


Abstract
Objectives: To investigate the effects and safety of lidocaine viscous gargle on postoperative sore throat (POST) in patients receiving a laryngeal mask airway (LMA) in general anesthesia.
Methods: In this randomized controlled trial, 90 patients undergoing urological surgery were allocated into 2 treatment arms (n=45): lidocaine viscous gargle before LMA insertion (Group G) and topical application of lidocaine viscous on the LMA (Group T). Outcome data were collected before placement of LMA (T0), after insertion of LMA (T1), immediately (T2), one hour (T3), and 24 hours after removal of LMA (T4). We analyzed the incidence of POST, pharynx dryness, and adverse events.
Results: The incidence of POST was lower in Group G than Group T at T2 (11.1% vs. 28.9%; p=0.063), T3 (11.1% vs. 24.4%; p=0.167), and T4 (2.2% vs. 4.4%; p=0.566), but there was no significant difference between groups. No patient in either group experienced severe pain or treatment-related adverse events. There was a significantly lower incidence of pharynx dryness in Group G than Group T (p<0.05) at T2, T3, and T4.
Conclusion: Lidocaine viscous gargle showed no statistically significant difference in incidence of POST and incidence of pharynx dryness compared with topical application of lidocaine on the LMA. Both approaches were safe for patients receiving LMA.
Chinese Clinical Trial Register No.: ChiCTR2200059720
Laryngeal mask airway (LMA) is currently widely used during general anesthesia because of its low-level stimulation, high air tightness, and easy operation in the management of the supraglottic airway.1,2 Laryngeal mask airway is also effective at reducing the incidence of peri-operative airway adverse events.3 However, the incidence of sore throat with the application of LMA is high, ranging from 32-44%, which significantly affects patient satisfaction and quality of life even after discharge, especially among patients who have a short operative time.4,5 In clinical practice, strategies to prevent sore throat after LMA include procedural approaches, such as partial inflation with air pre-insertion and appropriate intra-operative pressure control of the laryngeal mask cuff, and pharmacological approaches, such as intravenous nonsteroidal anti-inflammatory drugs (namely, flurbiprofen), or topical benzydamine hydrochloride.5-7 However, these measures have not been reported to significantly reduce the incidence of post-LMA sore throat.
Inhaled lidocaine as a localized analgesic can reduce inflammation in the airway with less impact on the whole body.8 However, inhaled lidocaine is not effective at reducing inflammation in the throat. Lidocaine viscous is currently used as a lubricant and local analgesic that is smeared on the surface of the LMA, which can relieve post-operative sore throat (POST) and enhance the success rate of LMA insertion. However, application of lidocaine viscous on the LMA can fall off when it touches the back of the tongue during the insertion procedure, resulting in insufficient local anesthesia.5 In addition, local trauma caused by repeat attempts during insertion of the LMA may increase risk of POST.2 We hypothesized that gargling with lidocaine viscous prior to LMA insertion could optimize the local anesthesia and protect the throat mucous membrane. We also hypothesized that an increase in saliva secretion as a result of gargling could relieve pharynx dryness. This study, therefore, aimed to report patient outcomes following LMA and evaluate the effectiveness of lidocaine viscous gargle prior to LMA placement compared with topical application of lidocaine viscous on the LMA in patients who received general anesthesia during ureteroscopic holmium laser lithotripsy.
Methods
This was a prospective, 2-arm parallel randomized controlled trial clinical study carried out at the First Affiliated Hospital of Soochow University, Suzhou, China. All consecutive patients who underwent ureteroscopic holmium laser lithotripsy under general anesthesia from June 2022 to August 2022 were screened, and those who met the inclusion criteria were enrolled in our study. The inclusion criteria were: I) age between 18-65 years old; II) American Society of Anesthesiologists (ASA) physical status grade I-II9; III) Mallampati grade I-II10; and IV) scheduled for elective minor urological surgery. The exclusion criteria were as follows: I) operation time of >2 hours; II) had difficulty opening mouth wide enough for LMA placement; III) had symptoms of sore throat before LMA; IV) had acute upper respiratory tract infection within 14 days before recruitment; V) with reactive airway disease, including anatomical airway abnormalities and bronchial asthma; VI) body mass index (BMI) of >30; VII) with high risk of reflux or aspiration; and VIII) history of lidocaine allergy. A total of 90 patients fulfilled these criteria and were enrolled in the study. The current study was approved by the institutional ethical review board of the First Affiliated Hospital of Soochow University, Suzhou, China. All methods were carried out in accordance with the relevant guidelines and regulations of the Declaration of Helsinki. All participating patients signed an informed consent form before they were included in the study.
Patients were allocated into 2 treatment arms (Group G and Group T; 45 patients per group) using a random number table. The allocation numbers were placed in opaque, sealed envelopes, and opened before LMA placement. The participating patients and study outcome assessors were blinded to the intervention allocation.
The patients in this study fasted from solid foods for 8 hours and fasted from liquids for 4 hours before surgery. No patient received pre-operative medication. After the patient entered the operating room, the peripheral venous catheter was placed, and patient vital signs were monitored during the general anesthesia, including heart rate (HR), electrocardiogram (ECG), saturation of peripheral oxygen (SpO2), bispectral index (BIS), and mean arterial pressure (MAP). Prior to general anesthesia, all patients received an infusion of 6 mL/kg of sodium (Ringer’s) lactate solution.
Patients in Group G received 2 mL of 2% lidocaine viscous gargle (Handan Kangye Pharmaceutical Co., Ltd., China. Approval no. of the National Medical Products Administration [NMPA]: H13021217) 10 minutes before insertion of the LMA, which was evenly smeared with lubricating saline before use. Patients in Group T gargled 2 mL of 0.9% saline 10 minutes before insertion of the LMA. Lidocaine viscous was evenly applied to the front and back of the LMA. The lidocaine viscous, saline, and LMA (disposable double-lumen, NMPA approval no.: PMDE38) were the same in both groups.
All patients received 2 mg/kg of propofol, 2 ug/kg of sufentanil, and 0.1 mg/kg of cisatracurium intravenously. After the neuromuscular blockade was in effect and the BIS dropped below 60, an experienced anesthesiologist used the same approach to insert the LMA via the patient’s mouth. An inflatable cuff with a standard volume was used. The operators checked and confirmed that the LMA was placed in the appropriate position and there was no air leakage prior to fixing the position of the LMA and starting mechanical ventilation. The tidal volume (8-10 mL/kg), respiratory rate (10-12 times/minute), and the end-tidal carbon dioxide tension (PETCO2: 35-45 mmHg) were maintained at standard levels. General anesthesia was maintained with sevoflurane and sufentanil (2 ug/kg) during the surgery. The anesthesiologist removed the LMA after the patients were awake, and their spontaneous breathing and muscle strength were restored post surgery. If a bronchial spasm occurred during the LMA removal, 1-2 mg/kg of propofol and positive airway pressure face-mask ventilation with oxygen were used. Before the end of surgery, patients in both treatment arms received 50 mg intravenous flurbiprofen axetil as an analgesic. If a patient had severe POST, 50 mg of flurbiprofen axetil was administered intravenously and the use of analgesic was recorded.
Patient demographic parameters (including age, gender, height, weight, and BMI) were documented. The prespecified outcomes were measured at 5 timepoints: before LMA placement (T0), after LMA insertion (T1), immediately after LMA removal (T2), one hour after LMA removal (T3), and 24 hours after LMA removal (T4). In the First Affiliated Hospital of Soochow University (Soochow, China) practice, the anesthesiologist removed the LMA after the patients were awake so that POST could be assessed at T2.
The primary outcome was the incidence of POST at T2, T3, and T4. Severity of POST was measured using a numeric rating scale ([NRS]; range of score: 0-10; no pain: 0, mild pain: 1-3, moderate pain: 4-6, and severe pain: 7-10).11-13 The number of the patients who rated ≥1 on the NRS were considered the event number of POST for the incidence at a given time point. The number of patients who rated scores of 0-10 on the NRS are also presented as categorical data.
We also measured and reported the following outcomes in the 2 study groups: peri-operative data of ASA grade, Mallampati grade, changes in hemodynamic indexes of MAP and HR between T0 and T1, and operative time; LMA procedural outcomes of airway pressure, LMA cuff pressure, number of LMA insertion attempts, and whether blood was observed on the LMA cuff; the number of laryngeal mask insertions until success; the pressure of the laryngeal mask cuff and the airway pressure; the incidence of pharynx dryness at T3 and T4; and adverse events such as hoarseness and laryngospasm at T2.
We determined the study sample size based on the primary POST outcome at all prespecified post intervention timepoints (T2, T3, and T4), which was up to 24 hours after LMA removal. Based on the results from previous studies,14-17 we used the estimated event rate of 35% in patients receiving the LMA with topical lidocaine application and the estimated event rate of 10% in patients receiving lidocaine viscous gargle prior to LMA. We calculated that 90 patients (45 per group) could achieve an 80% power to detect POST at the p=0.05 level of significance.
Statistical analysis
The Statistical Package for the Social Sciences for Windows, version 20.0 (IBM Corp., Armonk, NY, USA) was used. Categorical variables, such as gender and ASA grade, are expressed in frequency, and the Chi-square test was used for between-group comparisons. Continuous variables are expressed as means with standard deviation (SD) when normally distributed and the t-test was used for between-group comparisons. The Mann-Whitney-U test was used for NRS score comparisons. A p-value of <0.05 was considered significant.
Results
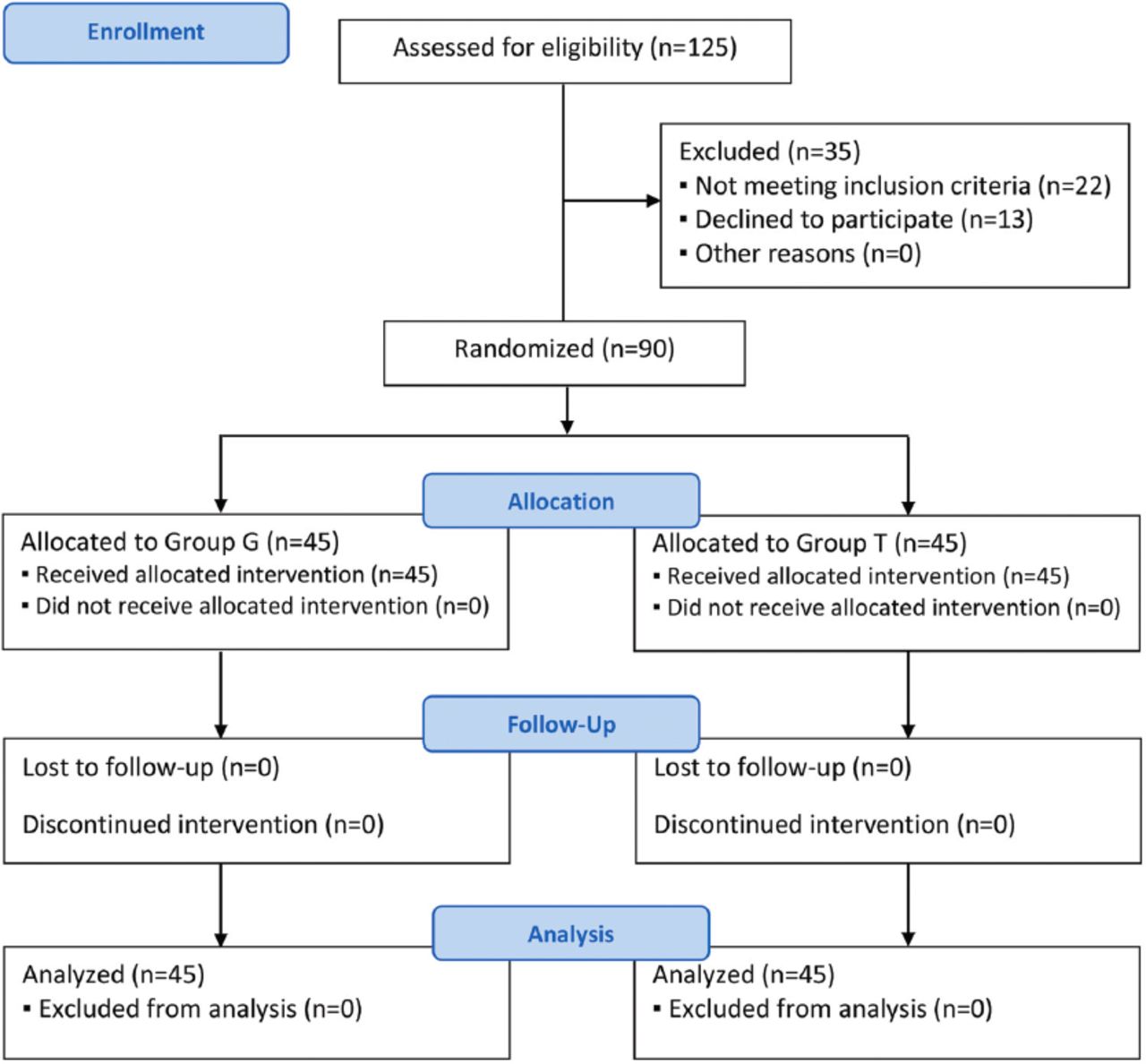
Of the 125 patients who underwent the screening during the study period, 22 did not meet the inclusion and 13 did not consent to participate in the study; thus 35 patients were excluded from the study. There were no missing values at any time points of outcome evaluation. Figure 1 shows the Consolidated Standards of Reporting Trials flow diagram for patient inclusion in this study.18
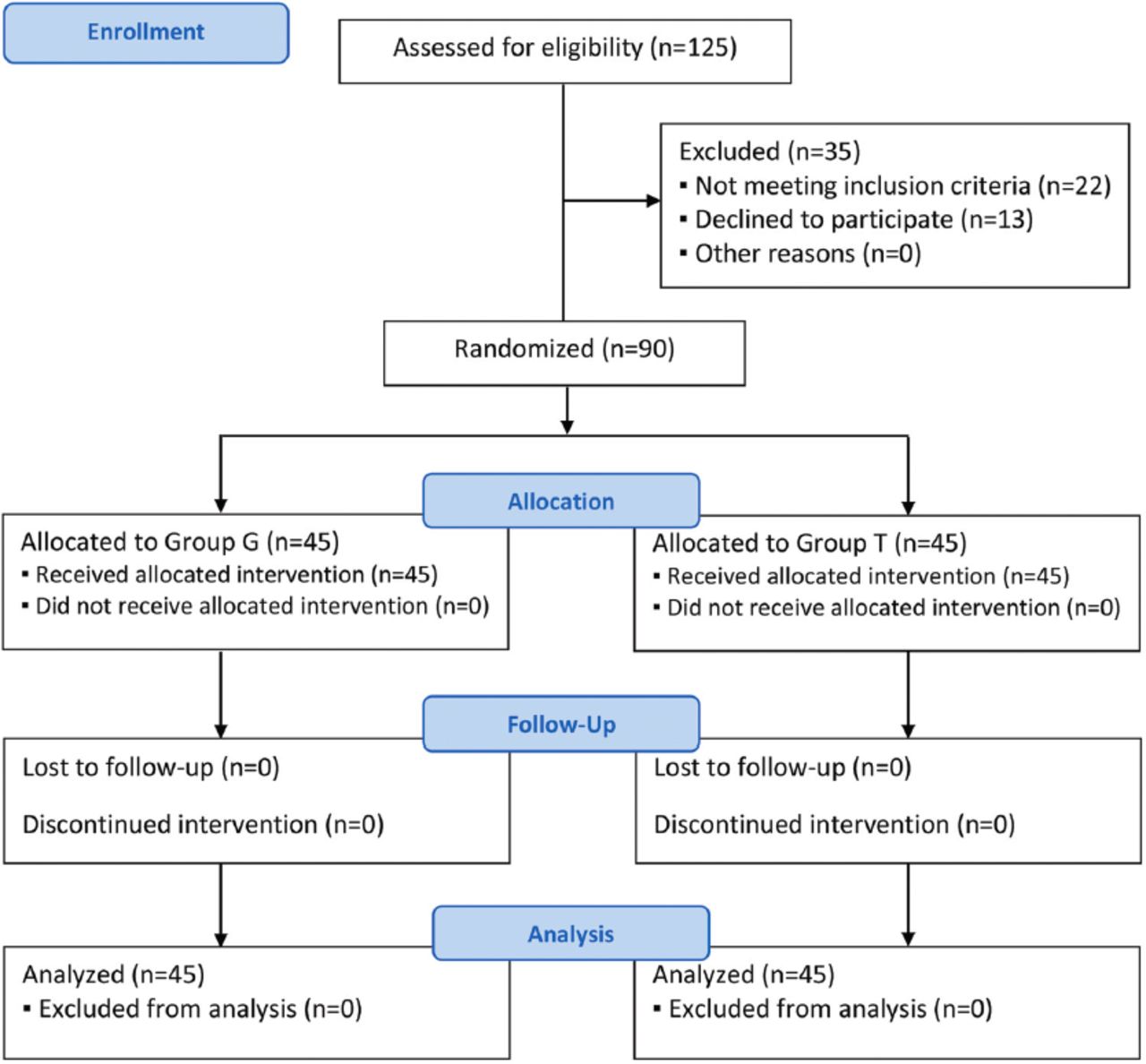
- Consolidated Standards of Reporting Trials (CONSORT) flow diagram of patient inclusion. Group G: lidocaine viscous gargle, Group T: lidocaine viscous topical application on laryngeal mask airway.
There were no significant differences in patient demographic characteristics, peri-operative data, and LMA procedural outcomes (p>0.05, Table 1). There were no significant differences between the treatment arms for MAP and HR between groups after (T1) or before insertion of the LMA (T0, p>0.05, Table 1).
- Demographic and clinical characteristics of patients.
The incidence of POST was 11.1% (5/45) in Group G and 28.9% (13/45) in Group T immediately after removal of the LMA (at T2, p=0.063 between groups). There was a significant difference between the 2 groups for severity of pain in categorical analysis based on discrete scores of pain NRS (number of patients with NRS score of 0, 1, 2, 3, 4, and 5 as categorical variables, p=0.020) at T2. There were no between-group significant differences in the incidence of POST and categorical analysis of pain NRS at one hour after removal of the LMA at T3 (p=0.167, Table 2). No significant difference was found in the incidence of POST between the 2 treatment arms (2.2% [1/45, NRS rated as 1] in Group G versus 4.4% [2/45, NRS rated as 1 for both patients] in Group T) 24 hours after removal of the LMA at T4 (p=0.566). No patients in either treatment arm experienced severe pain in POST (NRS of ≥7 points) at any time. There was no repeated use of analgesics due to POST.
- Comparison of postoperative sore throat between the 2 groups.
There was a significant incidence of pharyngeal dryness in Group G compared with Group T at T2, T3 and T4 (p<0.05, Table 3). No treatment-related adverse events (laryngospasm, hoarseness, dysphagia, nausea, vomiting, irritation, stiffness, allergies, local stinging, or numbness) were observed during this study.
- Comparison of postoperative pharynx dryness between the 2 groups.
Discussion
We compared the use of lidocaine viscous gargle 10 minutes before LMA insertion (Group G) with topical application of lidocaine viscous on the LMA with saline gargle (Group T) in this study. The incidence of POST was lower in Group G than in Group T; however, this difference did not reach statistical significance. There was a significantly lower incidence of pharynx dryness in Group G than Group T at T2, T3, and T4.
Postoperative sore throat is a common complication after LMA placement in patients who receive general anesthesia. The incidence of POST is typically associated with mechanical injury to the mucous membrane due to friction and continuous pressure of the LMA device during induction of anesthesia and surgery. The procedural-related injury may induce local inflammatory responses and increase the risk of postoperative symptoms such as sore throat, dysphagia, and dysphonia.19 Although these adverse events may not directly influence treatment effects of patient primary conditions, these events are especially critical with regard to patient satisfaction and quality of life assessment. These outcomes are particularly important for patients undergoing short, minor surgeries, as surgical site discomfort is usually minor and POST is the major postoperative complaint.19 Because of its technical advantages and easy operation, LMA has been widely used for minor urological surgeries including ureteroscopic holmium laser lithotripsy.3,20
Lidocaine is a topical anesthetic that is easy to apply and has the advantages of rapid analgesic effects, little influence on the whole-body system, low cost, and does not induce airway stimulation. Thus, lidocaine has been widely used to prevent POST in patients who receive an LMA under general anesthesia, mainly via inhalation or topical application on the front and back of the LMA cuff.2,8,21 However, it has been reported that topical application of lidocaine viscous on the LMA does not effectively reduce the incidence of POST.17 In this study, the incidence of POST in patients who received lidocaine viscous gargle before LMA placement (Group G) was 11.1% immediately and at one hour after removal of the LMA (at T2 and T3), which was lower than the incidence reported in the study with topical lidocaine viscous.17
In this study, although a few LMA placements resulted in bleeding after removal in both groups, no patients reported POST with severe pain (≥7 on a 0-10 pain NRS) at rest or swallowing any time up to 24 hours after surgery. The incidence of POST immediately after LMA removal (T2) in Group G (11.1%) was lower than that in Group T (28.9%), but the difference did not reach significance. Changchien et al20 and Bahk et al22 found that topical lidocaine not only effectively improved the LMA insertion conditions, but also reduced the dose of anesthetics during surgery. The topical analgesic effects of lidocaine can reduce transmission stimulation caused by the LMA device when applied to the laryngeal mucosa. Therefore, the strength of the hypopharyngeal muscle is reduced after anesthesia.23,24 Meanwhile, the pressure and friction of the LMA on the mucous membrane of the throat is reduced, thereby relieving the edema and discomfort of the local tissue and mucous membranes.20,25 Lidocaine also has an anti-inflammatory effect through reducing the release of leukotriene B4, which is an inflammatory mediator.26 In this study, gargled lidocaine was given to patients in Group G before the insertion of the LMA, with the aim of reducing the incidence of POST. We also found that the incidence of pharynx dryness at the 3 timepoints (T3, T3, and T4) was significantly lower in Group G compared with Group T. Pharynx dryness might be associated with patient pre-operative liquid fasting. The lower incidence of pharyngeal dryness in Group G may be related to a reduction in leukotriene B4 in the throat after using gargled lidocaine. Further research is needed to verify the effects of lidocaine viscous gargle on reducing the incidence of pharyngeal dryness.
In this study, patients in Group G received lidocaine viscous gargle 10 minutes before the induction of anesthesia while awake. Thus, the lidocaine mucilage was absorbed through the mucosa before LMA insertion. There were no major changes in parameters of MAP and HR prior to and post insertion of the LMA, consistent with the results of a previous report.27 A possible explanation for this finding is that the insertion position of the LMA is above the glottis, which is associated with less stimulation of local tissue compared to what occurs with endotracheal intubation, resulting in less impact on the systemic circulation.
Lidocaine viscous was administered via 2 approaches in this study. Fewer patients experienced POST in Group G than in Group T immediately after removal of the LMA (at T2). No increase in the incidence of POST in either treatment arm was observed one hour after removal of the LMA (at T3), possibly due to the short duration of the surgical operation (≤120 minutes), which was less than the effective period of lidocaine (~150 minutes).2,21 Although the differences at T2 (11.1% vs. 28.9%, p=0.063) and T3 (11.1% vs. 24.4%, p=0.167) were not statistically different, this result could be clinically relevant, as it indicates the potential benefits of lidocaine viscous gargle to prevent POST.
In this study, a few patients still had POST 24 hours after removal of the LMA (at T4), which may be related to the use of analgesics after surgery. Due to the unavailability of data, we were not able to carry out statistical analysis to determine whether analgesics used for postoperative pain, or types and doses of analgesic, were related to the incidence of POST. The low incidence of POST 24 hours after removal of the LMA may be related to the protective effect on the oral mucosa of the remaining lidocaine viscous, particularly in patients in Group G, which could postoperatively improve recovery from any inflammatory response.20,25
No treatment-related adverse events were observed in this study, which indicates the safety of the intervention. Patients in Group G experienced mild to moderate bitterness during gargling, but after removal of the LMA there were no complaints of bitter taste in either group. Further research is needed to improve the taste tolerance of lidocaine to enhance patient satisfaction of the intervention.
Study strengths & limitations
The strengths of this study include its randomized design, homogeneous patient inclusion in terms of surgery type and patient characteristics, use of normal saline gargle to blind the participants of the group allocation, blinding of outcome assessors, no crossover between the 2 groups, and no missing values in the assessment and analysis. However, this study has some limitations that should be noted. First, data on patient and provider (surgeons, nurses, and anesthesiologists) satisfaction were not available. We assumed that, except for the mild to moderate bitterness of the lidocaine viscous gargle, patient satisfaction would be high because of the easy, quick application, and good safety of the intervention. In future studies, it would be valuable to also collect and analyze patient satisfaction data. Second, providers were not able to be blinded due to the different appearance of the lidocaine viscous and saline. However, we think that this limitation was minimal and did not impact the standardized placement of the LMA or outcome assessment. Third, although we met the sample size of our power analysis, the between-arm difference of the overall incidence of POST (whether patients experience throat pain or not) did not meet the level of significance, although the p-value of comparison for POST at T2 was very close to the significance level. Given that we used lidocaine topical application on the LMA in Group T, instead of using a saline placebo for both gargling and topical application, to prevent POST (which was particularly important for patients undergoing minor, short urological surgery), a larger sample size in future studies is necessary to draw better comparisons between groups. Finally, this study involved a single institution and only included patients who underwent the same surgery; therefore, the generalization of the effects of lidocaine viscous gargle may be limited.
In conclusion, lidocaine viscous gargle before LMA was associated with lower risk of POST and incidence of pharynx dryness compared with lidocaine applied on the LMA among patients who received general anesthesia for minor urological surgery. Lidocaine viscous gargle is safe, easy to apply, and not costly. Clinicians may consider this approach before LMA insertion to improve patient outcomes.
Acknowledgment
The authors gratefully acknowledge Medjaden Inc. for thier English language editing.
Footnotes
Disclosure. This study was funded by the National Natural Science Foundation of China (project no.: 8202130), and the Natural Science Foundation of Jiangsu Province, China (project no.: BK20191171).
- Received May 19, 2023.
- Accepted November 8, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.