


Abstract
Staphylococcus epidermidis (S. epidermidis) is the most frequently isolated member of the coagulase-negative staphylococci, which colonizes the skin and mucous membranes of the human body. Despite being a component of the normal flora, S. epidermidis can act as an opportunistic pathogen and is frequently implicated in both bacterial and nosocomial infections. Macrophage activation syndrome (MAS) is a rare but potentially fatal disease that occurs as a result of increased activation and proliferation of T lymphocytes and macrophages in response to infections and immune mediated diseases. It is very rare in patients with cystic fibrosis. Here we report a case of an 8-year-old girl with cystic fibrosis and familial Mediterranean fever who developed MAS after contracting a S. epidermidis infection.
Cystic fibrosis (CF) is a genetic disease that predominantly affects Caucasians and leads to significant respiratory tract damage. Staphylococcus aureus and Pseudomonas aeruginosa (P. aeruginosa) are the predominant bacteria in the respiratory tract of CF patients. Staphylococcus epidermidis (S. epidermidis) is a member of the coagulase-negative staphylococci family and is the member most frequently associated with clinical infections.1 Staphylococcus epidermidis is an important agent in hospital-acquired, peripheral and central catheter, medical implant, and surgical site infections.2 Its high prevalence in human skin microflora, widespread colonizes, and expression of several virulence factors, as well as the increased use of medical devices are all contributing factors in these infections.3
Macrophage activation syndrome (MAS) is a severe and often fatal complication that can arise from various pediatric inflammatory disorders, and it is considered a type of secondary hemophagocytic lymphohistiocytosis (HLH).4 Macrophage activation syndrome is rare in CF, and the few documented cases were attributed to respiratory viruses and other pathogens common in patients with CF.1-3 To our knowledge, only one case of reactive HLH caused by S. epidermidis has been previously reported.5
Case Report
An 8-year-old girl with CF (delF508/delF508, pancreatic insufficiency, and chronic P. aeruginosa colonization) and familial Mediterranean fever (FMF; M694V/M694V) presented to Pediatric Pulmonology, Ankara City Hospital, Ankara, Turkey. with new-onset fever, increased cough, and sputum. There was no accompanying abdominal pain, chest pain, or joint complaints. On physical examination, she had 92% oxygen saturation, 36 breaths/minute respiratory rate, bilateral crepitant rales, and clubbing. She was hospitalized for acute worsening of pulmonary symptoms. She had P. aeruginosa growth in her last sputum culture. According to the culture antibiogram results, intravenous (IV) piperacillin-tazobactam and IV amikacin treatment were initiated. Her coronavirus disease 2019 (COVID-19) polymerase chain reaction (PCR) test was negative. After the second day of hospitalization, she no longer required oxygen support and her fever and cough decreased, and she completely recovered within the first week of treatment. On day 12 of treatment, the patient developed a toothache. A dentist examined the patient and carried out tooth extraction and tooth filling.
Clinical findings
One day after the procedure, the patient developed a high fever and her oxygen saturation decreased to 82% in room air. Her general condition deteriorated and she became lethargic.
Diagnostic assessment
The result of COVID-19 PCR test was negative and the patient exhibited no new findings on chest X-ray. Due to persistent fever and detection of gram-positive bacteria in the blood culture, IV amikacin was stopped and IV teicoplanin and IV meropenem were initiated. Staphylococcus epidermidis was detected in 3 consecutive blood cultures collected during the febrile period. Abdominal ultrasonography and echocardiography were normal. Laboratory tests revealed newly developed anemia, hyperferritinemia, hypofibrinogenemia, and elevated transaminases (Table 1). The patient continued to receive colchicine therapy (1.0 mg/day). The interleukin 6 (IL-6) level of this patient was in the normal range. Familial Mediterranean fever was considered an unlikely cause for the febrile illness. The result of COVID-19 PCR and antibody tests were negative. The patient was diagnosed with MAS as a result of an S. epidermidis infection following dental surgery.
- Laboratory values of the patient at admission and during follow-up.
Therapeutic intervention
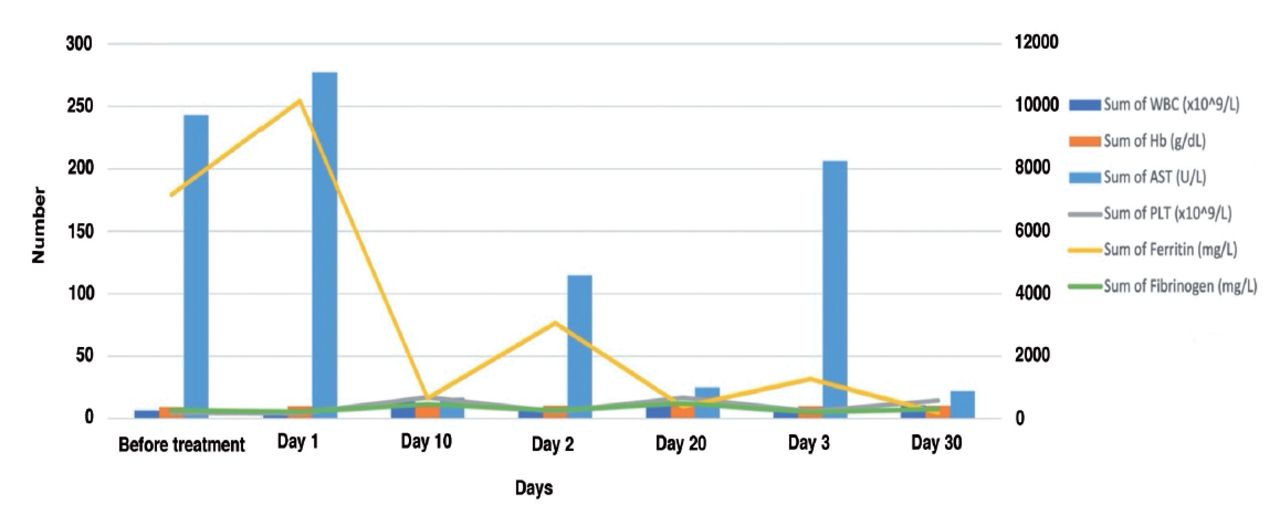
The patient was initiated on IV pulse methylprednisolone therapy at 30 mg/kg/day for 3 consecutive days. Following the pulse corticosteroid treatment, a dramatic improvement was observed in clinical findings and laboratory parameters (Figure 1).

- Therapeutic intervention and laboratory parameters. AST: aspartate aminotransferase, Hb: hemoglobin, PLT: platelet count, WBC: white blood cells
Follow up and outcome
After 2 weeks of observing clinical improvement, the patient was discharged. The corticosteroid therapy was tapered gradually over a period of 3 months until it was completely discontinued (Table 2).
- Patient’s summarized time line.
Discussion
Hemophagocytic lymphohistiocytosis is a severe hyperinflammatory disorder with significant morbidity and mortality in children and adults, categorized as primary or secondary. Secondary HLH is commonly linked to infections but can also arise from underlying conditions such as autoimmune/rheumatologic, malignant, or metabolic disorders.6 Ravelli et al established diagnostic criteria for MAS in systemic juvenile idiopathic arthritis, which also provided a comprehensive definition of secondary HLH, requiring the presence of fever and high ferritin (>684 ng/ml), along with 2 or more of the following conditions: thrombocytopenia (<181×109/L), elevated aspartate aminotransferase (>48U/L), hypertriglyceridemia, and hypofibrinogenemia (<3609 mg/dl).7 The most characteristic feature of MAS is exaggerated hyperferritinemia, and our patient exhibited a ferritin level of 10172 ng/ml.6 In recent years, it has been understood that MAS is not only a phenomenon observed in rheumatologic conditions but is closely related to HLH. It is important to emphasize that if all criteria are sought, MAS cases with an uncertain onset or incomplete clinical expression may not be detected.7
As the patient presented during the COVID-19 pandemic, COVID-19 PCR and antibody tests were carried out to exclude COVID-19 related multisystem inflammatory syndrome in children, and adverse drug reactions were ruled out.
The genetic defect in CF, caused by mutations in the CF transmembrane conductance regulator protein, is believed to impact inflammatory-immune processes, such as cytokine release, phagocyte activation, antioxidant mechanisms, and nitric oxide synthesis and metabolism, leading to uncontrolled elevation of proinflammatory cytokines and impaired monocyte function, ultimately contributing to the inflammatory response in CF.8 In the presented case, MAS may have developed as a result of stimulation by S. epidermidis, with increased pro- and anti-inflammatory cytokines in response to inflammation and localized damage in the airways in CF, increased levels of other cytokines secondary to this inflammatory response. Additionally, S. epidermidis has been shown to cause nonspecific macrophage activation and alter T-lymphocyte activity, which may have contributed to this process in our patient. The literature includes only one reported case of Kikuchi-Fujimoto syndrome complicated by HLH after S. epidermidis infection.5 While there have been only a limited number of reported cases of MAS in CF patients, the increasing awareness of this condition suggests the possibility of a higher number of cases in the future.1-3
High-dose corticosteroid therapy alone is the usual course of treatment for MAS, which differs significantly from other HLH groups in that it does so well our patient’s symptoms and laboratory results significantly improved from the first day of corticosteroid therapy.6
There are 2 documented cases of FMF-associated MAS in the literature. One case was in a 4-year-old patient with previously undiagnosed and untreated FMF who developed severe liver failure, and the other was in an 11-year-old patient with Crohn’s disease and FMF who was receiving immunosuppressive therapy.9,10 In our case, MAS secondary to FMF was not strongly suspected, as the patient’s FMF was well-managed with colchicine therapy, with no FMF-related episodes, complications, organ involvement, or symptoms observed during follow-up in the past 3 years. Innate immune system dysfunction leading to interleukin 1 hypersecretion plays an important role in the pathogenesis of FMF.9 Similarly, uncontrolled activation of the innate immune system is considered the primary cause of the pathogenesis of MAS.7 Considering these conditions, FMF was thought to contribute to macrophage activation in our case. Furthermore, the rapid response to pulse corticosteroid therapy also points to a possible contribution of FMF.
In conclusion, S. epidermidis infections and autoinflammatory diseases may lead to the development of MAS in pediatric CF patients. In cases of rapid and severe clinical deterioration in chronic diseases such as CF, one should be alert for the development of MAS.
Acknowledgment
The authors gratefully acknowledge Jacqueline Renee Gutenkunst for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 22, 2023.
- Accepted September 5, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.