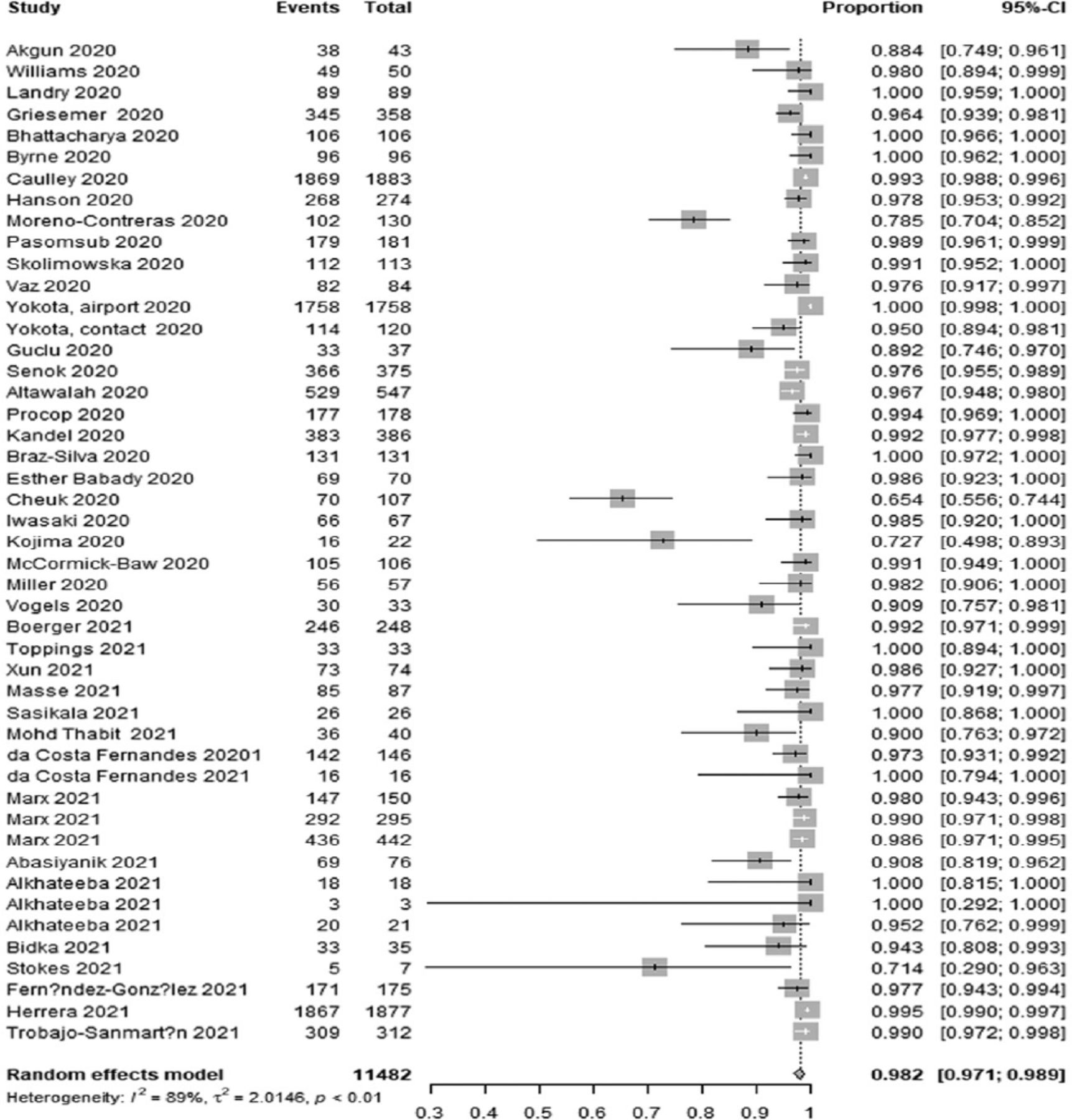
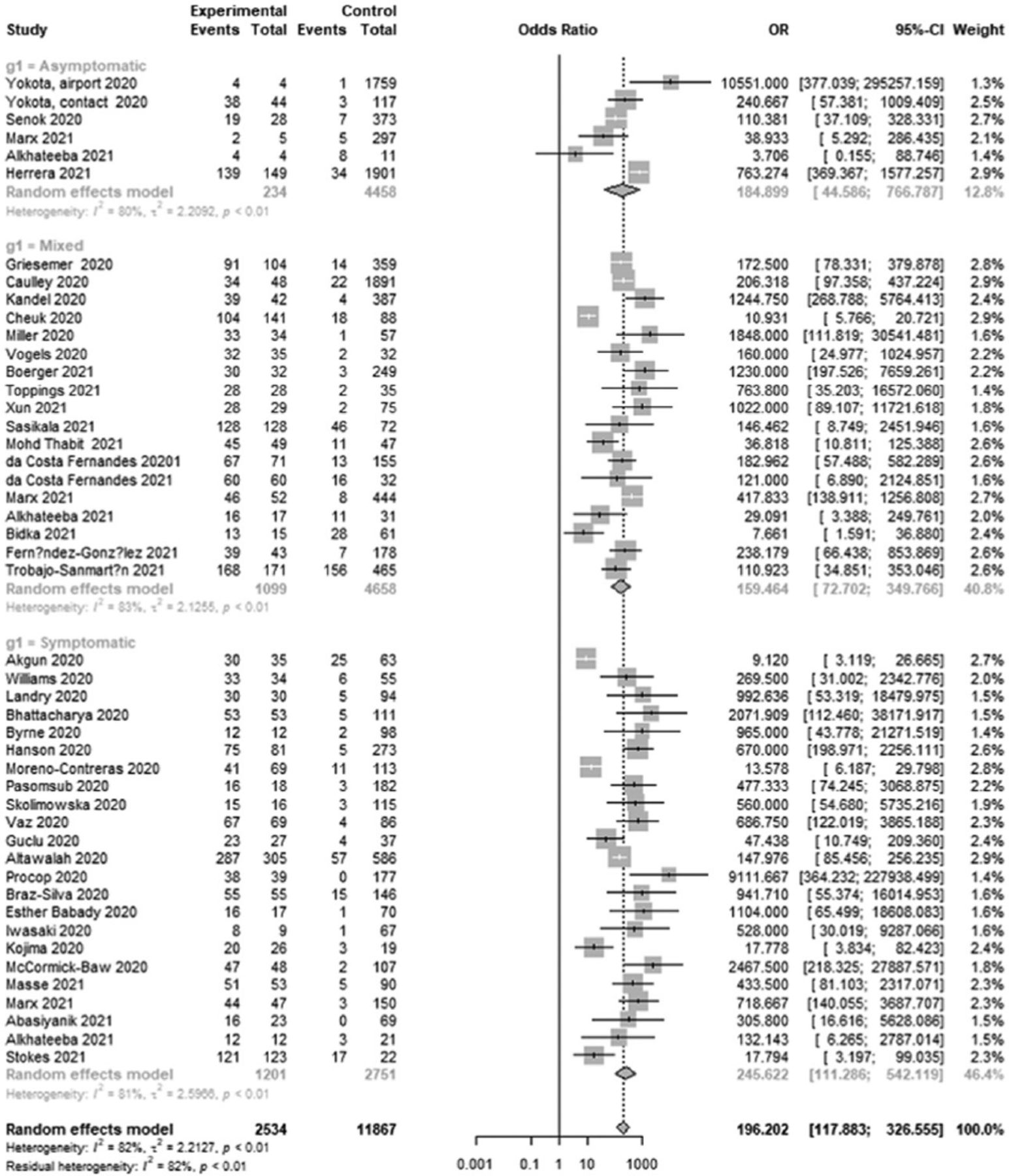
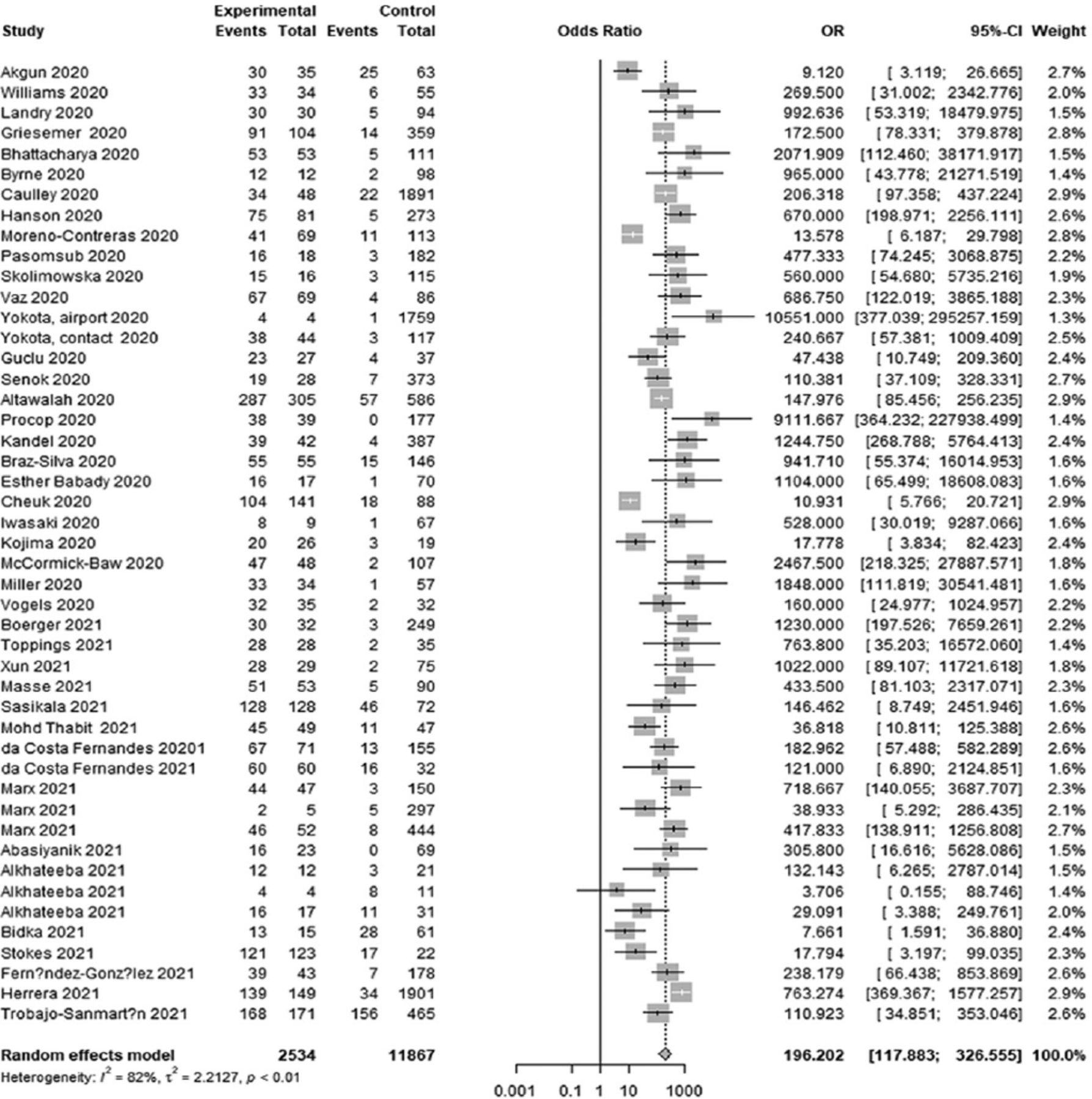
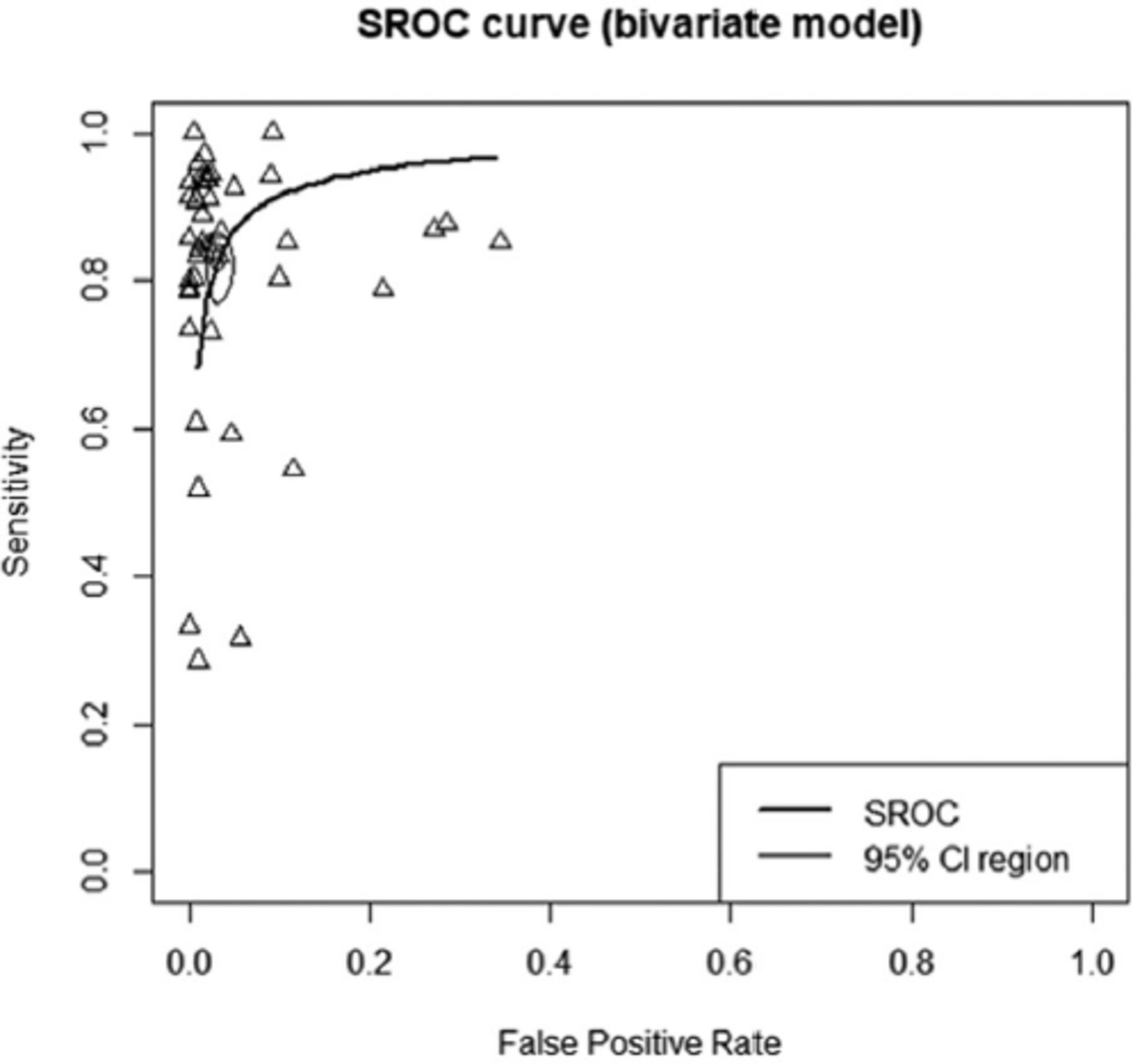
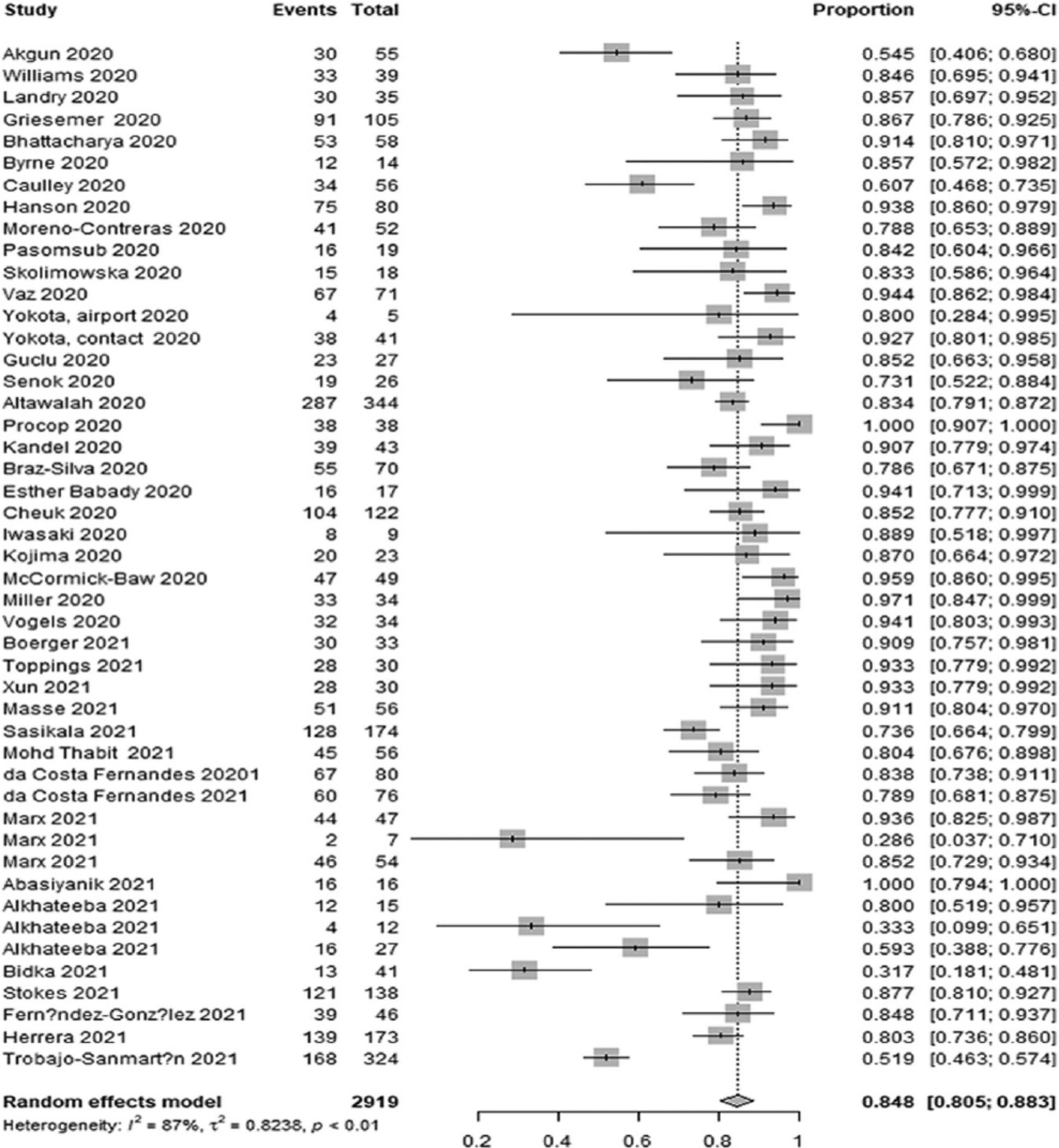
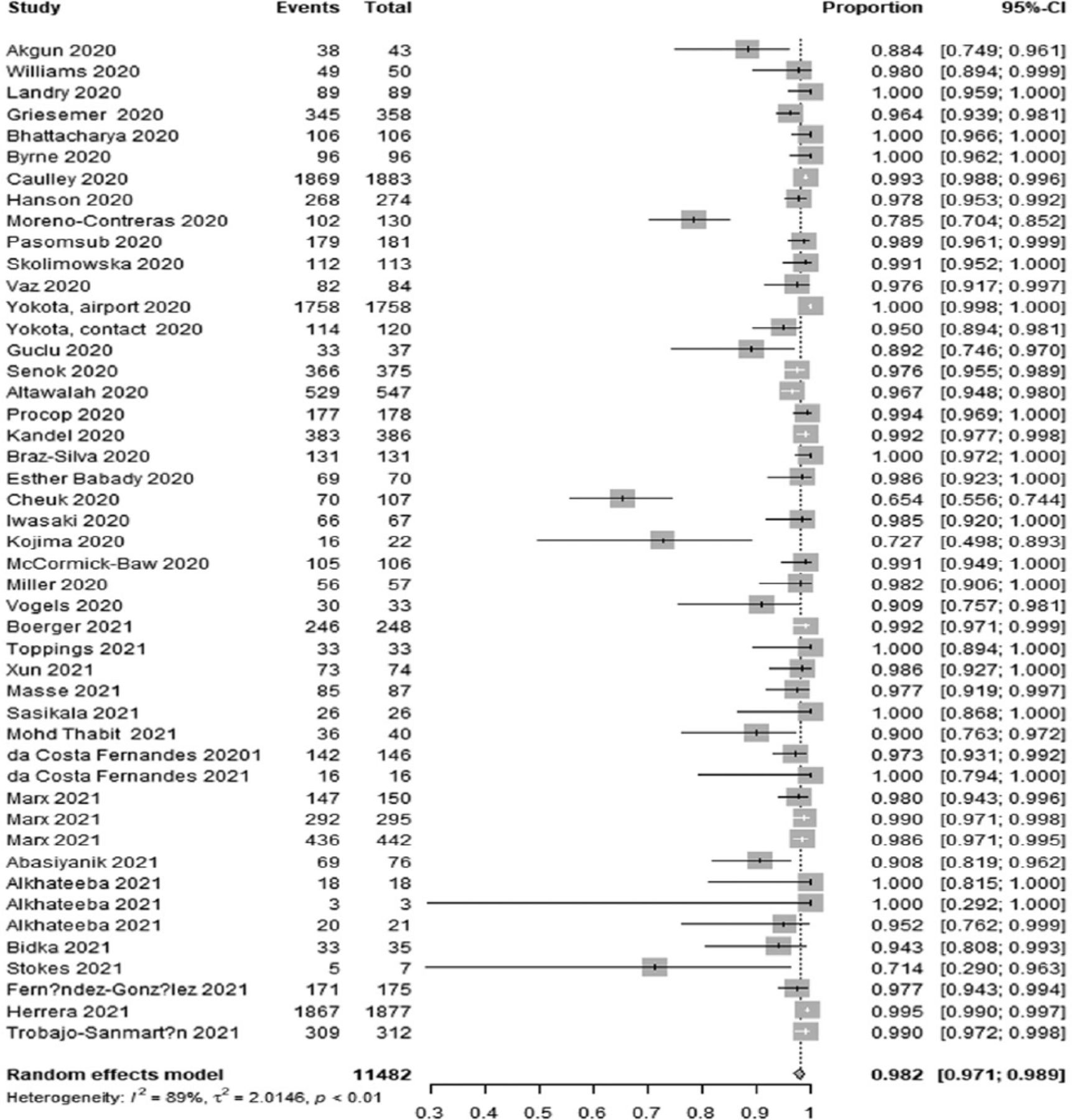
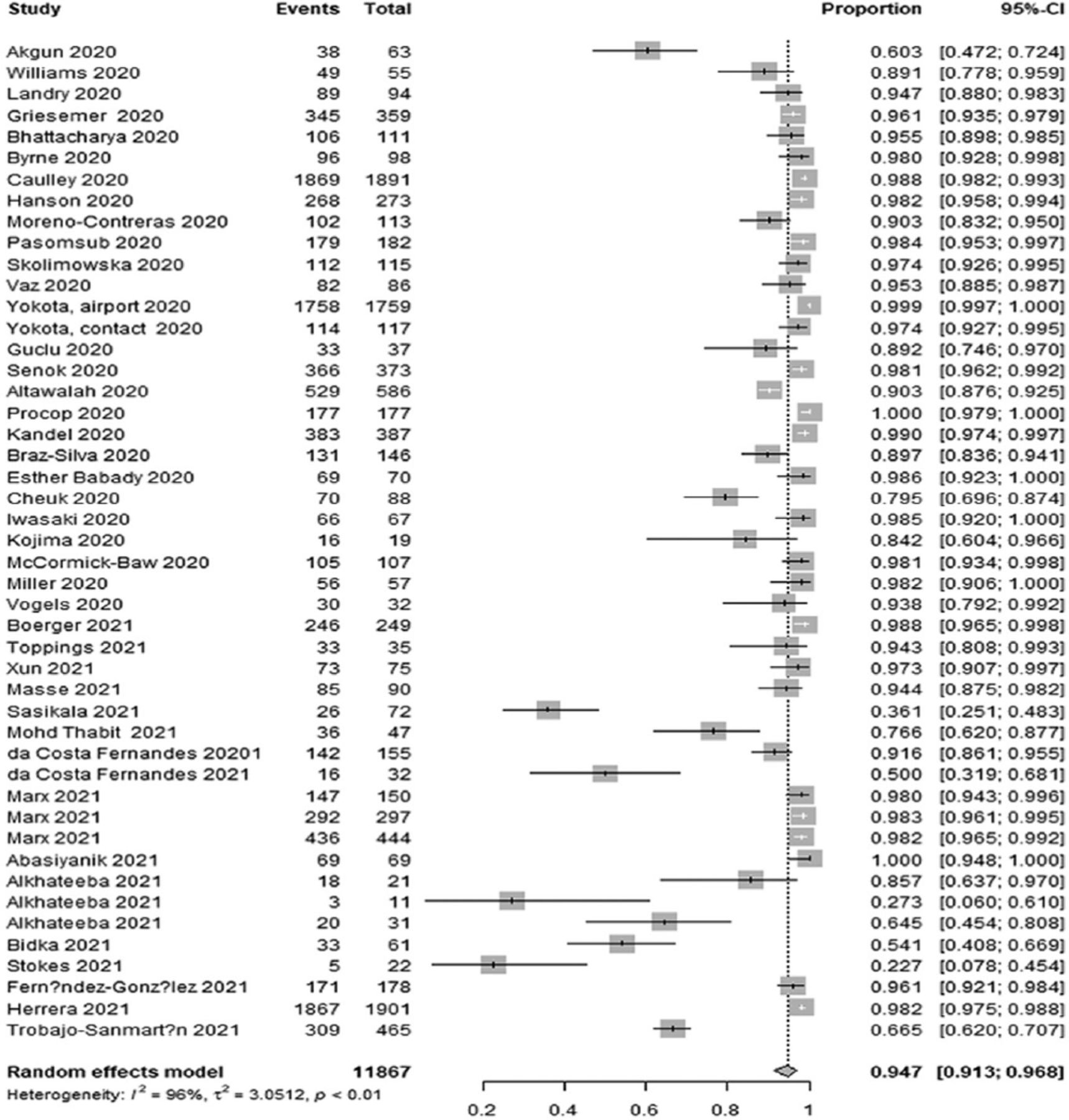
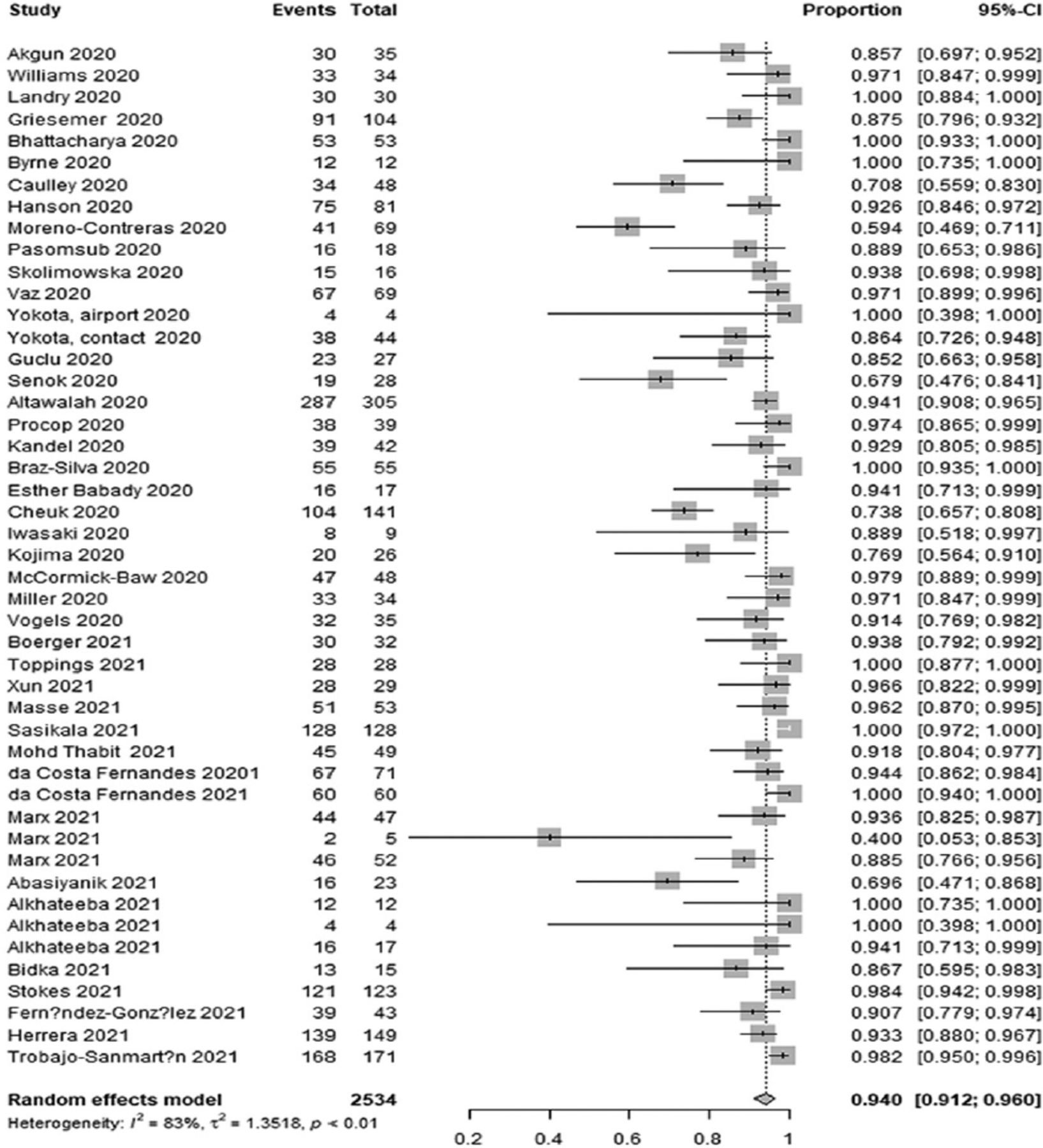
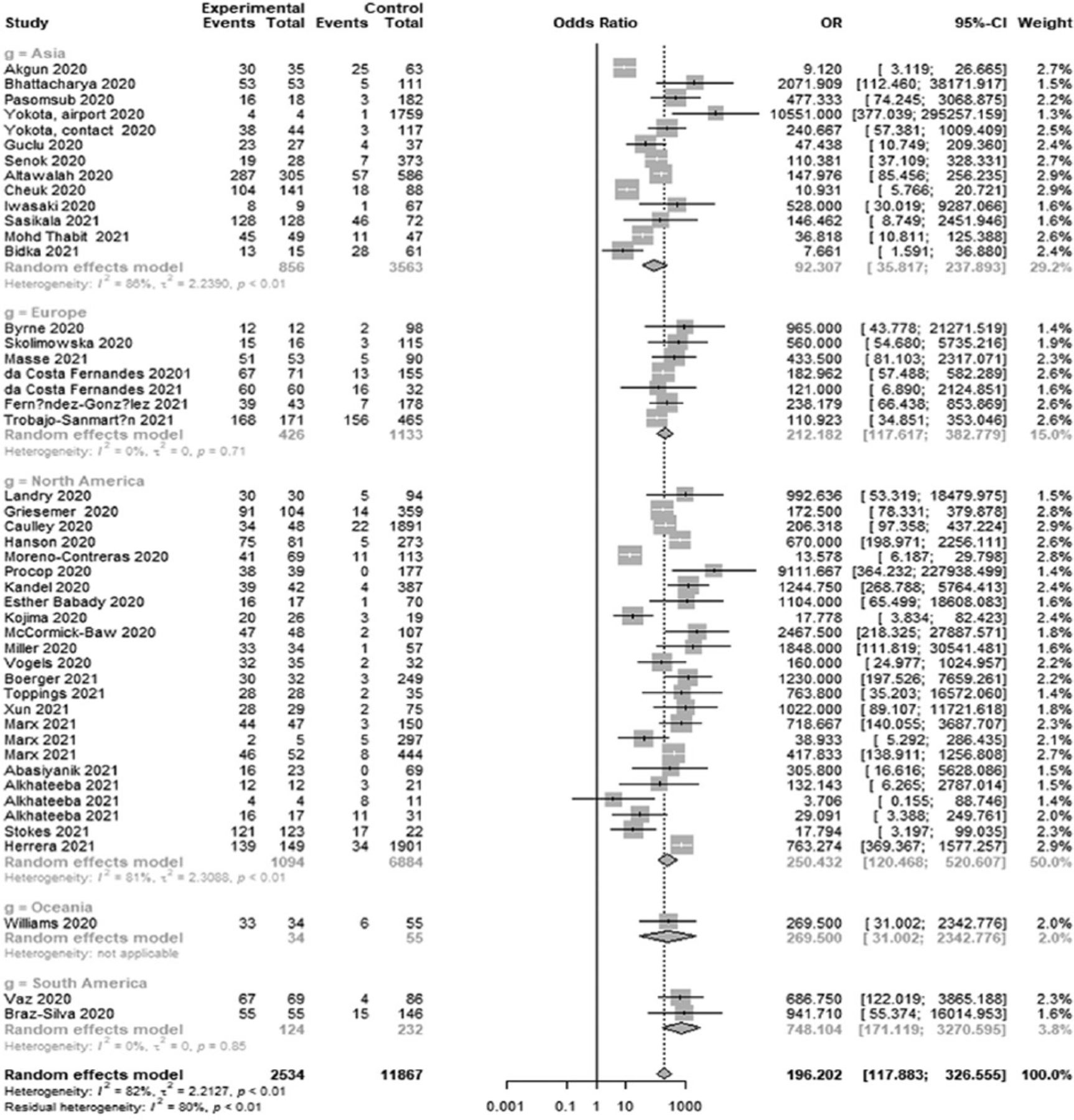
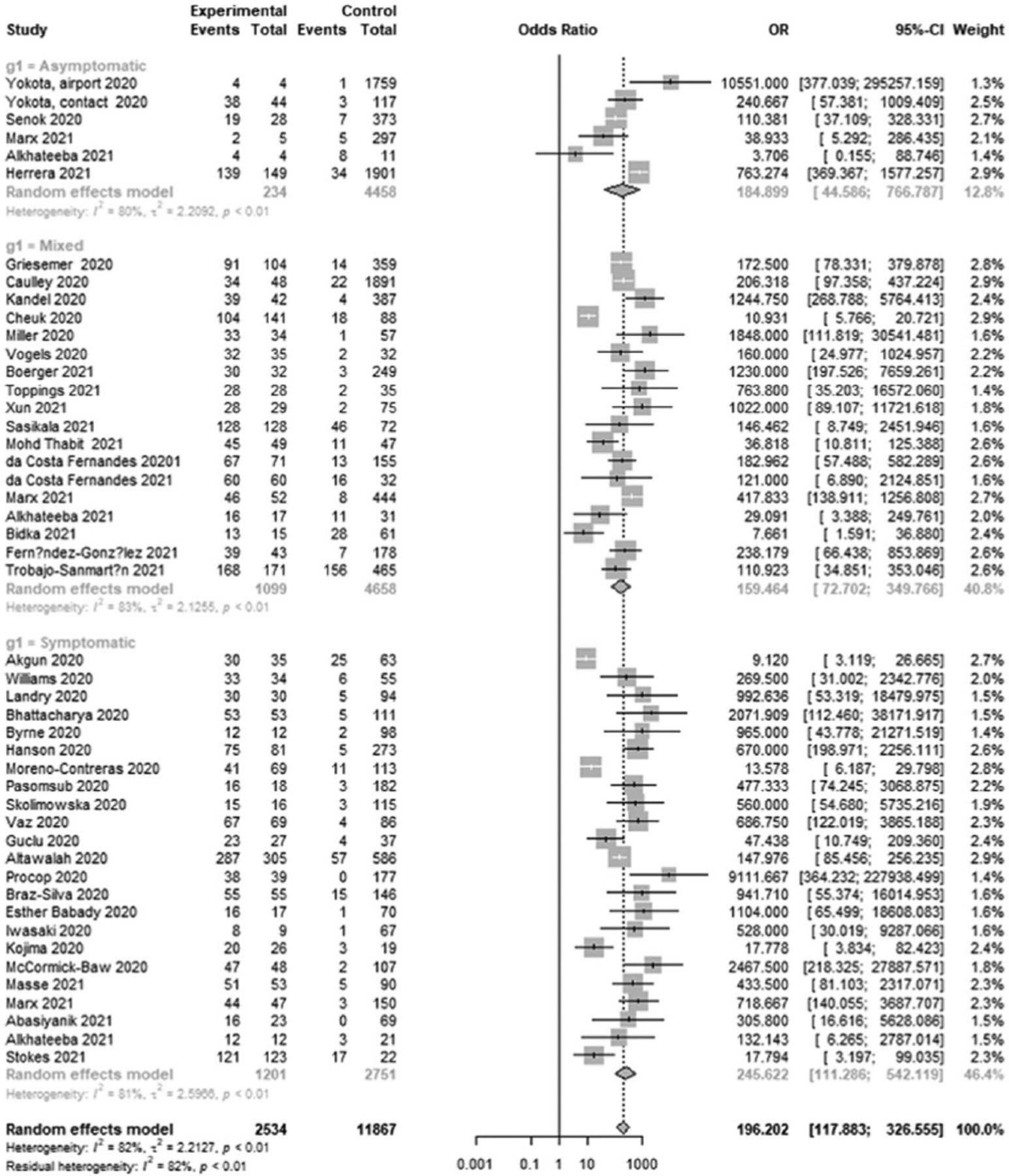
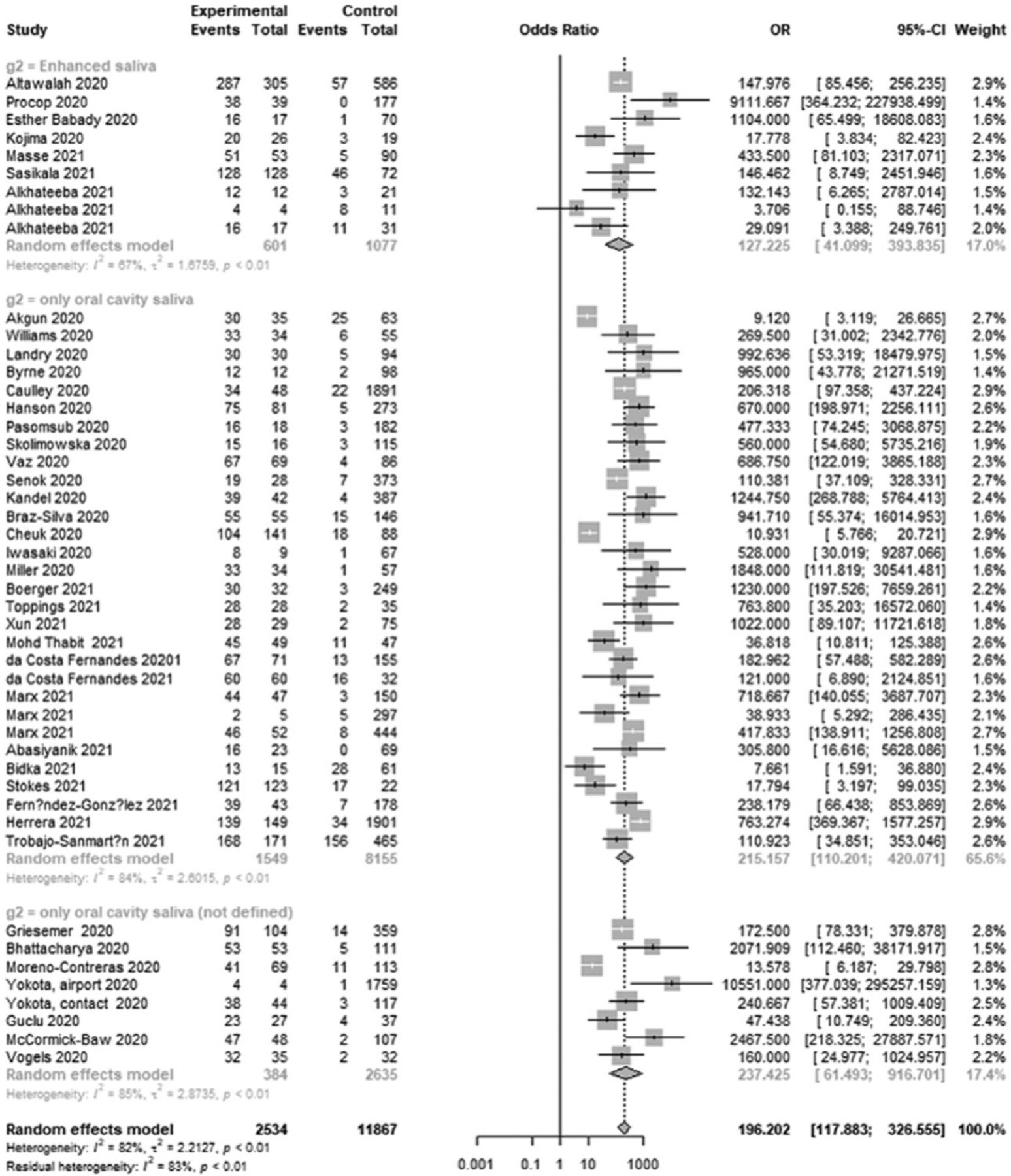
A total of 41 observational studies that used self-collected saliva samples for COVID-19 diagnosis were included in this study. The DOR of self-collected saliva for COVID-19 was 196.2022 (95% CI: [117.8833-326.5546], I2=82%; Figure 2) and the AUC was 0.955 (Figure 3). The self-collected saliva samples had a moderate sensitivity of 0.8476 (95% CI: [0.8045-0.8826], I2=87.3%) and PPV of 0.9404 (95% CI: [0.9122-0.9599], I2=83.2%) but a high specificity of 0.9817 (95% CI: [0.9707-0.9887], I2=89%) and NPV of 0.9467 (95% CI: [0.9130-0.9678], I2=96.4%; Appendix 4-7).

- Forest plot of the diagnostic odds ratios of the included studies.

- Area under the summary receiver operating characteristic (SROC) curve of the included studies. CI: confidence interval
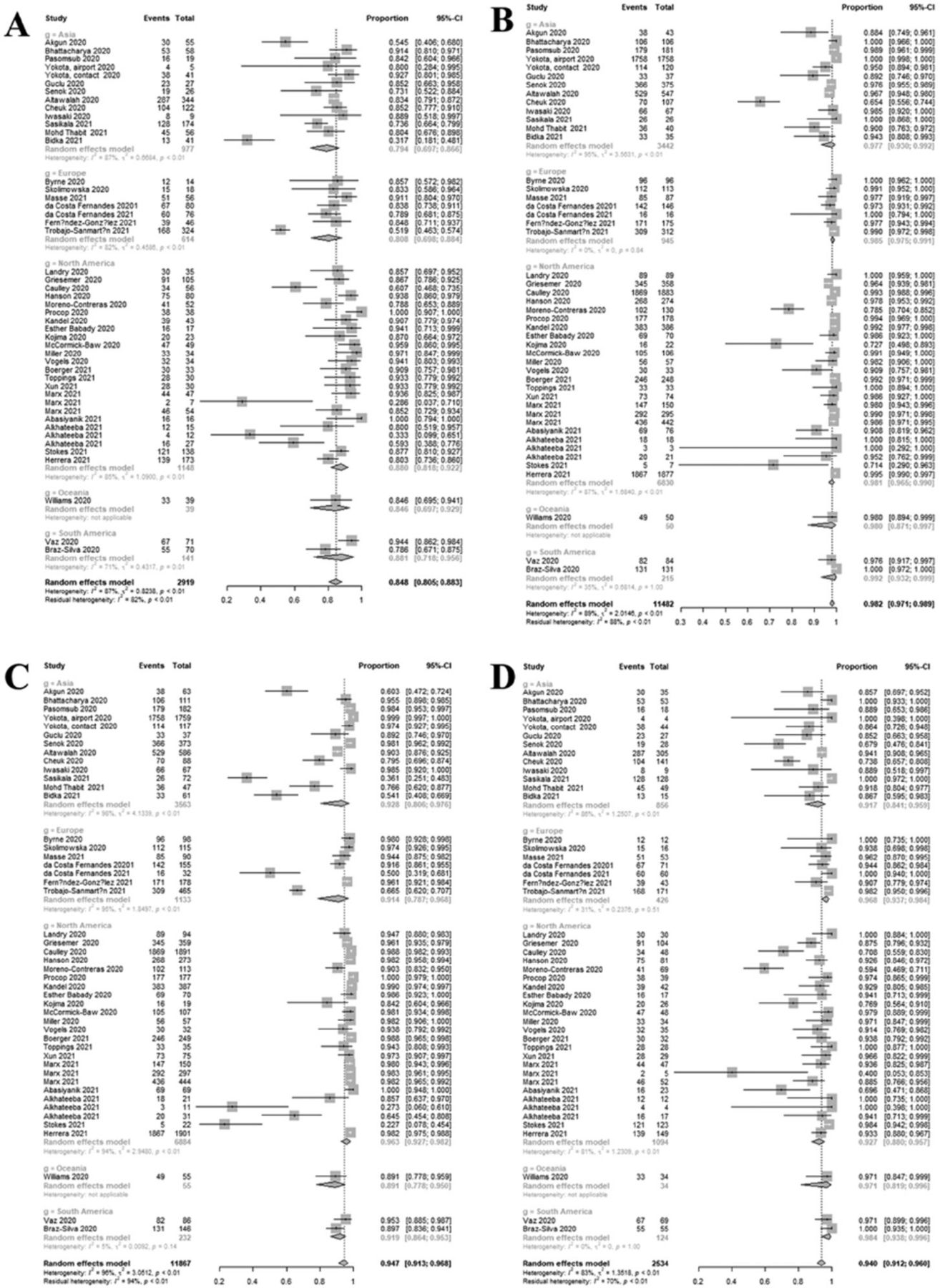
In concern of the heterogeneity of diagnostic accuracy, we looked for significant bias among the included studies. Subgroups were analyzed to assess the influence of geographic differences, saliva collection method, and presence or absence of symptoms (Table 1). Through these analyses, it was confirmed that there was no significant difference between continents.
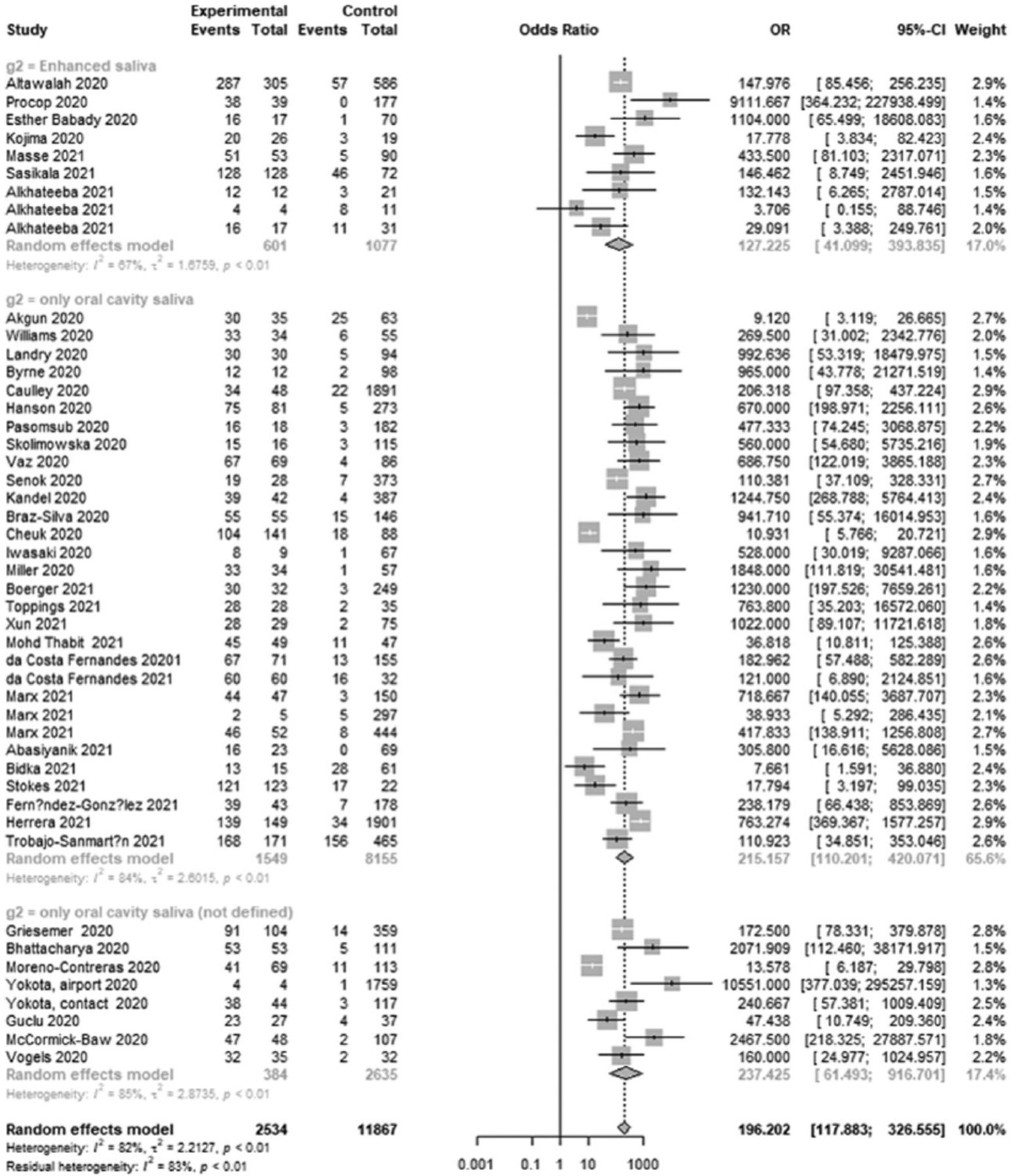
- Subgroup analysis of ethnicity, saliva collection method, and participants’ symptoms.
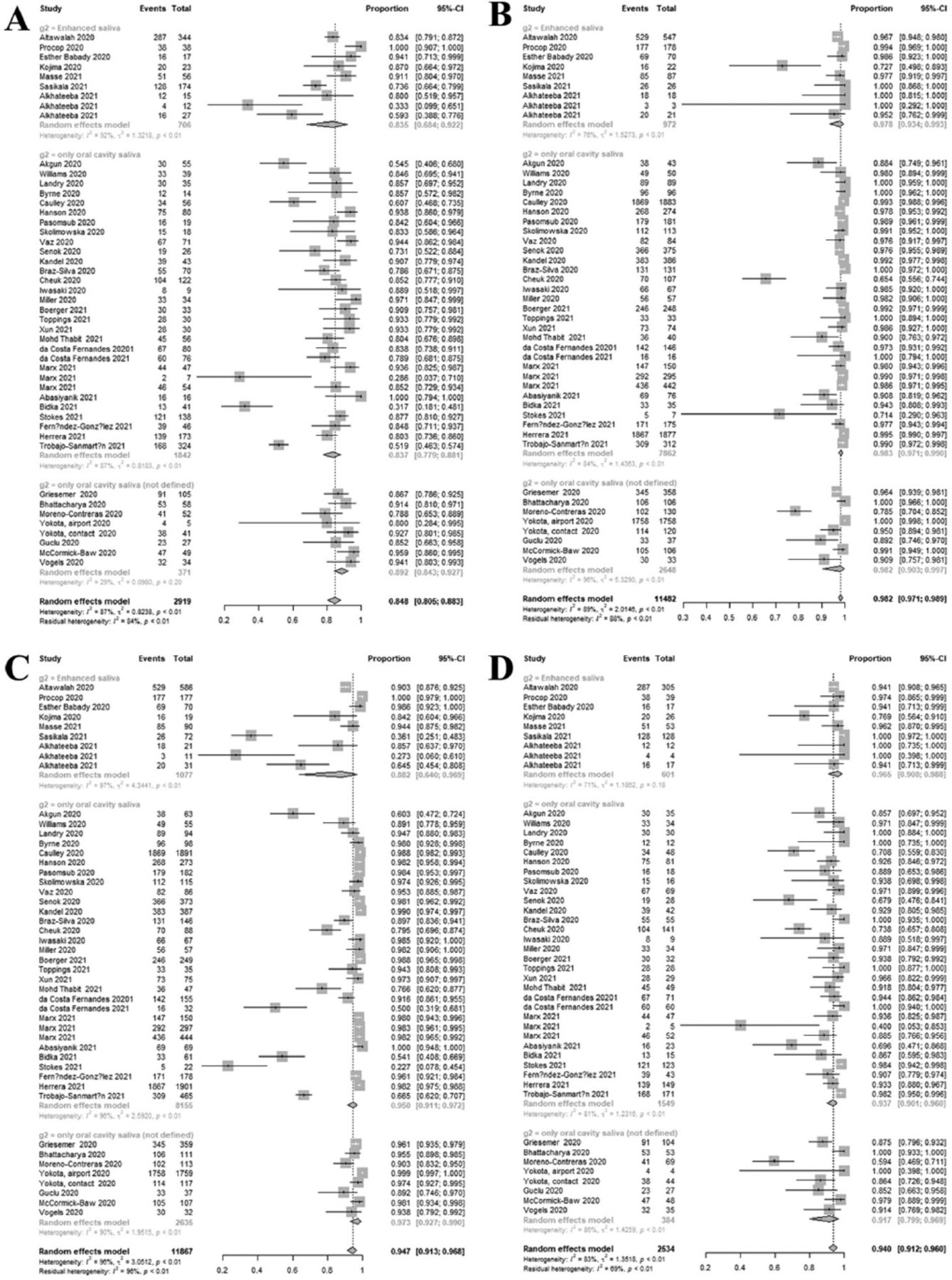
For the saliva collection method, there were 3 subgroups: enhanced saliva (including posterior pharyngeal saliva or induced cough), oral saliva only without cough, and oral saliva only not defined regarding cough. Diagnostic accuracy tended to be lower in the enhanced saliva than the other 2 subgroups (sensitivity: 0.8353 vs. 0.8365 and 0.8919, specificity: 0.9779 vs. 0.9827 and 0.9820, and NPV: 0.8823 vs. 0.9496 and 0.9731; Appendix 8-10, DOR: 127.2254 vs. 215.1566 and 237.4246 except PPV: 0.9654 vs. 0.9202 and 0.8510; Appendix 11-13). Regarding the presence/absence of symptoms in patients during testing, diagnostic accuracy tended to be higher in the symptomatic than non-symptomatic patients (sensitivity: 0.8851 vs. 0.8208 and 0.7049, specificity: 0.9791 vs. 0.9783 and 0.9933, NPV: 0.9522 vs. 0.9164 and 0.9772, PPV: 0.9495 vs. 0.9435 and 0.8483, DOR: 245.6222 vs. 159.4638 and 184.8991). All analyses performed on each subgroup showed high heterogeneity. Based on this, it is difficult to document that subgroup analysis explains heterogeneity.
A total of 16 studies reported the Cohen’s kappa coefficient; the summary intra-class correlation coefficient was 0.8506 (95% CI: [0.8024-0.8877]), and the heterogeneity was high (I2=97.05%). Therefore, the correlation coefficients represented a good qualitative agreement between the standard naso/oropharyngeal swab and saliva samples in this meta-analysis.
Discussion
Because of the rapid global spread of COVID-19 and its high morbidity and mortality rates at older ages, early and accurate diagnosis of COVID-19 is the key to disease management.3 In particular, the fall-winter season in the northern hemisphere which typically increases the co-circulation of other respiratory viruses, including influenza, which could render the difficulty of distinguishing COVID-19 from other respiratory diseases. Currently, naso/oropharyngeal swab sampling according to RNA extraction and RT-qPCR is the most common methods for SARS-CoV-2 detection. However, the naso/oropharyngeal swab procedure has several short-comings including nasal irritation, pain, and a requirement for technical skill (false-negative results may result from improper procedures). Furthermore, this procedure requires additional medical resources, such as personal protective equipment and sterile swabs.51 Considering these factors, the naso/oropharyngeal swab method is quite limited for mass screening or its use in developing countries.25 Therefore, there is an increasing need of an effective testing method for COVID-19 that is non-invasive, safe, comfortable, and requires minimal medical resources.52
Saliva samples have previously been proposed as diagnostic tools for detecting various respiratory virus infections, such as influenza viruses, respiratory cell fusion viruses, and SARS-CoV. Recent studies have shown that SARS-CoV-2 could also be diagnosed with saliva.25 In addition, saliva sampling reduces time and costs by eliminating the need for personal protection or virus-carrying solutions.16 Therefore, studies have been conducted to examine the diagnostic power of tests based on saliva sampling.7,8,10-26
Two previous meta-analyses evaluated the use of saliva to accurately diagnose COVID-19.9,53 The authors suggested that self-collected saliva can be used to diagnose COVID-19. However, there were some limitations to confirm the evidence.9,53 Due to the relatively small sample size, a comprehensive analysis and thorough investigation were difficult in previous analysis.9 The other analysis evaluated 8 additional studies, but it had methodologic flaws.53 For example, only one author conducted the search and extracted data from the included studies, and there was no mention of the heterogeneity among the enrolled studies or the strategy for addressing the heterogeneity (for instance, subgroup analysis).53
Therefore, we did a bivariate meta-analysis with newly included studies focusing on the location and timing of sample harvest. The self-collected saliva samples were compared to samples collected by medical workers using naso/oropharyngeal swabs, and qualitative agreement between the saliva-based test and reference test was assessed. This information could be helpful for citizens to gain easy and early access to the test and for healthcare professionals to minimize the risk of SARS-CoV-2 transmission via specimen contact.
In this study, self-collected saliva testing yielded AUC of 0.955. The AUC was in the range of 0.9-1, suggesting excellent diagnostic accuracy.49 The virus utilizes the angiotensin converting enzyme 2 receptor for host entry, and it is also expressed at detectable levels in the salivary glands and ducts.54 In addition, salivary gland epithelial cells are early targets and the virus can dwell inside the cells during the first stage of infection.7,54 High correlation coefficients, indicating strong diagnostic agreement between the standard naso/oropharyngeal swab and the saliva collection sample, also could support the diagnostic power of the saliva samples.
However, our results showed that self-collected saliva samples had lower sensitivity and similar specificity compared with naso/oropharyngeal swab specimens for diagnosing COVID-19. This finding was consistent with the previous findings of Kivelä et al.53 Previous studies reported lower viral loads of SARS-CoV-2 in saliva than in corresponding nasopharyngeal swab specimens.7,15,54 The lower viral load in saliva may explain the higher rate of false negatives (decreasing sensitivity) compared with naso/oropharyngeal specimens.15,53 However, relatively low sensitivity of the saliva-based test is acceptable under certain conditions, considering that the saliva sampling test requires fewer medical consumable resources and professional personnel, and minimizes patient’s discomfort.53
In this regard, one report recommended standardizing the sampling and testing methods for optimal clinical application of the saliva-based COVID-19 test.9 Our meta-analysis included various methods (saliva only vs. enhanced saliva [including lower pharyngeal and respiratory secretion]) and clinical conditions (asymptomatic vs. symptomatic examinees). Therefore, we carriedout a subgroup analyses according to different geography, saliva collection method, and existence or absence of symptoms. Interestingly, the saliva collection method did not show the significant influence in diagnostic accuracy. A previous study also reported similar results that there was no substantial difference between only oral saliva and enhanced saliva.55 In pathophysiology and time course, the main entry points of coronavirus are the nasal epithelial cells as well as the stratified squamous epithelium of oropharynx and laryngopharynx.56 Through oral-lung aspiration, the virus can spread from oral or nasal passage to the lower respiratory organs. In 80% of infected cases, the virus remains within the upper airway expressing mild symptoms.57 The enhanced saliva may contain both bronchopulmonary and nasopharyngeal secretions by coughing. The current knowledge of viral progression from proximal to distal airways might explain why oral saliva plus lower respiratory secretion seemed to have the similar diagnostic accuracy with oral saliva only in the community or mass screening. In particular, some patients would feel uncomfortable or have difficulty in coughing to produce mucus. However, simple collecting method such as drooling or spitting could help spread the usage of saliva test for COVID-19.
In addition, the viral loads of samples were significantly high during the first week of symptom development, then gradually decreased over time, and became undetectable approximately 2 weeks after symptom development.58 These patterns could indicate that the timing of sampling regarding diagnosis was likely to influence accuracy in asymptomatic as well as symptomatic patients. Caution is recommended when choosing diagnostic tests for screening in terms of the related timing to disease progression.58 Saliva self-collection for SARS-CoV-2 testing was reported not to be influenced by gender, age, race/ethnicity, or educational level in the United States.19 There was no significant heterogeneity of diagnostic accuracy among geographic locations. However, our classification according to geographic location included only one or 2 studies in South America and Oceania. Therefore, future prospective studies with larger numbers of patients evenly grouped by geographic location are needed to analyze the effect of geographic location on the results of test using self-collected saliva.
Study limitations
First, the collected data showed significant heterogeneity that required random effect models and subgroup analysis. One possible explanation is that RT-qPCR in naso/oropharyngeal samples, which is used as the main diagnostic tool for COVID-19, shows a wide range in sensitivity (56-83%).59 This might have led to misclassification and diagnostic bias, causing heterogeneity. Secondly, the nature of cross- sectional designs can over- or under-estimate the real prevalence. Thirdly, there was a lack of methodological homogeneity and inadequate reporting of methods.9
In conclusion, this study indicated that RT-qPCR detects SARS-CoV-2 with lower sensitivity using self-collected saliva compared to conventional naso/oropharyngeal samples. However, saliva samples are easily obtained by drooling or spitting in a sample container. The saliva-based test has the advantage of not requiring healthcare workers or personal protective equipment for sample collection. This advantage could be useful in situations in which mass screening is needed or medical resources are scarce.
Acknowledgment
The authors gratefully acknowledge Textcheck (www.textcheck.com) for English language editing.
Appendix 1 - Participants, interventions, comparisons, outcomes, timings, and study design (PICOTS)
Appendix 2 - Study characteristics
Appendix 3 - Methodological quality of all included studies
Appendix 4 - Forest plots of the sensitivity of the included studies
Appendix 5 - Forest plots of the specificity of the included studies
Appendix 6 - Forest plots of the negative predictive value of the included studies
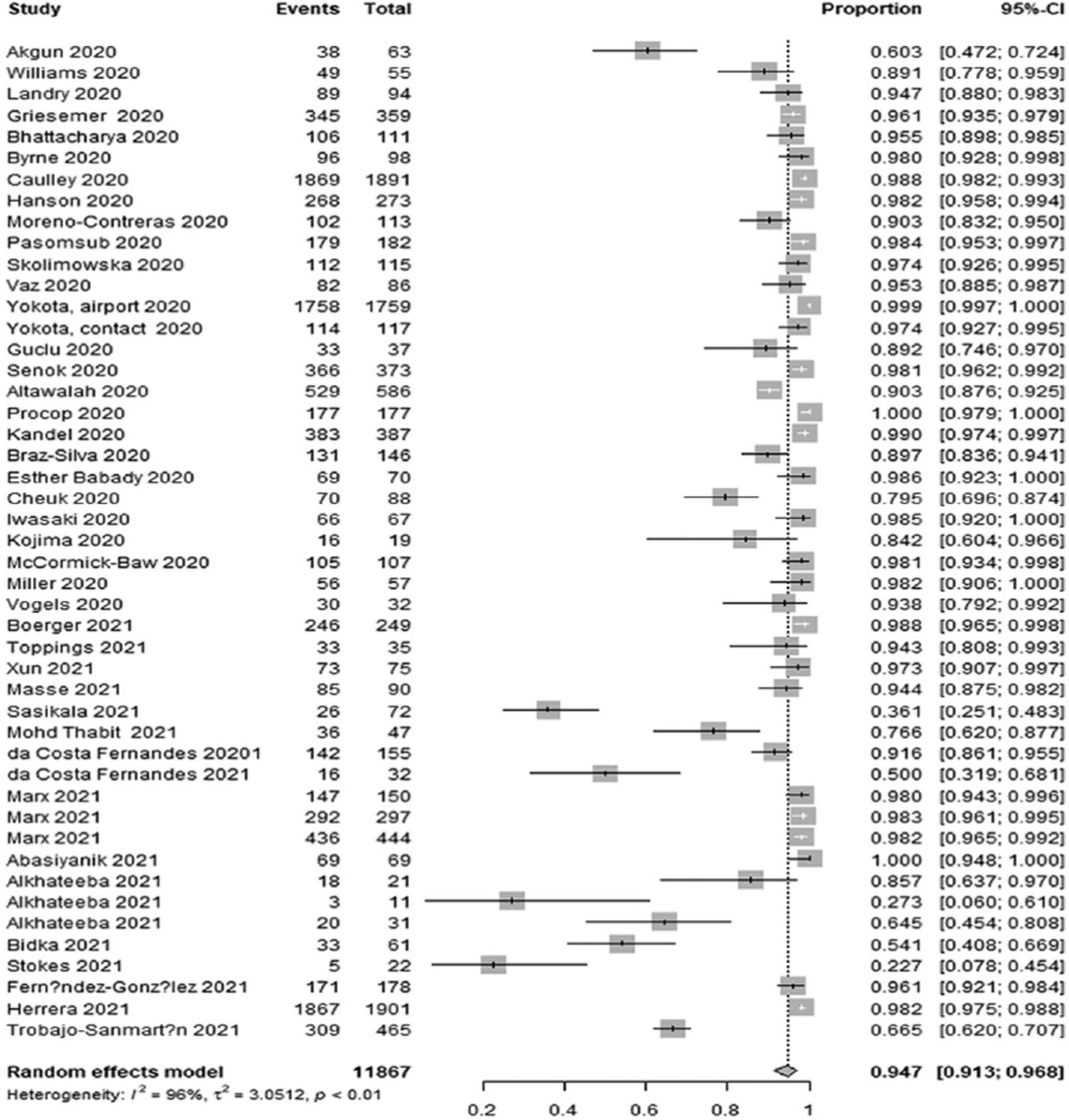
Appendix 7 - Forest plots of the positive predictive value of the included studies

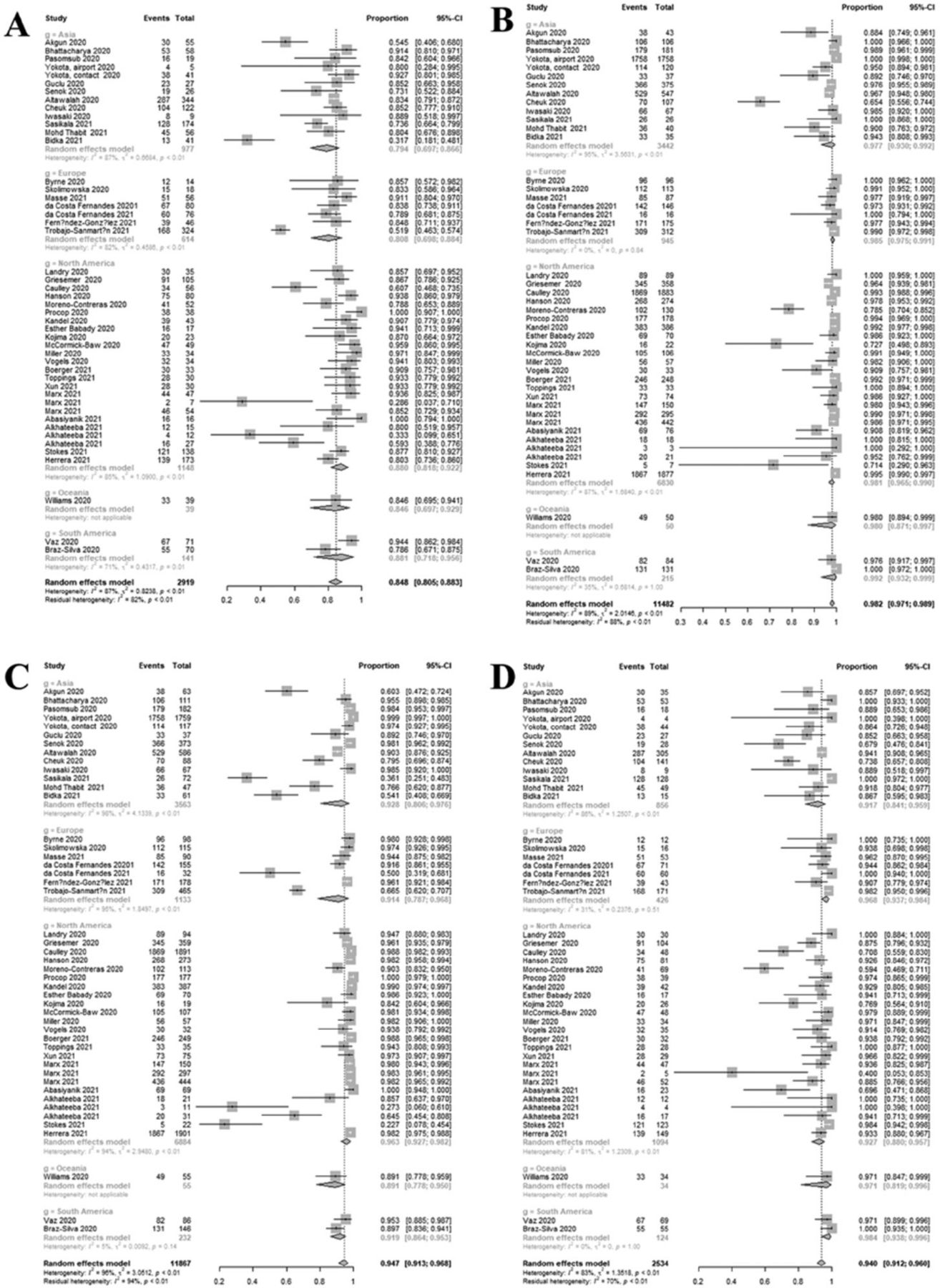
Appendix 8 - Forest plots of A) the sensitivity, B) the specificity, C) the negative predictive value, and D) the positive predictive value regarding the effect of geographic differences on self-collected saliva for COVID-19
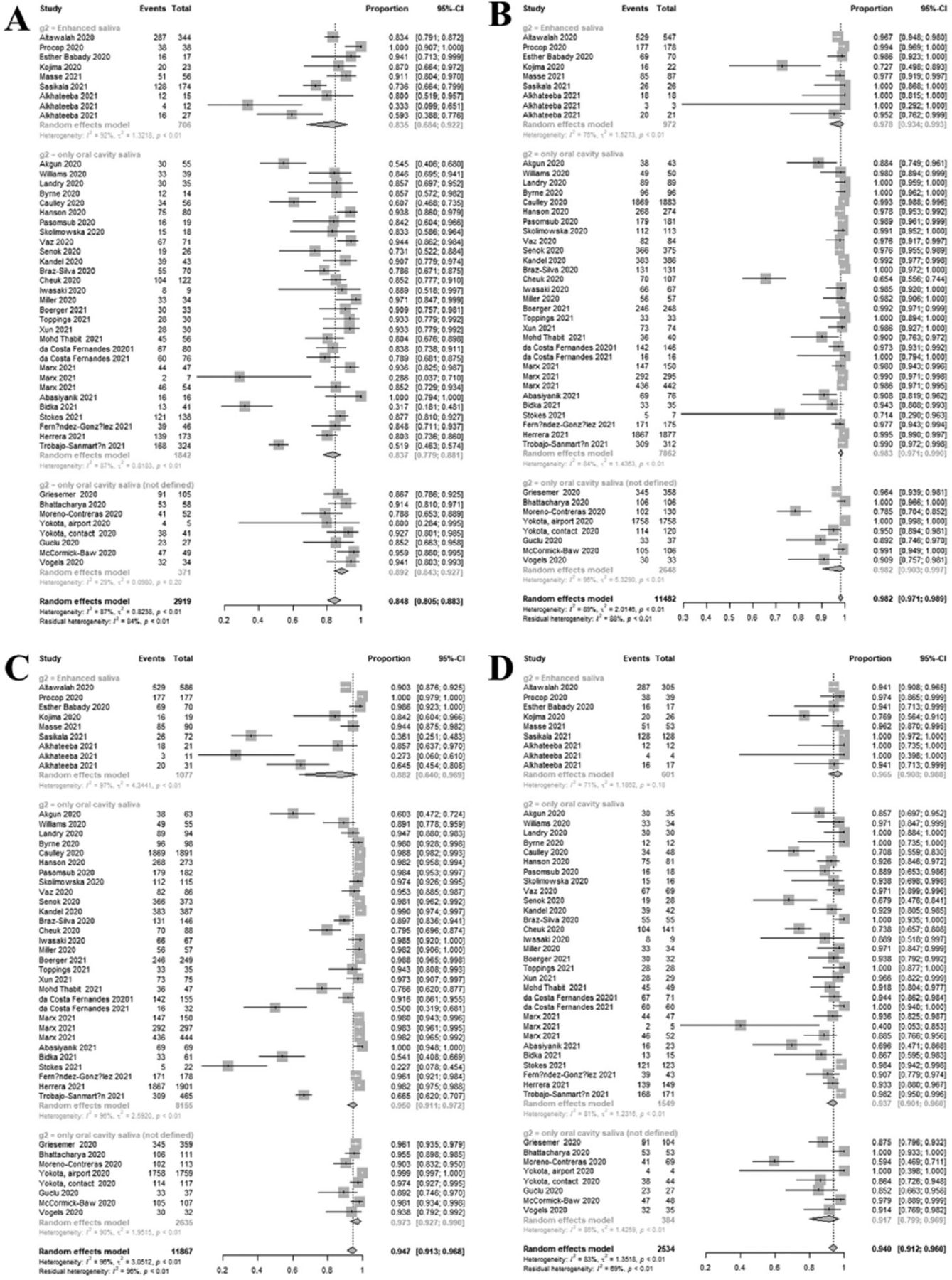
Appendix 9 - Forest plots of A) the sensitivity, B) the specificity, C) the negative predictive value, and D) the positive predictive value regarding the effect of saliva collection method on self-collected saliva for COVID-19
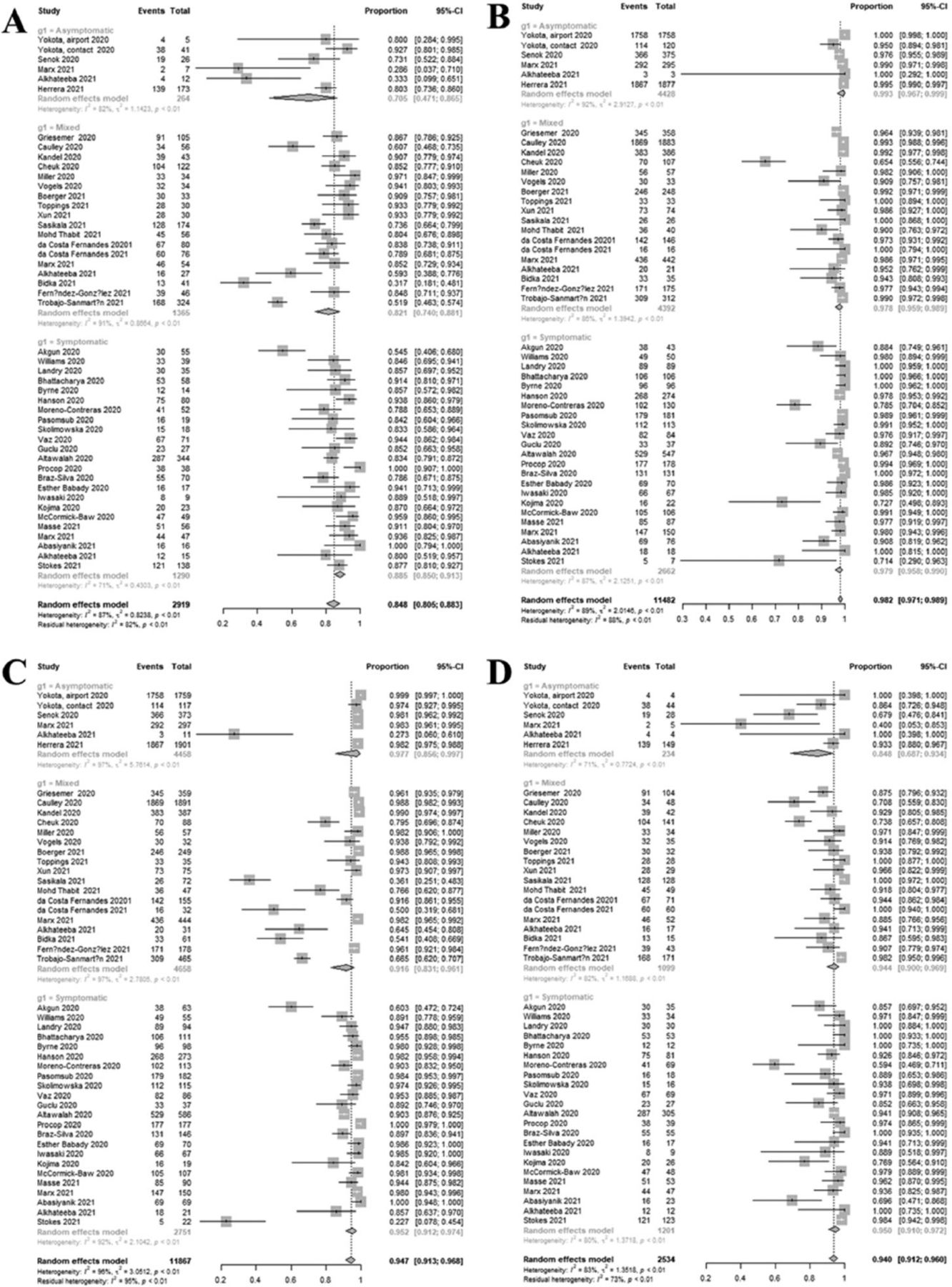
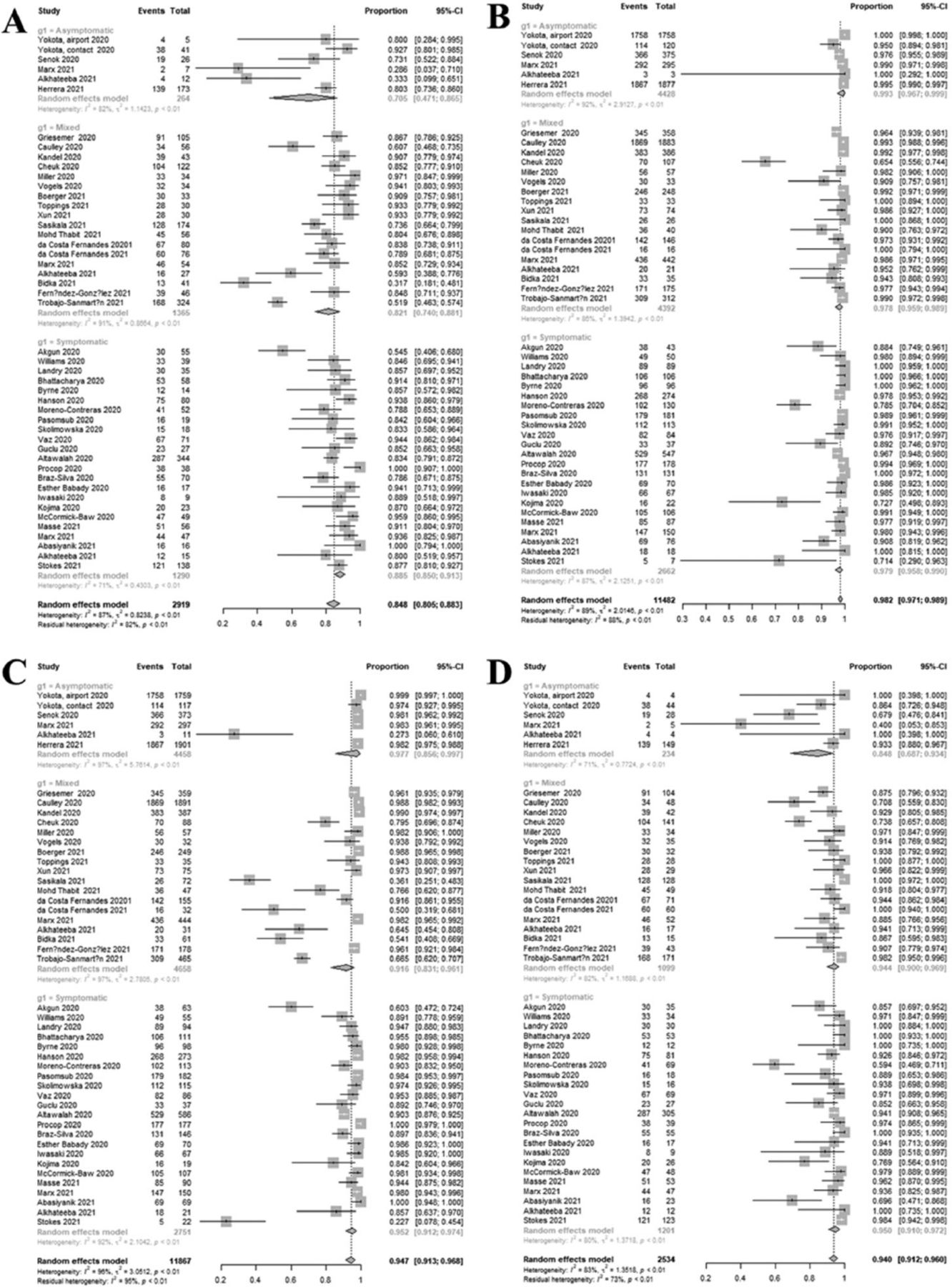
Appendix 10 - Forest plots of A) the sensitivity, B) the specificity, C) the negative predictive value, and D) the positive predictive value regarding the effect of presence or absence of symptoms on the diagnostic odds ratios on self-collected saliva for COVID-19
Appendix 11 - The effect of geographic differences on the diagnostic odds ratios of self-collected saliva for COVID-19

Appendix 12 - The effect of saliva collection method on the diagnostic odds ratios of self-collected saliva for COVID-19
Appendix 13 - The effect of presence or absence of symptoms on the diagnostic odds ratios of self-collected saliva for COVID-19
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 21, 2021.
- Accepted December 7, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Methods
- Results
- Discussion
- Acknowledgment
- Appendix 1 - Participants, interventions, comparisons, outcomes, timings, and study design (PICOTS)
- Appendix 2 - Study characteristics
- Appendix 3 - Methodological quality of all included studies
- Appendix 4 - Forest plots of the sensitivity of the included studies
- Appendix 5 - Forest plots of the specificity of the included studies
- Appendix 6 - Forest plots of the negative predictive value of the included studies
- Appendix 7 - Forest plots of the positive predictive value of the included studies
- Appendix 8 - Forest plots of A) the sensitivity, B) the specificity, C) the negative predictive value, and D) the positive predictive value regarding the effect of geographic differences on self-collected saliva for COVID-19
- Appendix 9 - Forest plots of A) the sensitivity, B) the specificity, C) the negative predictive value, and D) the positive predictive value regarding the effect of saliva collection method on self-collected saliva for COVID-19
- Appendix 10 - Forest plots of A) the sensitivity, B) the specificity, C) the negative predictive value, and D) the positive predictive value regarding the effect of presence or absence of symptoms on the diagnostic odds ratios on self-collected saliva for COVID-19
- Appendix 11 - The effect of geographic differences on the diagnostic odds ratios of self-collected saliva for COVID-19
- Appendix 12 - The effect of saliva collection method on the diagnostic odds ratios of self-collected saliva for COVID-19
- Appendix 13 - The effect of presence or absence of symptoms on the diagnostic odds ratios of self-collected saliva for COVID-19
- Footnotes
- References
- Figures & Data
- eLetters
- References
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.