


Abstract
The incidence of malignant transformation in ectopic pancreas (EP), including adenocarcinoma, is extremely rare. Herein, we presented a single case with invasive adenocarcinoma caused by the EP in the stomach. The patient consulted our hospital due to abdominal discomfort with acid regurgitation. Computed tomography scan showed a pyloric obstruction and thickening of the gastric wall in the gastric antrum; a digestive endoscopic examination showed mucosal congestion, swelling in the anterior pyloric area, and pyloric canal stenosis. Next, the patient underwent gastrointestinal surgery, and the distal gastrectomy specimens revealed a deviation of 10 cm towards the lesser curvature and an extension of 22 cm towards the greater curvature. A 5.5 x 5.4 cm round-like mass was found during surgery. Pathological examination suggested invasive submucosal adenocarcinoma located under the gastric antrum mucosa. Our report provides additional clinical experience for diagnosing EP with canceration in the stomach.
An ectopic pancreas (EP) is a pancreatic tissue lacking anatomical communication, vascular communication, or a neural connection with normal pancreatic tissue. Gastric EP, also known as gastric glandular muscle, myoepithelial hamartoma, adenomyosis, or foregut mastoid tumor, is a rare disease that often occurs in the pyloric area of the gastric antrum. Because of the lack of characteristic clinical manifestations, diagnosis is often challenging. Also, although digestive endoscopy and imaging have been improved for diagnosis and technical convenience, distinguishing EP tissue from gastric submucosal diseases is difficult.1
Ectopic pancreas tissue is easily affected by the primary pancreatic tissue of the tumor. Yet, the malignant transformation of the EP is rare, and only a few cases have been described in the literature. Malignant tumors of EP have been found in the upper gastrointestinal tract, with the top 3 incidence rates being the stomach (35.2%), duodenum (22.2%), and jejunum (14.8%).2 Pancreatic tumors reported in EP include anaplastic carcinoma, mucinous cystadenocarcinoma, acinar cell carcinoma, solid pseudopapillary, pancreatic blastoma, perivascular epithelioid cell tumor, neuroendocrine tumors, and adenocarcinoma.2
Herein, we presented a new EP case with epithelial carcinogenesis in the stomach and described the clinical and imaging findings.
Case Report
A 59-year-old female patient consulted our hospital for abdominal discomfort (upper abdominal discomfort, pain, and aggravation of pain after eating) with acid regurgitation. She was in good health and had no history of external injury or surgeries.
Clinical findings & diagnostic assessment
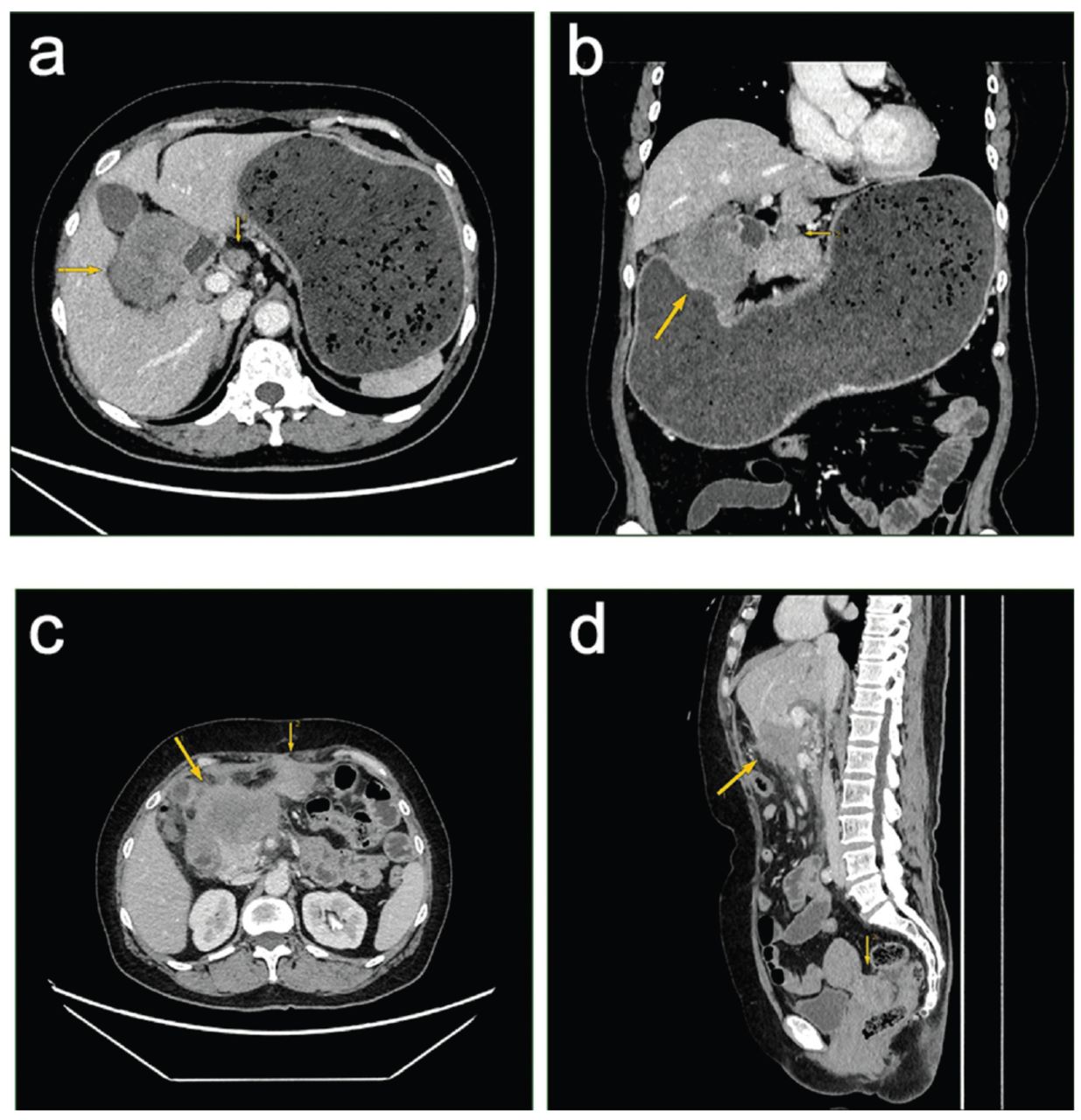
A computed tomography (CT) enhanced scan of the entire abdomen and pelvis showed irregular thickening (irregular soft tissue mass, 5.3 × 6.3 cm) and enhancement of the gastric wall on the lesser curvature of the pyloric stomach and enlarged lymph nodes in the hepatogastric space, approximately 1.7 cm (Figure 1A & B). The size and shape of the gallbladder, spleen, pancreas, and right kidney were normal, and no obvious abnormal density or abnormal enhancement was found. Next, a digestive endoscopic examination showed mucosal congestion and swelling in the anterior pyloric area and pyloric canal stenosis; also, the endoscope failed to enter the duodenum. Therefore, pyloric obstruction and adenocarcinoma were considered.
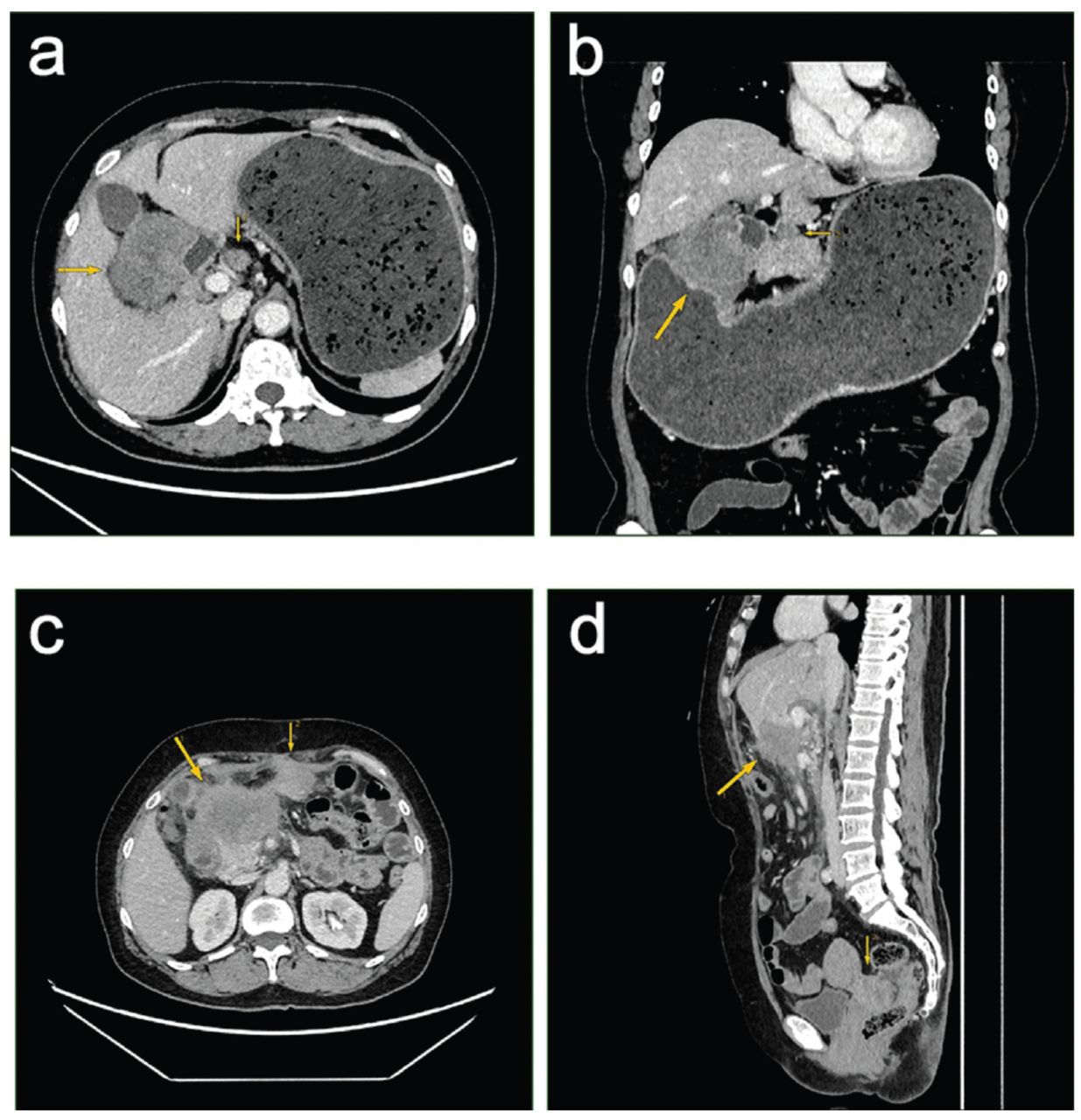
- Results of first (before surgery) and second (12 months post-surgery) pelvic enhanced computed tomography (CT) scan. a & b) The first contrast-enhanced axial CT scan of the upper abdomen revealed an irregular soft tissue mass (thick arrows) on the lesser curvature side of the gastric antrum, measuring approximately 5.3 × 6.3 cm. The mass showed moderate and uneven enhancement. The gastric antrum lumen was compressed, leading to gastric retention and dilation. Additionally, a lymph node enlargement of approximately 1.7cm was observed in the hepatogastric ligament (thin arrows). c & d) The second contrast-enhanced axial CT scan of the upper abdomen and pelvic regions showed (c) an irregular, slightly lower-density mass (thick arrows) below the left lobe of the liver, measuring approximately 6.5 × 6.8 cm. The mass displayed moderate and uneven enhancement, with unclear demarcation from the lower edge of the liver, gallbladder, duodenum, and pancreas. An irregular peritoneal metastatic soft tissue mass (thin arrows) was found beneath the anterior abdominal wall in the left upper quadrant, measuring approximately 3.3 × 3.5cm. d) The contrast-enhanced sagittal CT scan of the abdominal and pelvic regions on the same date showed the same irregular, slightly lower density mass (thick arrows) below the left lobe of the liver, with similar size and enhancement characteristics. The mass had unclear demarcation from the lower edge of the liver, gallbladder, duodenum, and pancreas. Multiple scattered peritoneal metastatic soft tissue masses were observed in the abdominal cavity, mainly concentrated in the Douglas cul-de-sac (rectouterine pouch) in the pelvic floor (thin arrows), measuring approximately 3.9 × 5.4cm.
Therapeutic intervention & pathological assessment
The patient subsequently underwent gastrointestinal surgery. The distal gastrectomy specimens revealed a deviation of 10 cm towards the lesser curvature and an extension of 22 cm towards the greater curvature. During surgery, a 5.5 x 5.4 cm round-like mass was found in the pyloric area, with poor activity and a hard texture located adjacent to one side of the incisal margin and 8 cm away from the other side. The pylorus was narrow, and the pyloric canal was blocked; therefore, a partial gastrectomy, gastrojejunostomy, celiac lymph node dissection, and intestinal adhesion lysis were carried out. The tumor section appeared gray, moderately firm, slightly adhesive, and slippery, with invasion into the serosal layer. Also, multiple lymph nodes were observed, with the largest measuring 0.2-0.5 cm in diameter in the adipose tissue of the lesser curvature of the stomach and several lymph nodes measuring 0.4-0.8 cm in diameter in the adipose tissue of the greater curvature of the stomach. Several nodules measuring 10.0 x 10.5 cm were found in the perigastric accessory omentum, and no distinct nodules were detected.
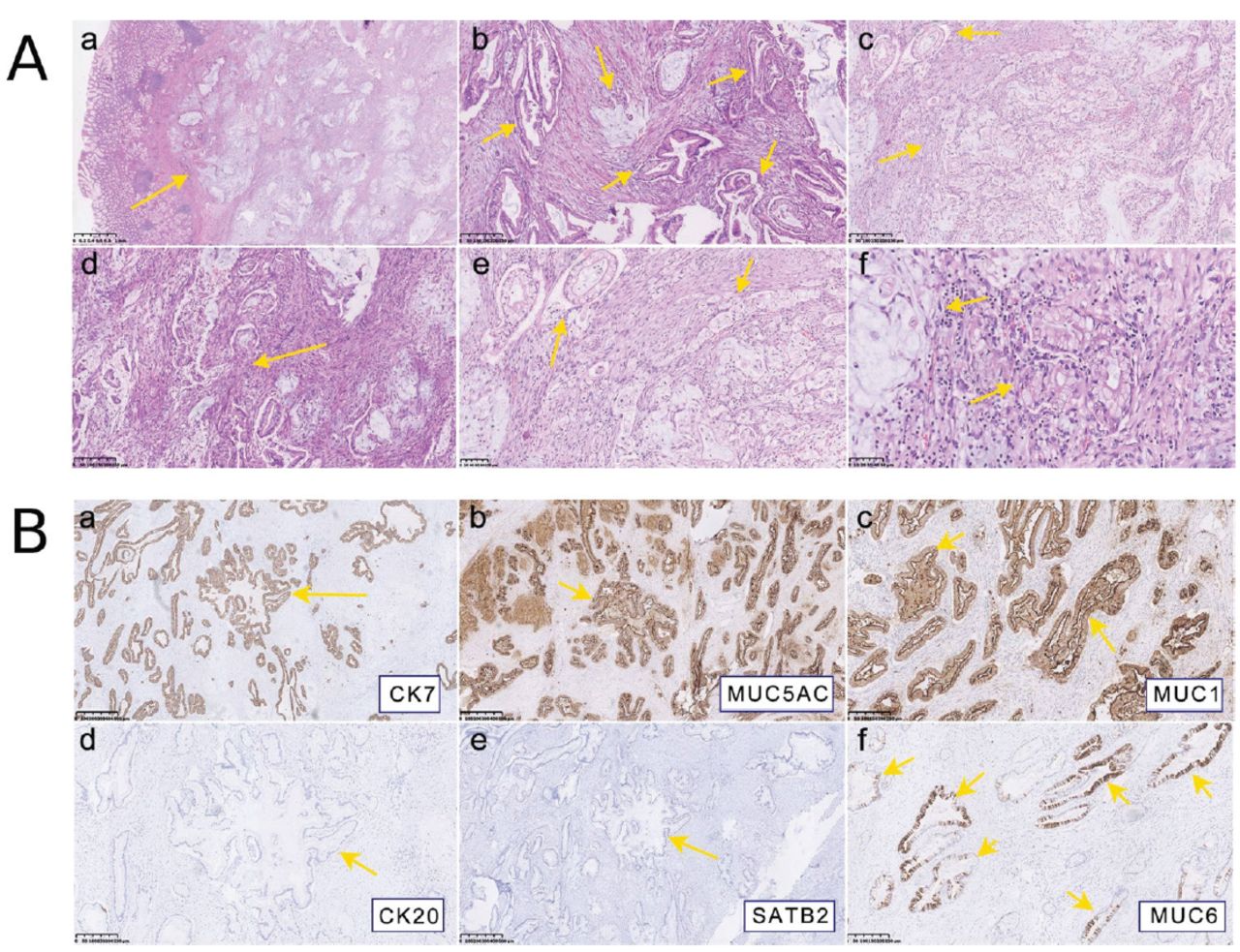
The postoperative specimens were immediately sent to the pathology department for further diagnosis. Under the microscope (Figure 2A), the gastric pyloric canal’s muscular wall and serous layer exhibited significant thickening. The submucosa, muscular, and serous layers showed duct-like structures, some of which displayed cords or cribriform patterns. Certain ducts exhibited cystic dilation and were lined with cuboidal or columnar epithelium, with evidence of papillary hyperplasia. The epithelium appeared atypical, with chromatin-rich nuclei, a high nucleus-to-cytoplasm ratio, and observable mitotic activity. Dysplastic smooth muscle was observed surrounding the ducts, displaying an “onion skin” appearance with a few fibrous bundles and lymphocytes. Ruptured cystic dilated ducts contained many histiocytes, along with a few lymphocytes, and plasma cells. Next, immunochemistry was carried out (Figure 2B). The abnormal glandular epithelium in the lesser curvature of the gastric antrum exhibited strong and diffuse positivity for cytokeratin 7 (CK7), oligomeric mucus gel-forming (MUC1), and MUC5AC. The glandular ducts showed positive staining for CK19 but were negative for caudal-type homeobox 2 (CDX2), CK20, MUC2, estrogen receptor (ER), progesterone receptor (PR), napsin A, and special AT-rich sequence-binding protein 2 (SATB2). The final diagnosis was gastric and pancreatic heterotopic tissue (type III) with adenocarcinoma with epithelial carcinogenesis.
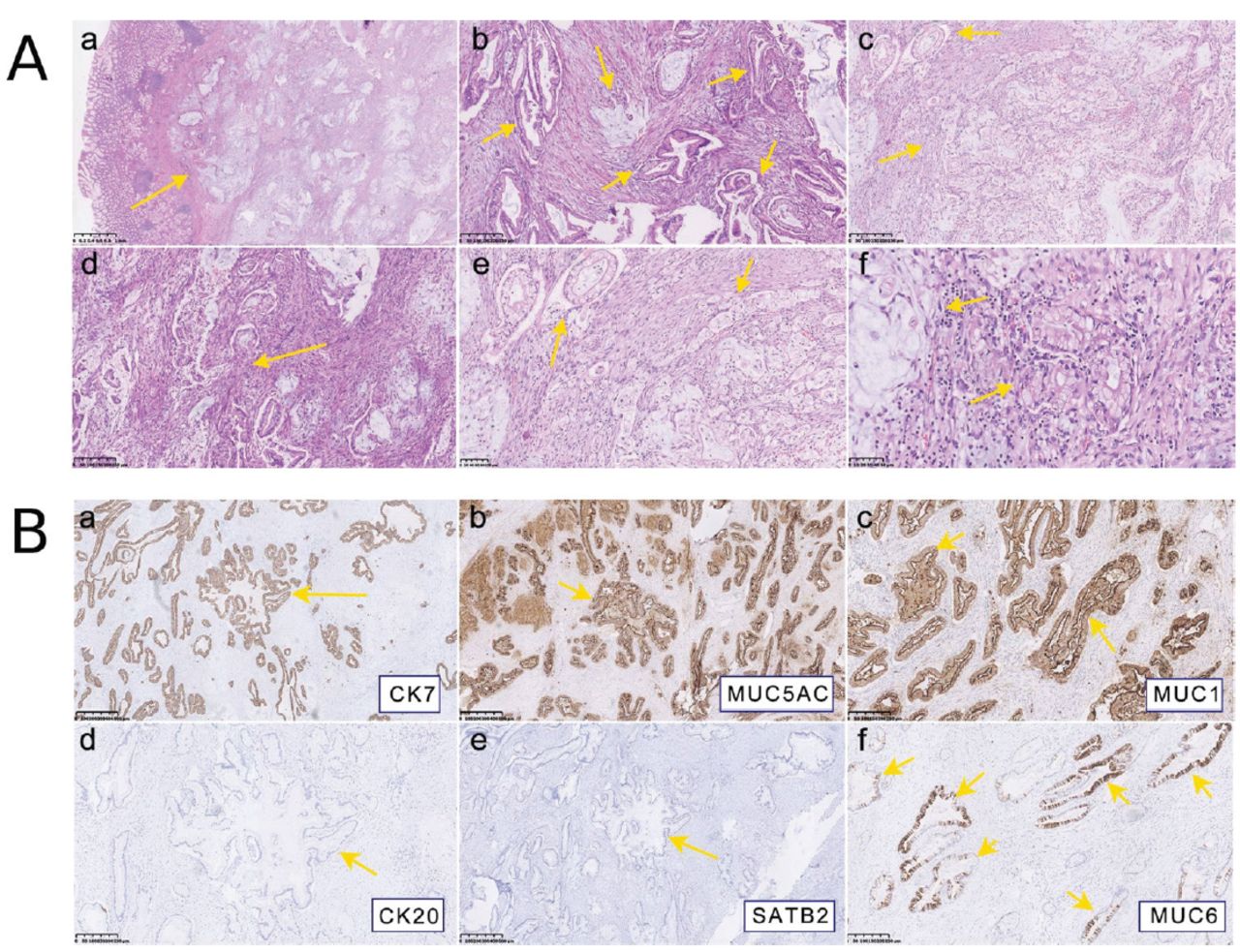
- The A) histological morphology of hematoxylin and eosin (HE) (bar = 500 μm). a) Tumor located under the mucosa; glands of the mucosal layer were normal (HE × 25). b) In some areas, the tumor tissues are arranged in the shape of glandular tubes, and the glands are angled deformities (HE × 100). c) In some areas, the neoplastic glands are arranged in a back-to-back manner (HE × 100). d) Proliferative smooth muscle bundles, fibrous tissue, and inflammatory cell infiltration can be seen around the tumor tissue (HE × 100). e) Tumor cells are rich in the cytoplasm (HE ×200). f) The nucleus of tumor cells was abnormal, and the nuclear membrane was irregular (HE × 400). B) Immunohistology staining (EnVision, original magnification, × 50; bar = 500 μm). a) CK7 (+); b) MUC5AC (+); c) MUC1 (+); d) CK20 (-); e) SATB2 (-); and f) the tumor tissue was positive in some areas of MUC6, and the positive staining was located in the cytoplasm. a-c) The positive expression was localized in the cytoplasm. The CK7, MUC1, and MUC5AC are intensely positive in infiltrating adenocarcinoma tissue, with staining in the cytoplasm and cell membrane. The MUC6 exhibits strong positive expression in some infiltrating adenocarcinoma tissues, with a patchy distribution and strong intensity, also in the cytoplasm and cell membrane. However, CK20 and SATB2 are negative in infiltrating adenocarcinoma tissue.
Follow up & outcomes
The patient was followed up for 4 months, and her general condition was good. During the follow-up, she underwent 6 rounds of chemotherapy and antibiotics (gemcitabine and tigecycline). No tumor recurrence or other organ metastasis was observed 6 months post-surgery. One year after the surgical treatment of pancreatic cancer originating from the ectopic pancreas in the lesser curvature of the gastric antrum, irregular and slightly lower-density tumor recurrence was observed in the surgical area (Figure 1C). Multiple scattered metastatic soft tissue masses of varying sizes were present in the abdominal cavity, mainly concentrated in the Douglas cul-de-sac (rectouterine pouch) in the pelvic floor (Figure 1D). Multiple lymph node metastases were also observed in the abdominal cavity and the retroperitoneum. The timeline was shown in Table 1.
- Patient’s timeline.
Discussion
Most recently, Manhal et al3 reported a rare case of duodenal adenocarcinoma of EP in a 69-year-old man admitted to the emergency department with feculent vomiting lasting 2 days prior to presentation. Herein, we presented a single EP case with adenocarcinoma. Our clinical and imaging findings suggested cancerogenesis (irregular soft tissue mass, 5.3 × 6.3 cm) and enhancement of the gastric wall on the lesser curvature of the pyloric stomach. Pathological examination suggested invasive submucosal adenocarcinoma located under the gastric antrum mucosa.
Most patients with malignant EP have clinical symptoms.2 It has been reported that the size of non-neoplastic EP tissue is usually <4 cm, while malignant EP is >4 cm.4 Our case presented with pyloric obstruction and clinical symptoms (namely, upper abdominal discomfort and pain, aggravation of pain after eating). An enhanced CT scan of the entire abdomen and pelvis showed irregular thickening (measuring approximately 5.3 × 6.3 cm) and enhancement of the gastric wall on the side of the lesser curvature of the stomach in the pylorus. Yet, CT scans and ultrasonography have no specificity for diagnosing EP but can show only the presence of the tumor; thus, biopsy inspection is required. Endoetal et al5 have reported a case of heterotopic pancreatic cancer diagnosed by endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA). This suggests that EUS-FNA may be helpful in preoperative diagnosis. For our case, gastroscopy was preferred; the mucosa in the anterior pyloric area was congested, swollen, and rough; the pyloric canal was narrow; and the endoscope could not enter the duodenum. Further biopsy in the anterior pyloric area showed chronic mucosal inflammation with activity.
In the pathological examination of the disease, the focus was small and occasionally found in other lesions; when the focus was extensive, the mucosa and gastric wall were obviously thickened. In the present study, during the general autopsy, the lesion was located under the mucosa, the section was gray and solid, and some were cystic. Microscopically, the ducts of the cuboidal or columnar epithelium and their proliferated smooth muscle bundles were observed within the tumor area. There was cystic dilation of the ducts, and pancreatic acini and islet cells were found in a small number of cases. We found no cystic dilation of islet cells, pancreatic acini, and Brunner adenoid ducts in gastric tissue. Glandular epithelium showed a papillary, cord-like, or ethmoidal structure, and some ducts were ruptured with a large number of infiltrated histiocytes. Immunohistochemistry further showed diffuse strong positivity for CK7 and negative results for CK20, suggesting that the adenocarcinoma originates from the upper gastrointestinal tract, which is consistent with Song et al6 and Duval et al.7 Also, tumor mass was negative for CDX2, MUC2, and SATB2, further ruling out the possibility of lower gastrointestinal tract origin. In addition, ER and PR were negative, excluding the possibility of breast cancer origin. Finally, napsin A excluded the possibility of lung adenocarcinoma metastasizing to the stomach.
Since the adenocarcinoma is from the upper gastrointestinal tract, CK7 and CK19 were used together to determine if they originated from the bile duct. In this case, CK19 showed partial positivity in the glandular structures, but insufficient evidence supports a diagnosis of bile duct adenocarcinoma. Positivity for MUC5AC and MUC1 (+) further suggested an origin from the stomach or pancreas. Therefore, the diagnosis was gastropancreatic ectopic carcinoma (canceration type III) in the stomach that had undergone carcinogenesis.
According to Heinrich’s classification, there are 3 types of EP tissue: I) the lesion has typical pancreatic tissue (namely, ducts, acini, and islet cells can be seen in the lesion); II) a large number of acini, fewer ducts, and no islet cells can be seen in the lesion; and III) a large number of ducts, no or only a few acini, and no islet cells are seen in the lesions.8 Fuentes et al9 have modified the existing histological classification and added another type of EP - type IV. This type of lesion is composed of endocrine islets without EP tissue. Types I and II gastric adenomyoma are more or less similar to normal pancreatic tissue, so they are not difficult to diagnose, while type III has many ducts and only a small number of pancreatic acini, which requires extensive sampling and careful searches.10
In conclusion, our report provides additional clinical experience, including imaging and clinical findings, for diagnosing EP with canceration in the stomach.
Acknowledgment
The authors gratefully acknowledge Mr. Chunfeng Sun for reviewing the images. The authors also would like to thank MedSci for their English language editing.
Footnotes
Disclosure. This study was supported by the Horizontal project of Nantong University, Nantong, China (no.: 21ZH470).
- Received July 19, 2023.
- Accepted September 21, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.