


Abstract
Objectives: To analyze the clinical and echocardiographic changes in individuals with morbid obesity who underwent bariatric surgery.
Methods: In total, 59 obese patients with body mass index >35 kg/m2 were prospectively enrolled. We assessed baseline pre-operative and a 6-month post-operative lipid profile, hemoglobin A1c, echocardiography, lifetime, and a 10-year risks of atherosclerotic disease for all patients.
Results: The mean patients’ age was 37±12 years, with 40 (67.8%) women. We found that the pre-operative total cholesterol (4.2±1.1 vs. 4.4±1.1, p=0.014) and triglyceride levels (1.4±0.7 vs. 1.8±0.8, p<0.0001) were significantly lower than post-operative levels, while post-operative high-density lipoprotein levels were significantly higher (1.5±0.5 vs. 1.2±0.3, p<0.0001). The calculated 10-year risk of atherosclerotic cardiovascular disease was significantly lower post-operatively (1.1±1.6% vs. 1.6±1.8%, p<0.0001). Echocardiography follow-up revealed that diastolic dysfunction was more prevalent pre-operatively than that post-operatively (41% vs. 10%, p<0.0001). Post-operative left ventricular (LV) mass was significantly lesser than the pre-operative mass (168±252 g vs. 187±255 g, p=0.019), whereas the post-operative LV diastolic (46.5±7 mm vs. 38.5±18 mm, p=0.002) and systolic dimensions (31±5 mm vs. 25±11 mm, p=0.001) were significantly smaller.
Conclusion: Bariatric surgery resulted in a significant amelioration in lipid profile, reduction in LV mass, and LV cavity dimensions.
Obesity is becoming a global health issue with a plethora of medical and economic implications. Its prevalence has significantly increased in the past decade.1 Obesity is defined as a body mass index (BMI) of 30 kg/m2 or greater.1 In Saudi Arabia, approximately 24% of males and 33% of the females are obese, which makes adiposity a major burden on the health care system.2 Multiple comorbidities, such as metabolic syndrome, obstructive sleep apnea, dyslipidemia, hypertension, non-alcoholic fatty liver disease, and left ventricular (LV) hypertrophy, and diabetes mellitus are associated with adiposity.3,4 Furthermore, various obesity-related hemodynamic and structural cardiovascular changes can result in cardiomyopathy, which is characterized by marked increase of LV mass, diameter, and wall thickness with impairment of systolic or diastolic function.5-7
Currently, different techniques for weight loss surgery are being increasingly utilized to treat obesity and thus reduce its long-term public health and economic consequences. Furthermore, bariatric surgery reverses hormonal and hemodynamic changes associated with obesity, resulting in reduced mortality rate and comorbidities.4,8 Regression of LV mass after bariatric surgical intervention has been documented and might have favorable effects on the long-term survival of obese patients.9 Although improvements in cholesterol, insulin, and glucose levels are more pronounced during the first 3 months, cardiovascular changes such as LV mass regression have a more delayed response and follow a linear fashion that persisted for 24 months post surgery.9 In a systematic review involving more than 50 studies, including approximately 16,800 patients, the observed 10-year relative risk reduction in cardiovascular diseases after bariatric surgeries, was approximately 40%.10 Laparoscopic sleeve gastrectomy (LSG) was associated with a higher rate of diabetes remission than other obesity-related comorbidities such as obstructive sleep apnea, hyperlipidemia, and hypertension.11 Another study investigated the effect of LSG on hypertension and demonstrated that LSG had a favorable effect on blood pressure and resulted in significant improvement or full recovery in the majority of cases.12 Nevertheless, the impact of hypertension on the heart, and thus on the possible long-term consequences, is cumulative. Therefore, increased clinical improvement or even resolution of hypertension does not necessarily imply a direct improvement in cardiac function. Cavarretta et al3 retrospectively assessed cardiac remodeling with global longitudinal strain (GLS) and found a significant reduction in the LV mass and wall thickness, but no significant improvement in ejection fraction.
Recent advances in speckle-tracking echocardiography techniques have enabled GLS measurement, which allows for an accurate assessment of the subtle changes in the LV function that are undetectable with conventional imaging techniques.4-6 Global longitudinal strain may be ideal for follow-up and monitoring the effects of interventional treatment on myocardial changes over short time periods.7,13
In this study, we aimed to prospectively assess the changes in the clinical and echocardiographic parameters in obese patients after bariatric surgery.5
Methods
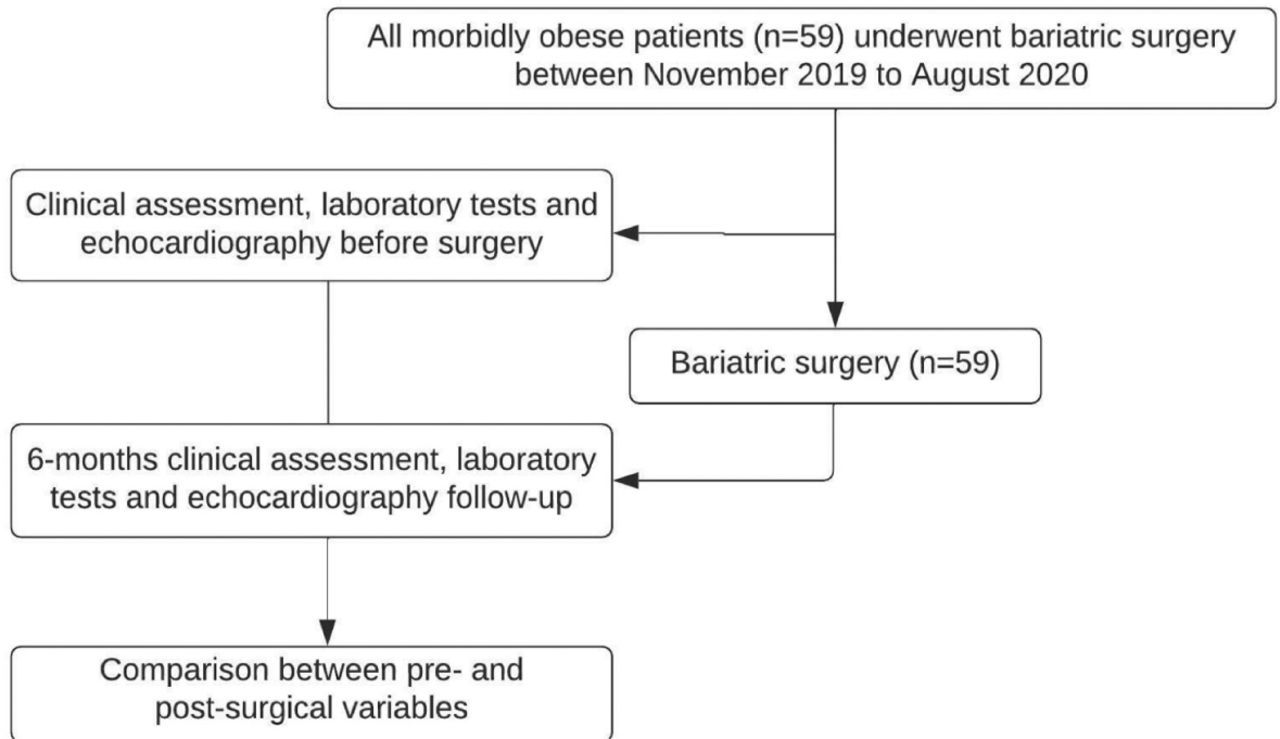
We prospectively enrolled 59 obese patients who were scheduled for LSG. The inclusion criteria were: BMI >40 kg/m2 or patients with BMI of 35-40 kg/m2 if more than one comorbidity factor was documented, age >18 years, repeated failures of the conservative treatment, and no prior history of psychiatric disorders, between November 2019 and August 2020 (Figure 1). Patient demographic data, blood tests, lifetime, and 10-year risks of atherosclerotic disease driven from pooled cohort equations (PCE) were reported. Patients with a history of decompensated heart failure, significant valvular heart disease, ischemic heart disease, cerebrovascular disease, or a high perioperative risk were excluded. The study protocol was approved by the local ethical committee, and all patients signed an informed consent form for surgery, enrollment in the study, and follow-up after surgery. This study adhered to the principles of the Declaration of Helsinki.
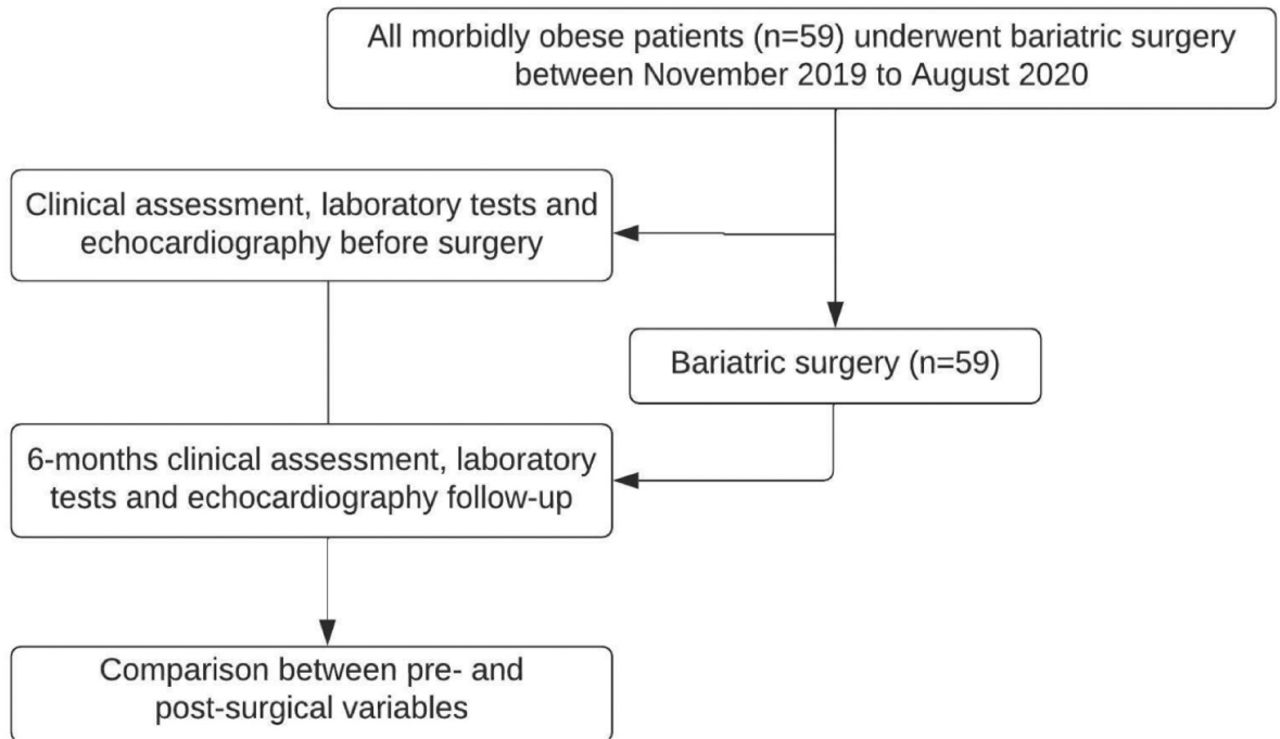
Patients inclusion and follow up.
All candidates underwent full echocardiographic assessment with 2-dimensional echocardiography, color Doppler (Vivid E95, General Electric Medical Systems, Waukesha, WI, USA). Images were obtained from the apical and parasternal windows and were digitally recorded. Images were interpreted according to the International Echocardiographic Societies Standards to measure the LV ejection fraction, LV wall thickness, mass and volume, valvular lesion assessment, and speckle-tracking strain analysis for LV global longitudinal strain.
All patients underwent sleeve gastrectomy under general anesthesia, and surgical techniques were used as described in the previously published international guidelines.14 The surgery was carried out in the reverse Trendelenburg position. Vertical gastric resection was initiated 6 centimeters from pylorus up to the angle of His. Followed by calibration with a 48 Fr bougie aiming to obtain a gastric pouch with approximate capacity of 60-70 ml capacity. Stomach fundus and the greater curvature were dissected 2-3 centimeters from the pylorus with Endo-GIA (Covidien Endo GIA™ 60mm staples with Tri-Staple™ Technology [MA,USA]) staplers, with 4-5 staple cartilages. Lastly, the tube was detached and then the staple line was reinforced by re-attaching the omentum with a V-Lock™ barbed suture size 2-0.
All patients underwent a 7-month follow-up period after LSG. During follow-up, we reported the post-surgical complications, lipid profiles, and lifetime and 10-year risks of atherosclerotic disease using PCE and dose adjustment of antihypertensive or antidiabetic medications. We define diabetes remission as either fasting glucose level of <100 mg/dl or hemoglobin A1c (HbA1C) level <6.0% without using insulin or oral hypoglycemic medications.15 All patients underwent a 6-month echocardiography follow-up to measure echocardiographic variables similar to the pre-operative echocardiographic variables.
Statistical analysis
Quantitative variables were expressed as mean ± standard deviation (SD), and qualitative variables and categorical variables were expressed as frequencies and percentages. The Chi-square and paired sample t-tests were used to compare pre-operative and post-operative baseline characteristics and echocardiographic parameters. A p-value of <0.05 was considered significant.
Results
A total of 59 obese patients with a mean age of 37±12 years (40 women) were included, other baseline characteristics are shown in Table 1. During the follow-up period, we found that post-operative BMI was significantly reduced in comparison to the pre-operative BMI (32.7±6 kg/m2 vs. 45.8±7.7 kg/m2, p<0.001). The total cholesterol (4.2±1.1 vs. 4.4±1.1, p=0.014), triglyceride (1.4±0.7 vs. 1.8±0.8, p<0.0001), and HbA1C levels (5.2±0.6 vs. 5.9±1.2, p<0.0001) significantly reduced post-operatively when compared to those pre-operatively. In contrast, lactate dehydrogenase levels significantly increased post-operatively (1.5±0.5 vs. 1.2±0.3, p<0.0001; Table 2).
- Baseline characteristics.
Pre- and post-operative comparison of the patient’s cohort using paired t-test and Chi-square test.
The calculated 10-year (1.1±1.6% vs. 1.6±1.8%, p<0.0001) and lifetime (34.5±6.7 vs. 39.6±13.6, p<0.0001) risks of atherosclerotic cardiovascular disease using PCE were significantly reduced post-operatively when compared to the pre-operative risks. Interestingly, 3/12 (25%) patients with diabetes were in remission with HbA1C levels reduced to less than 6.0%. Furthermore, 8/12 (66.7%) were advised to stop the hypoglycemic agents and 2/12 (16.6%) to reduce the doses of diabetic medications. A total of 3/9 (33.3%) patients with hypertension were advised to reduce the number or the doses of the antihypertensive medication after surgery.
After a 6-month echocardiography follow-up, the prevalence of diastolic dysfunction was more common in pre-operative status than in post-operative status (41% vs. 10%, p<0.0001), while systolic function (assessed with ejection fraction and GLS) was not significantly different (Table 2). The post-operative LV diastolic (46.5±7 mm vs. 38.5±18 mm, p=0.002) and systolic (31±5 mm vs. 25±11 mm, p=0.001) dimensions were significantly larger. However, the LV diastolic and systolic volumes did not differ. Conversely, the post-operative LV mass was significantly lower than the pre-operative mass (Table 2).
Discussion
In the present study, we prospectively analyzed clinical and echocardiographic changes in patients who were morbidly obese who underwent bariatric surgery. We found that post-operative BMI, total cholesterol level, triglyceride level, HbA1C level, and LV mass were significantly lower than pre-operative levels, while the high-density lipoprotein levels were significantly increased post-operatively. Moreover, two-thirds of the patients with diabetes and one-third of the patients with hypertension showed improvement in disease status and were advised to step-down medications during the follow-up period.
Several reports have investigated the mechanisms underlying the effects of overweight on cardiovascular structures. A high BMI results in increased cardiac stroke volume and output, which leads to LV cavity dilatation and subsequently eccentric LV hypertrophy. Excessive adipose tissue in overweight patients increases insulin resistance, which contributes to an increase in LV mass, influences the levels of circulating angiotensin II, enhances the growth of myocardial tissue, and subsequently stimulates fibrosis, which results in LV diastolic dysfunction.16,17 In this study, approximately 41% of our patients had diastolic dysfunction, which significantly regressed after surgery. Furthermore, the LV mass were significantly reduced post-operatively.
Algahim FM et al9 analyzed the effect of LSG on the myocardium among 15 women with morbid obesity and reported similar results to our study; there was a linear regression of the LV mass over 2 years following surgery. However, in our study, we included patients of both genders.
Many studies have shown that LSG has a favorable impact on patients’ comorbidities. In a retrospective analysis to compare the mortality and morbidity prevalence in obese individuals treated with either bariatric surgery or with conservative management, there was a remarkable mortality reduction (50%) in the surgical arm than the conservative management after 23 years follow-up. In addition, surgically treated patients had a lower incidence of cancer, diabetes mellitus, renal diseases, cardiovascular diseases, and number of hospital admissions.18,19 Furthermore, a recent systemic review of 18 studies (involving approximately 269,000 patients with bariatric surgery and 1,270,000 patients treated medically as a control) after 4.9 years follow-up period, LSG resulted in a lower rate of all-cause mortality, and more importantly, it reduced the rate of hypertension, diabetes, and dyslipidemia.20
Similar to our study, Samson et al21 found that post-LSG, patients had a significant blood pressure reduction with a decrease in antihypertensive medications during the follow-up period. Furthermore, consistent with the present study, Aminian et al22 found that morbidly obese patients treated with LSG had significantly better glycemic control, diabetes remission, and fewer diabetic medications over 6 years post-surgery when compared to the pre-surgical diabetic status.
Study limitations
First, the number of patients was small. Second, all patients underwent only one type of bariatric surgery. Third, our patients were relatively young. Fourth, only patients who were morbidly obese were enrolled. Therefore, the results cannot be generalized to other patients with lower BMI; and lastly, the follow-up period was relatively short.
In conclusion, bariatric surgery resulted in significant regression of LV mass and improvement in lipid profiles and blood glucose levels. In addition, it resulted in a significant reduction in the calculated lifetime and 10-year risks of atherosclerotic disease in patients who were morbidly obese.
Acknowledgment
The authors gratefully acknowledge Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 13, 2022.
- Accepted May 17, 2022.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.