


Abstract
Objectives: To reducing the risk of venous thromboembolic (VTE) events and subsequent mortality in covid-19 patients is still a matter of research. This systematic review and meta-analysis serve the purpose of comparing the mortality associated with the intensity of anticoagulation in patients admitted with covid-19.
Methods: A total of 7120 patients were recruited in 11 studies comparing using prophylactic anticoagulants against therapeutic anticoagulants.
Results: Our study showed that using prophylactic anticoagulants was associated with a 42% reduction in mortality compared to therapeutic anticoagulants (OR 0.58 (95% CI:0.676-0.499), p=0.000). Also, we assessed mortality in patients using no anticoagulants against using prophylactic anticoagulants. A total of 6069 patients were recruited in 4 studies in which 2 studies significantly favored prophylactic anticoagulants in terms of reducing mortality. Cumulatively, the meta-analysis showed that using prophylactic anticoagulants was associated with a 5% reduction in mortality but without any statistical significance: (OR 1.049 [95% CI 1.237 - 0.865]) (p=0.626).
Conclusion: Our meta-analysis favors using prophylactic anticoagulation in covid-19 patients reduces all-cause mortality in comparison to therapeutic anticoagulation however the impact on mortality when compared with no anticoagulation was not significant.
PROSPERO Number: CRD42021257320
The Coronavirus disease 2019 (COVID-19) is a global pandemic resulting in significant mortality and morbidity burden worldwide. According to the World Health Organization (WHO), as of September 2021, millions of cases were reported, with more than 4 million deaths.1 Since its recognition in late 2019, understanding of COVID-19 has evolved considerably, improving preventative and management measures.
Research has been focused on various treatment modalities in COVID-19 pneumonia and their effectiveness. There has been considerable success in identifying multiple potential therapeutic agents and synthesizing effective vaccinations.
COVID-19 is known to be a prothrombotic state.2 One aspect of interest for research is to mitigate the risk associated with the higher incidence of venous thromboembolic (VTE) events, especially pulmonary embolism (PE).3 Although the pathophysiology is not studied in-depth, stimulation of proinflammatory cytokines, cell-death mechanisms, and vascular endothelial damage are known driving factors of coagulation dysfunction cascade.4 Patients admitted with COVID-19 also exhibit elevated levels of D-dimers that may suggest ongoing hyperfibrinolysis.4 These pathophysiological changes likely contribute towards increased VTE events in COVID-19 patients. Therefore, approaches to lower the risk of VTE events are still a matter of academic interest and research.5
Evidence regarding appropriate anticoagulation strategies to prevent VTE events and subsequent adverse outcomes in COVID-19 remains unclear. Some studies showed increased mortality in patients receiving pre-emptive therapeutic anticoagulation, while others showed positive outcomes. 3,6-8 This necessitates further research and data to identify the safest approach to minimize the fatal adverse outcomes of VTE in COVID-19.
Thus, this systematic review and meta-analysis explores the mortality beneficial roles of anticoagulation use in COVID-19 patients. It compares all-cause mortality in patients who received prophylactic doses of anticoagulants compared to those treated with therapeutic doses. This comparison is made possible by the increasing number of available studies that addressed anticoagulation since the pandemic.
Methods
We used Preferred Reporting Items for Systematic Reviews and Meta-Analysis to complete this meta-analysis and systemic review. A predefined protocol was registered with Prospero before the initiation of our study.
In our study, we included all randomized controlled trials (RCTs), cluster trials or controlled (non-randomized) clinical trials (CCTs), retrospective and prospective comparative cohort studies, and case-control or nested case-control studies. Cross-sectional studies, case reports, and case series were excluded from the study sample.
A search strategy was constructed using medical subject headings (MeSH). The MeSH terms of COVID-19, SARS-CoV-2, and anticoagulation were used to systemically search PubMed, Cochrane Central Register of Controlled Trials (Wiley interface, current issue), Embase, and MEDLINE databases. Only studies in the English language and with a study population of 18 years and above were included. All the relevant publications up to August 27, 2021, were included.
Both quantitative and qualitative studies were included. No limits regarding study design or date were set on the search, and all studies in English language were included. The MEDLINE strategy was developed with input from the project team. After the MEDLINE strategy was finalized, it was adapted to the syntax and subject headings of the other databases. The search was properly reviewed and validated to make certain that the MEDLINE strategy retrieves a high proportion of eligible studies found through any means but indexed in MEDLINE.
Lastly, duplicate studies were removed from our study pool. All the included studies were scrutinized against strict inclusion and exclusion criteria, as provided in Table 1. Our inclusion criteria primarily focused on published literature that assessed the effect of anticoagulation dosage on COVID-19 mortality outcomes in hospitalized patients.
- Study inclusion and exclusion criteria.
The remaining titles and abstracts found against the above inclusion criteria were properly screened by the team of authors. The whole text of these research articles was downloaded and reviewed extensively by the authors. Following this process, the authors included the articles that fulfilled the inclusion criteria in the final sample. After all the authors’ agreements, the current list of studies was finalized. Any discrepancy was resolved through discussion and consensus among the authors (Table 2).
- The main characteristics of the included studies.
- The main characteristics of the included studies (continuation).
To obtain data from the shortlisted studies, a standardized form was used. These forms were reviewed independently in duplicate by the reviewers to ensure standardization. The extracted data included the type and setting of the study, sample size and distribution, anticoagulation intervention, and its outcomes in terms of all-cause mortality. The data was then analyzed by Comprehensive Meta-analysis Software (CMA) version 3 software and forest plots and funnel plots were made using the same software.
Statistical analysis
Comprehensive meta-analysis version 3 software was used to perform statistical analysis. In order to run the analysis data was entered in the format of comparison of 2 groups, then analysis was executed for dichotomous data and using data for retrospective studies.
The data was entered as the number of events in each group and the groups were named according to the dose of anticoagulant used namely prophylactic therapeutic and no anticoagulation. In the first set of data extraction data was extracted for mortality of prophylactic versus therapeutic anticoagulation and in the second group data for mortality of prophylactic versus no anticoagulation was obtained. The exact calculation used are odds ratio (OR) log along with their respective standard errors for group 1 and p-values in group 2 for each study as shown in tables.
This meta-analysis was completed using random effect model. Risk of bias was evaluated for each study individually. Sensitivity analysis was carried out by exclusion of studies with high risk of bias, and then re doing the meta-analysis after exclusion of each study with high risk of bias.
The methods used to assess variability and heterogeneity were the calculation of Q values, degrees of freedom (df) values, Q-df values, T and I² statistics. The exact values of the above parameters for both groups was as the following: i) For group one comparing prophylactic anticoagulation vers therapeutic anticoagulation Q value is 180.745 versus (vs.) df (Q) is 8 and the I-squared is 95.574. ii) For group 2 comparing no anticoagulation to prophylactic anticoagulation Q value is 40.931 the df (Q) is 3 and I-squared is 92.671.
The variables for which data was extracted included total number of patients in a study, the location of the study, the mean age of the patients, gender groups of the patients, type of anticoagulation used, and mortality in the 2 groups.
Results
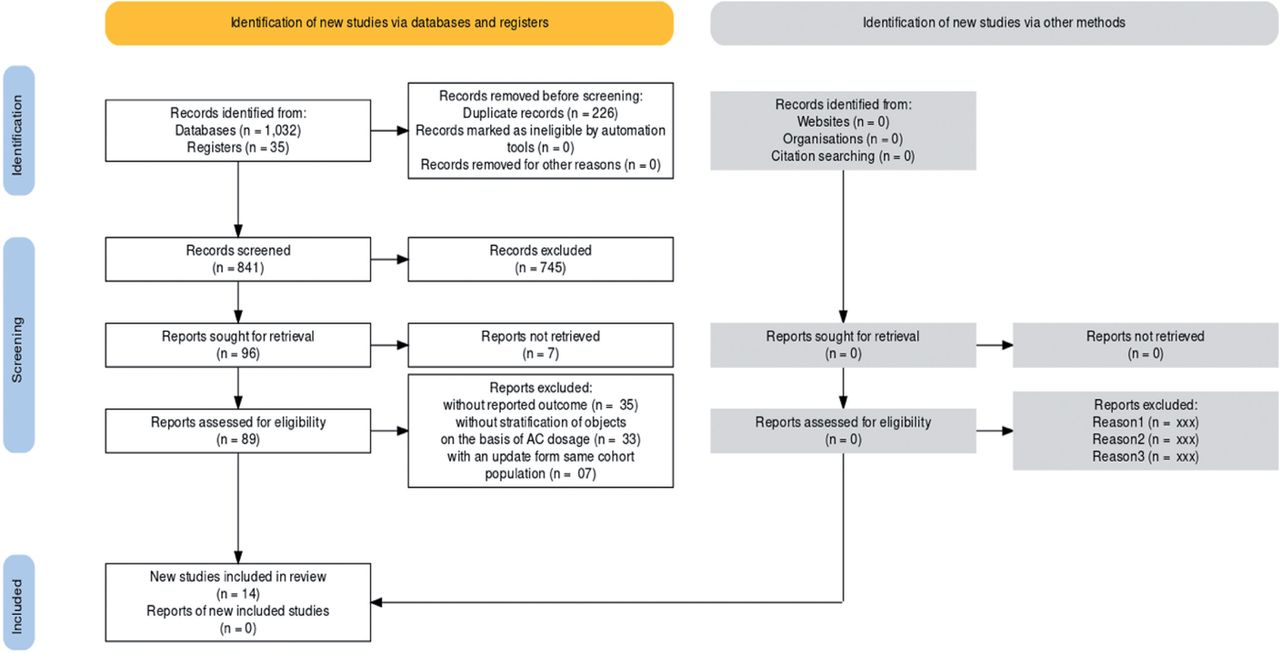
Our search retrieved a total of 1037 titles and abstracts, of which 841 were unique after we deleted the duplicates. We excluded 745 records by screening the titles and abstracts and sought 96 reports for retrieval. We were able to retrieve the full texts of 89 reports and evaluated them further (Figure 1). The 12 that met the eligibility criteria were included in the sample (Table 1).

- Flow chart of database search and studies selection.
A summary of the main characteristics of the 12 included studies and their participants is listed in Table 1. The studies were published between 2020 and 2021. With mortality being the primary endpoint, 11 studies compared the use of prophylactic anticoagulants against therapeutic anticoagulants, while 4 studies compared the no anticoagulant use against the use of prophylactic anticoagulants.
All the included studies were randomized controlled studies (RCTs): 7 were performed in the United States, and the remaining were conducted in the United Kingdom, China, Brazil, Iran, France, and Canada. The total number of participants in all studies was 12,779.The total number of patients who received therapeutic anticoagulation was 2369, and those who received prophylactic anticoagulation were 7002. Overall, 961 patients did not receive any anticoagulation.
Mortality in patients using prophylactic anticoagulants vs. therapeutic anticoagulants
A total of 7120 patients were recruited in 11 studies comparing the use of prophylactic anticoagulants (n=4576) against that of therapeutic anticoagulants (n=2544).
Individually, 6 studies favored prophylactic anticoagulants in terms of reducing mortality, of which 4 were proven to be of statistical significance. The remaining 5 studies showed that using therapeutic anticoagulants was associated with less mortality; however, only 2 studies were reported to be of statistical significance (Figure 2).
- Mortality in patients using prophylactic anticoagulants versus therapeutic anticoagulants.
Cumulatively, the meta-analysis indicated that using prophylactic anticoagulants was significantly associated with a 42% reduction in mortality compared to using therapeutic anticoagulants, OR 0.58 (95% CI 0.676-0.499), p=0.000 (Figure 2).
Mortality in patients not using any anticoagulants vs. prophylactic anticoagulants
A total of 6069 patients were recruited in 4 studies comparing not using any anticoagulants (population n=961) against prophylactic anticoagulants (population n=5118).
Individually, 2 studies significantly favored prophylactic anticoagulants in terms of reducing mortality. The other 2 studies showed that not using any anticoagulants was associated with less mortality; however, only one was barely of statistical significance. (Figure 3).
- Mortality in patients not using any anticoagulants versus prophylactic anticoagulants.
Cumulatively, the meta-analysis showed that using prophylactic anticoagulants was associated with a 5% reduction in mortality but without any statistical significance: OR 1.049 (95% CI 1.237-0.865), p=0.626 (Figures 2 & 3).
Risk of bias
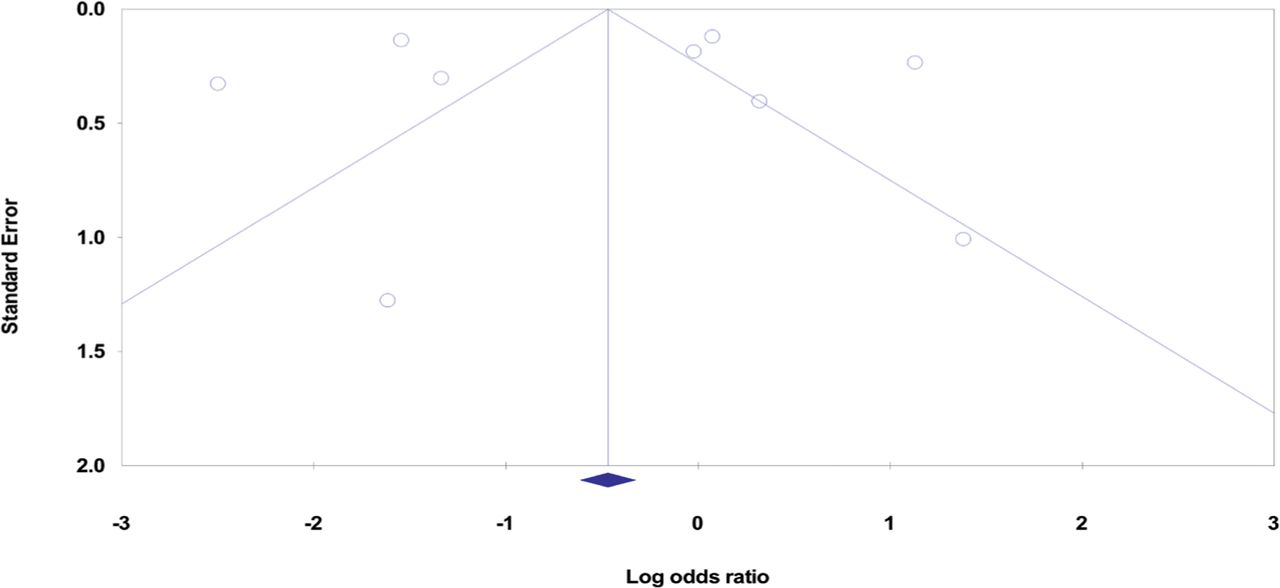
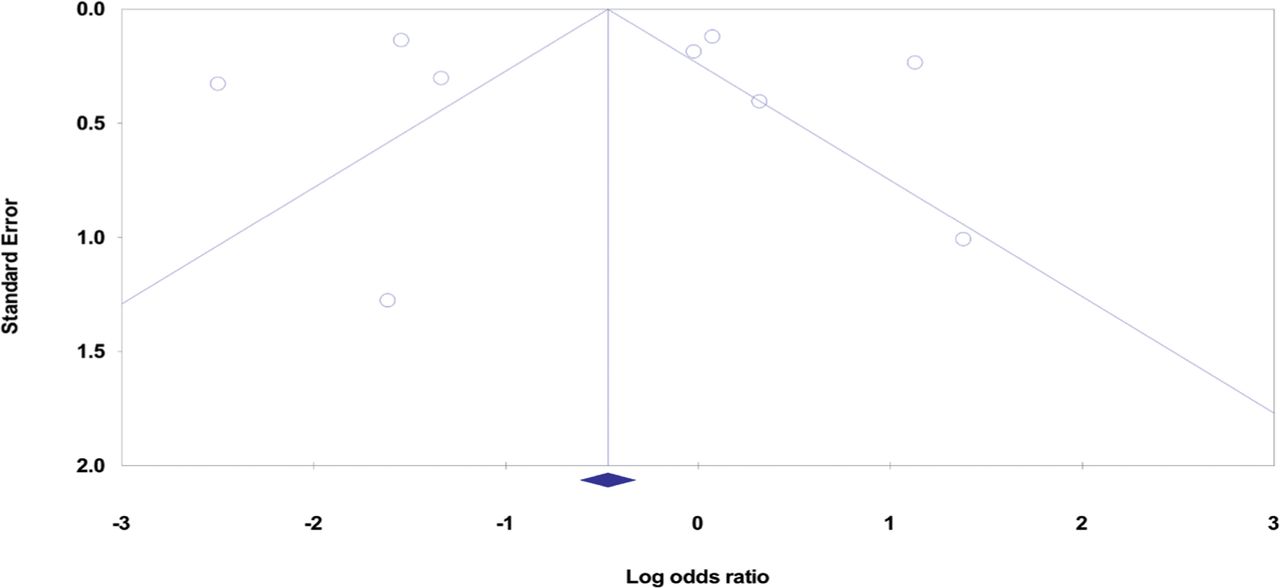
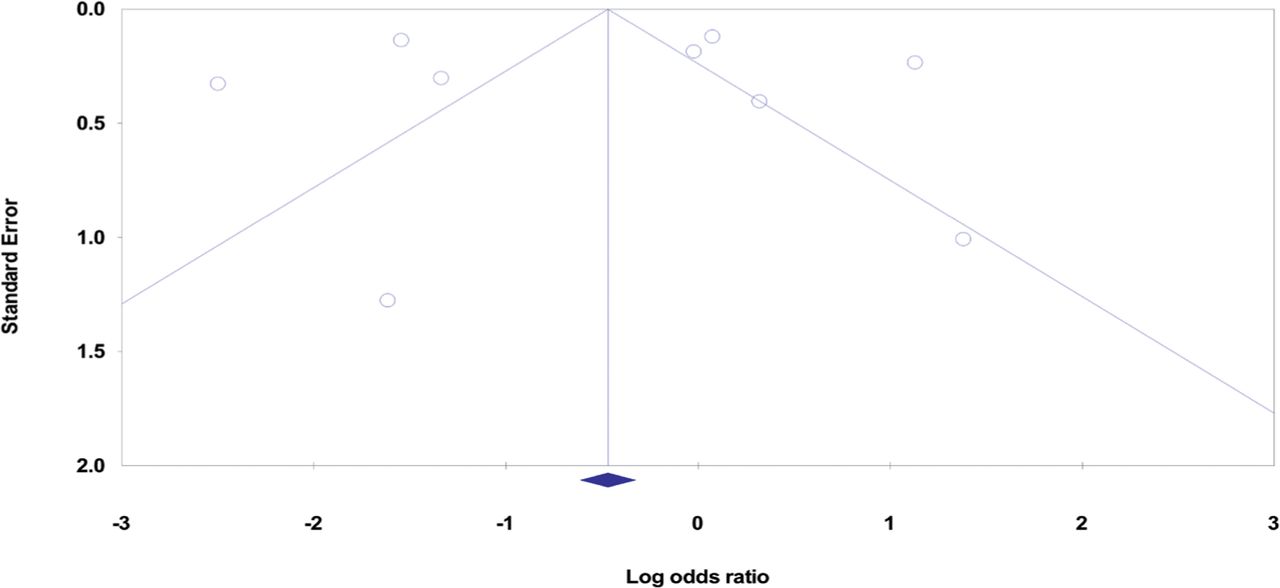
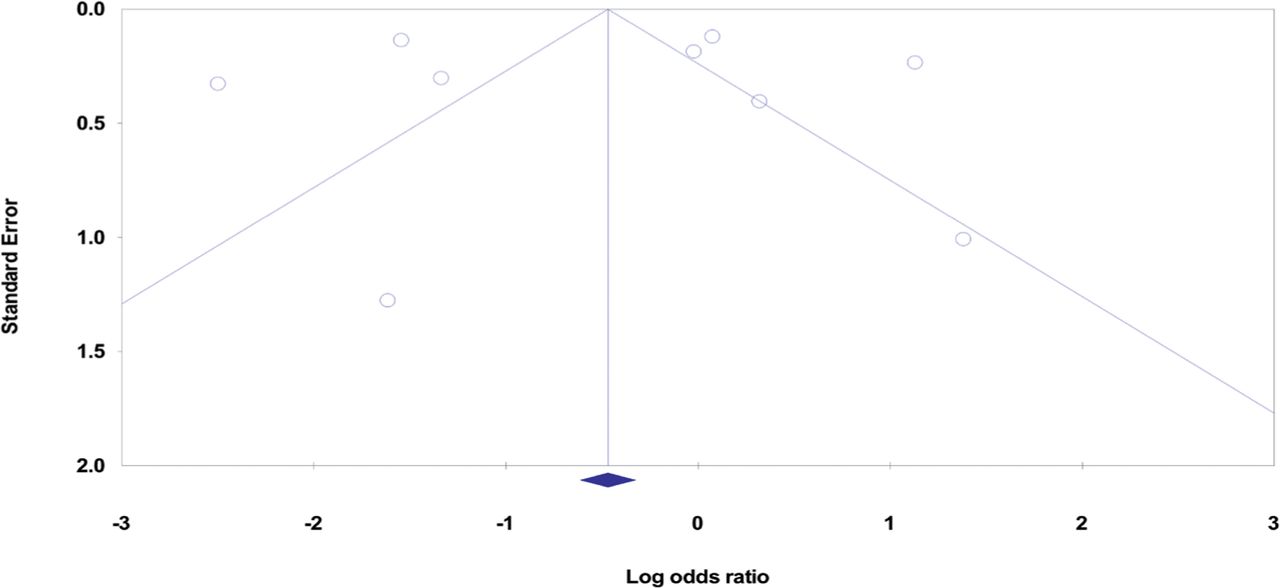
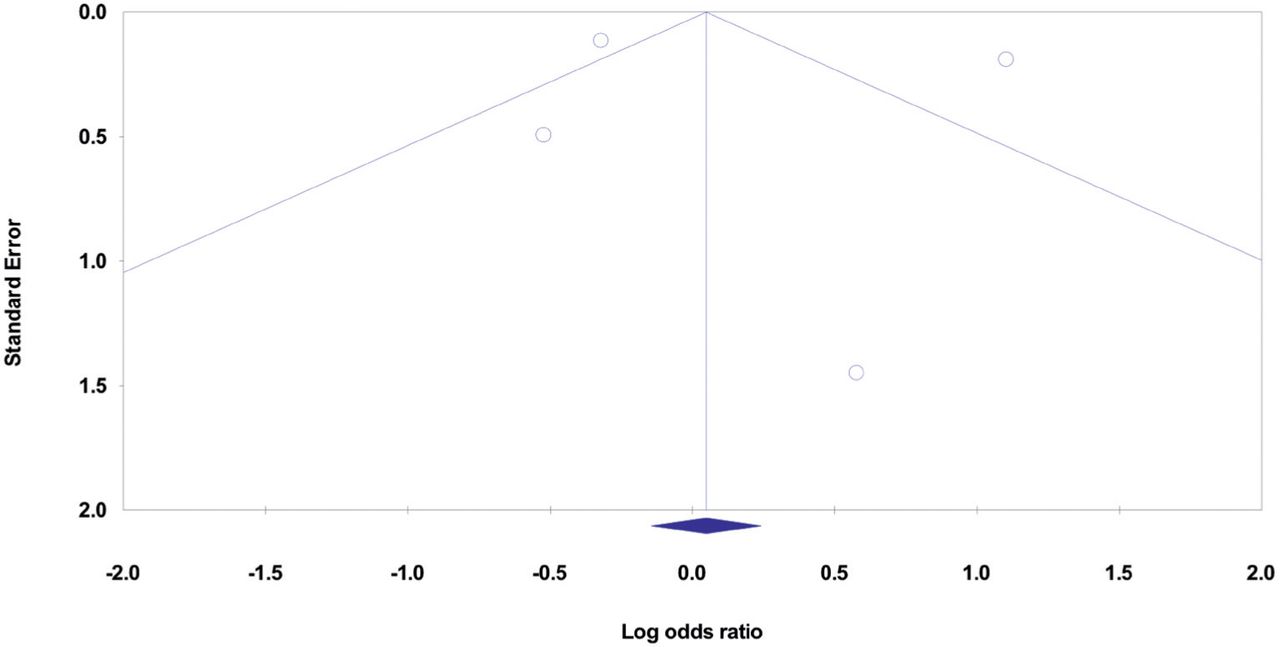
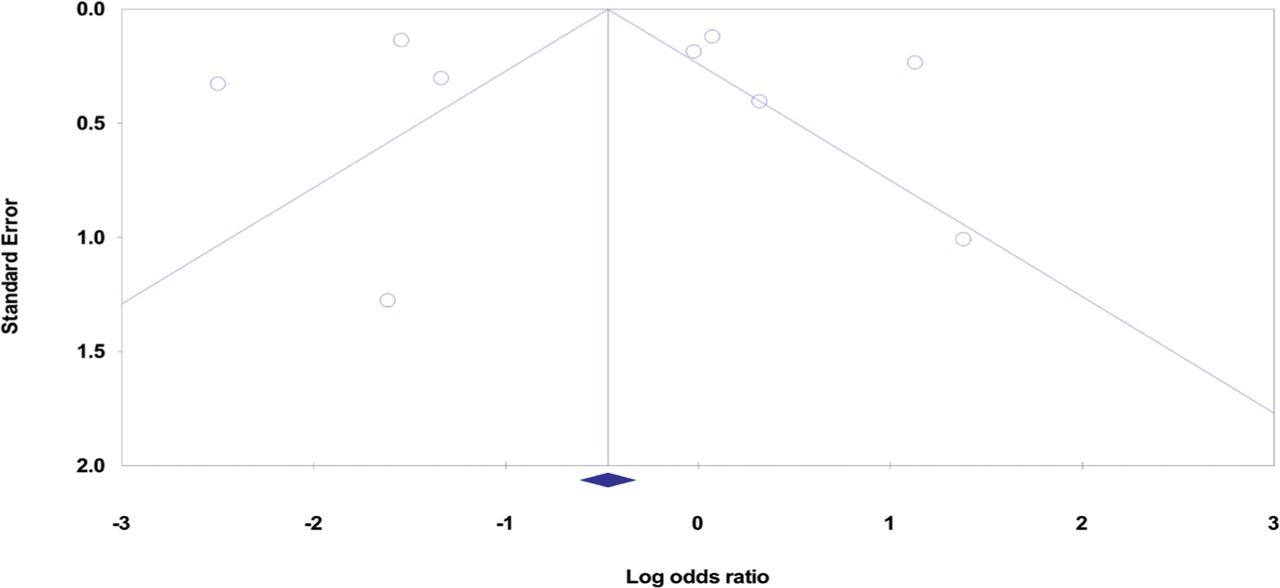
The risk of bias was calculated by doing calculations after removing one study at a time. The risk of publication bias was assessed by making funnel plots of the included studies in both groups and ensuring equal distribution on each side of the funnel plots (Figure 4 & 5).
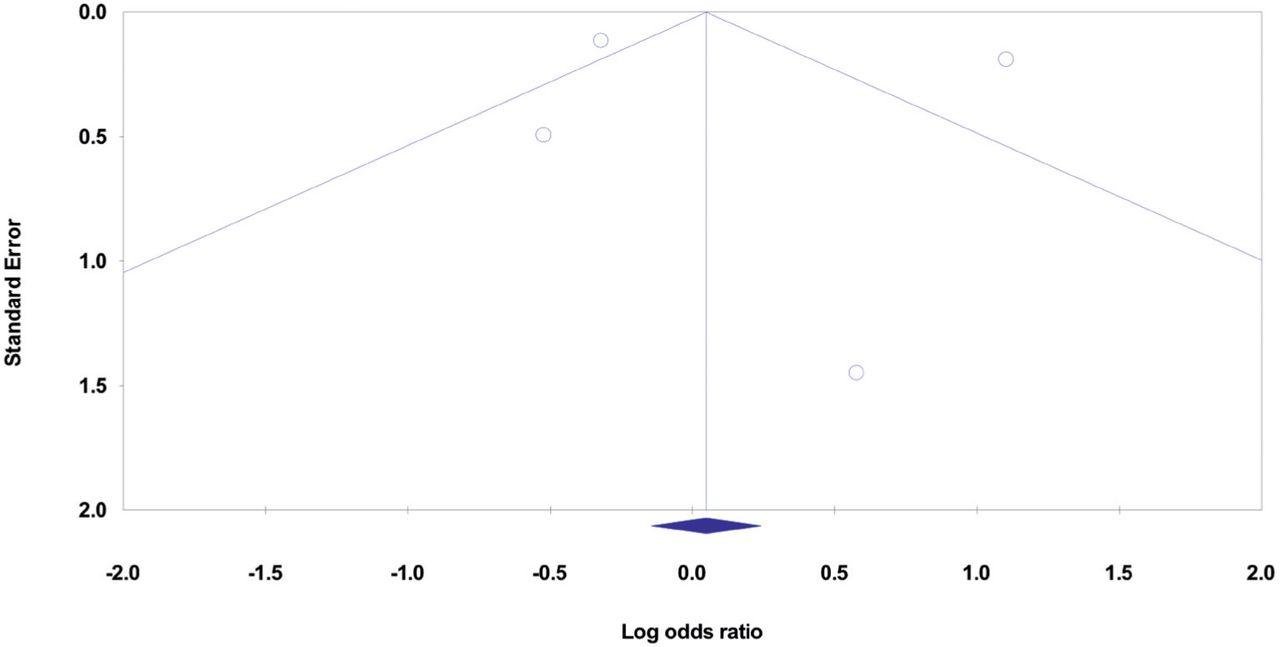
- Funnel plot of standard error by log odds ration. Studies with anticoagulation versus no anticoagulation.

- Funnel plot of standard error by log odds ration. Mortality in patients using prophylactic anticoagulants versus therapeutic anticoagulants.
Discussion
Coronovirus disease-19 has been recognized as a pro-thrombotic condition with a higher incidence of VTE in hospitalized patients.9 There are a number of possible mechanisms for COVID-19-associated-coagulopathy (CAC). It seems that the SARS-CoV-2 virus directly invades the endothelial cells and then enters the cells using ACE-Receptors (Angiotensin-converting enzyme receptors), triggering a thrombo-embolic state.10 Other possible mechanisms include cytokine storm secondary to viral infection as significantly higher plasma cytokine levels have been reported in COVID-19 patients compared to healthy adults.11,12-14 Tumor necrosis factor-α and IL-6 induce the expression of tissue factors which serve as primary initiators of the blood coagulation cascade, possibly leading to a hypercoagulable state.15,16 In addition, the release of ultra-large von Willebrand factor multimers secondary to inflammatory cytokines causes thrombotic microangiopathy, and reduction of vascular heparin-like molecules disrupts anticoagulant pathways.17,18 Lastly, immobility in hospitalized patients results in stasis of blood, which could explain a higher incidence of VTE, particularly in the intensive care unit (ICU) patients.
Di Minno et al19 analyzed 20 studies and concluded that the prevalence of VTE in 1988 hospitalized COVID-19 was 31.3%, with 23% of those patients who developed VTE events during hospital stay being on VTE prophylaxis. In a large multicenter retrospective study, Al Samkari et al20 reported the incidence of VTE to be as high as 6% in COVID-19 patients (including 4% in non-critical admitted patients and 10% in critical patients). However, all study population was on prophylactic anticoagulation. Mai et al21 compared VTE events between COVID-19 and non-COVID-19 patients by analyzing 7 studies in their meta-analysis. They reported that there was a significantly higher incidence of VTE events in hospitalized COVID-19 patients. From the above results, it is evident that hospitalized COVID-19 patients are at increased risk of developing VTE.
Multiple guidelines have been published regarding the initiation of anticoagulation in COVID-19 patients. Nevertheless, there is no consensus upon dosage regime or preference of any specific agent over another. That is because available scientific literature could not establish a single satisfactory protocol for the administration of anticoagulants. For example, there is uncertainty whether a prophylactic dose is beneficial or a therapeutic dose should be administered to reduce mortality. An RCT reported that full-dose anticoagulation was associated with a 4% absolute increase in organ support-free hospital survival in patients not requiring ICU-level support (defined as high-flow oxygen, non-invasive ventilation or continuous positive airway pressure, invasive ventilation, or pressor/inotrope use) when compared to usual-care thromboprophylaxis (27% of whom received intermediate-dose thromboprophylaxis).22 Another study,23 conversely, observed that full-dose anticoagulation did not increase organ support-free hospital survival compared with usual-care thromboprophylaxis (52% of whom received intermediate-dose thromboprophylaxis). Moreover, the drive for anticoagulation therapy is yet to be determined whether it should be the clinical perspective or by using a test, such as D-dimer to monitor anticoagulation therapy. Klok et al24 observed that increasing age and coagulopathy (defined as an elevation in prothrombin time by >3 seconds or activated partial thromboplastin time by >5 seconds) were independent predictors of outcomes though D-dimer levels were not reported in this study.
Our systematic review and meta-analysis examined studies that have analyzed all-cause mortality rate as the outcome in COVID-19 patients in relation to anticoagulation as an intervention of concern. We showed that using prophylactic anticoagulants was significantly associated with a 42% reduction in mortality compared to using therapeutic anticoagulants alone, OR 0.58 (95%CI: 0.676-0.499), p=0.000, and resulted in a 5% reduction in mortality compared to no anticoagulation at all but without any statistical significance: OR 1.049 (95%CI: 1.237-0.865), p=0.626. A prophylactic dose was favored in 4 studies, while a therapeutic dose was rendered beneficial in preventing death in 2 studies, as evident from the results. So it is statistically significant to use prophylactic anticoagulation over therapeutic doses. Surprisingly, prophylactic doses of anticoagulation showed no statistical significance over no usage of anticoagulation.
Lu et al9 concluded in a similar study that no standard regimen of anticoagulants was deemed to reduce mortality, despite higher VTE incidence in COVID-19. In addition, they pointed out 3 studies that concluded that the role of anticoagulation was not adequately addressed due to confounding problems like cardiovascular diseases.26,27 Another meta-analysis by Kolias et al27 also doubted whether anticoagulation was beneficial in reducing mortalityassociated with VTE in COVID-19.
Currently, clinical trials are under process and are still open for enrolling subjects.9,24 However, what has surfaced till now is a not-yet-clear picture regarding the anticoagulation effect in reducing mortality (or for the sake of discussion-to-be-open, increasing mortality - probably and possibly through bleeding defects) in VTE or PE in COVID-19. For instance, a meta-analysis by Hasan et al29 in August 2020 concluded that thromboprophylaxis failure had a high prevalence and they advised that individualized rather than protocolized VTE thromboprophylaxis would appear prudent at interim. But as studies poured in, of different types and strengths, it was deduced from the available that anticoagulation could be of some benefits, but to whom and to what extent are the questions that are still left unanswered. A meta-analysis by Kamal et al29 favored therapeutic anticoagulation over prophylactic when it comes to reducing mortality. Another meta-analysis by Lu et al25 has reported that use of anticoagulation was not associated with increase in mortality; however, it was not shown to reduce mortality either.
The meta-analysis by Lu et al9 was claimed to be the first one, and the confusion they stated regarding the choice of anticoagulation is still there as we are concluding this latest, to our claim, meta-analysis. This lack of clarity makes our study both relevant and significant. Moreover, our study has enrolled a larger population compared to most meta-analyses of its type. It is multicentral and multi-population based (such as, the study population represents different communities from all over the world). Moreover, it includes studies that had a wide age range and comprised both male and female subjects. Lastly, it has been extensively checked for heterogeneity and the risk of bias was evaluated and eliminated.
Study limitations
Studies included were of variable strengths. Also, some included studies did not particularly differentiate between ward patients and ICU patients, which can have a significant effect on mortality.
In conclusion, our meta-analysis favored using prophylactic anticoagulants in COVID-19 patients compared to both therapeutic anticoagulants alone (in a statistically significant manner) and no anticoagulation at all in terms of reducing all-cause mortality
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 22, 2022.
- Accepted April 10, 2022.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.