


ABSTRACT
Objectives: To examine the risk factors for severe bronchopulmonary dysplasia (BPD) in a cohort of very preterm infants (VPIs) in China, as BPD is common among VPIs and associated with a high mortality rate.
Methods: In this multicenter retrospective study, medical records from infants with BPD born at gestation age (GA) of <32 weeks with birth weight (BW) of <1,500 grams (g) in 7 regions of China were included. The cohort was stratified into different BPD severity groups based on their fraction of inspired oxygen requirement at a modified GA of 36 weeks or post discharge. Risk factors were identified using logistic regression analysis.
Results: A significant inverse correlation was revealed between BPD severity and both GA and BW (p<0.001). Independent risk factors for severe BPD (sBPD) were identified as invasive mechanical ventilation (≥7d), multiple blood transfusion (≥3), nosocomial infection (NI), hemodynamically significant patent ductus arteriosus (hsPDA), delayed initiation of enteral nutrition, and longer time to achieve total caloric intake of 110 kcal/kg. Conversely, administration of antenatal steroids was associated with reduced risk of sBPD.
Conclusion: Our study not only reaffirmed the established risk factors of low GA and BW for sBPD in VPIs, but also identified additional, potentially modifiable risk factors. Further research is warranted to explore whether intervention in these modifiable factors might reduce the risk of sBPD.
Clinical Trial Reg. No.: ChiCTR1900023418
Bronchopulmonary dysplasia (BPD) is a respiratory condition primarily impacting preterm infants. The diagnosis of BPD is confirmed when a baby receives oxygen for at least 28 days and requires positive pressure ventilation or oxygen support at 36 weeks’ postmenstrual age or at discharge.1 As reported by the International Network for Evaluation of Outcomes in Neonates, approximately 22% of preterm infants with a gestational age (GA) under 32 weeks and birth weight (BW) below 1500 grams (g) are affected by BPD.2 The severity of BPD is categorized as severe, moderate, or mild.1 The mortality rate associated with severe BPD (sBPD) can reach up to 25%.3
Advancements in perinatology and neonatal critical care over the recent decades have significantly extended the survival rates of infants born <32 weeks of gestation, commonly referred to very preterm infants (VPIs).4 However, despite efforts to prevent and treat BPD with various strategies such as antenatal corticosteroid therapy, surfactant administration, decreased oxygen saturation targets, and more, BPD incidence among preterm infants continues to increase.5 Survivors of sBPD often suffer from neurodevelopmental impairments, cardiovascular comorbidities, and persistent respiratory problems, greatly affecting both their own lives and those of their caregivers.3,6 Therefore, prevention of BPD, especially sBPD, in VPI remains an ongoing research imperative.
Although the prevalence of BPD is high in VPI, far from all are affected and the severity varies. Low GA and BW are recognized risk factors for BPD.7,8 Recent studies have explored the various pre- and postnatal risk factor for sBPD, such as nutrition and ventilation.9,10,11 Yet China, with over one million preterm birth yearly, lacks nationwide multicenter investigation on the matter. The preterm birth rate, especially that of VPIs, shows a continuously increasing trend in China, with acceleration noted.12
This study is designed to elucidate the risk factors for sBPD in China, with the goal of identifying potential targets that can lead to more effective methods for prevention and treatment.
Methods
The Chinese multicenter extrauterine growth retardation (EUGR) collaborative group was established in 2019 to study the morbidity and contributing factors of extrauterine growth retardation (EUGR) among VPIs across different areas of China during hospitalization. Utilizing stratified cluster sampling, hospitals from 7 districts (Northeast, North, East, Central, South, Northwest, and Southwest China) were selected to ensure equal representation. A total of 28 hospitals were included and the proportion of general hospitals, women’s and children’s hospitals, and children’s hospitals were 13:9:6. From September 2019 to December 2020, a total of 2,561 VPIs were prospectively enrolled. The study was carried out according to the ethical principles of the Declaration of Helsinki. The Ethics Committees of Women and Children’s Hospital, School of Medicine, Xiamen University, Xiamen, China, approved the study protocol (KY-2019-016).
The present study retrospectively assessed data on VPIs with BW of <1500 g that have a diagnosis of BPD and were admitted within 24 hours of birth and hospitalized for ≥28 days (n=922). Only infants that have survived over 36 weeks after birth are included. Exclusion criteria included: inherited metabolic disorders or congenital malformation, death during hospital stay, interruption in therapy, self-discharge, or insufficient data. Hospital discharge criteria included: recovery from primary disease, stabilization of vital signs (including discharge with supplemental oxygen), attainment of full enteral feeding (milk volume = 150 mL/kg.d), weight of >1800-2000 g, and modified GA of ≥36 weeks.
As per the national institute of child health and human development (NICHD) consensus statement, BPD diagnosis was confirmed when there was at least 28 days of oxygen receipt and when positive pressure ventilation or oxygen receipt was given at 36 weeks’ postmenstrual age (PMA) or at discharge. According to the NICHD criteria,1 the enrolled VPIs were categorized into 3 groups: mild BPD (n=590, room air), moderate BPD (n=250, FiO2 of <0.3), and sBPD (n=82, FiO2 of ≥0.3, or necessitating respiratory support with positive pressure).
We collected the following data: I) perinatal factors (GA, BW, gender, delivery mode, multiple births, 5-minute Apgar score of ≤7, small for gestational age [SGA], use of antenatal corticosteroids, and presence of gestational hypertension and diabetes); II) complications and major treatments: hemodynamically significant patent ductus arteriosus (hsPDA), neonatal respiratory distress syndrome (NRDS), neonatal necrotizing enterocolitis (NEC) stage ≥2, early onset sepsis (EOS), late-onset sepsis (LOS), nosocomial infection (NI), grades III-IV intraventricular hemorrhage (IVH), periventricular leukomalacia (PVL), metabolic bone disease of prematurity (MBDP), retinopathy of prematurity (ROP), feeding intolerance (FI), EUGR, use of postnatal steroids, anemia, red blood cell transfusions (RBCTs) ≥ 3, cumulative days of antibiotic use, duration of mechanical ventilation (invasive and noninvasive), oxygen time, and overall length of hospital stay; III) growth and nutrition: enteral feeding initiation time, days required to achieve full enteral feeding, parenteral nutrition duration, cumulative fasting days, accumulative fat and amino acid emulsions in the initial week of hospitalization, energy intake within the first week of hospitalization, days of overall and oral calories (each up to 110 kcal/kg/d), days to regain BW, growth velocity (GV) following BW regain, and greatest weight loss.
Detailed definition and diagnostic criteria used for the above conditions are listed in Table 1.
- Definitions and diagnostic criteria.
Statistical analysis
SThe Statistical Package for the Social Sciences, version 25.0 (IBM Corp., Armonk, NY, USA) was used. Continuous data are depicted either as mean ± standard deviation (SD) or as medians (interquartile ranges [IQRs]), whereas categorical variables are shown as numbers and percentages (%). For inter-data comparisons, normally distributed data underwent ANOVA, and skewed data underwent Kruskal-Wallis-H tests. Categorical data were subjected to Chi-square tests. The χ2 partitioning method or Bonferroni test was employed for post-hoc analysis. Spearman correlation analysis assessed GA, BW, and BPD severity links. Ordinal logistic regression was used by multivariate analysis to identify risk factors. A p-value of <0.05 was considered significant.
Results
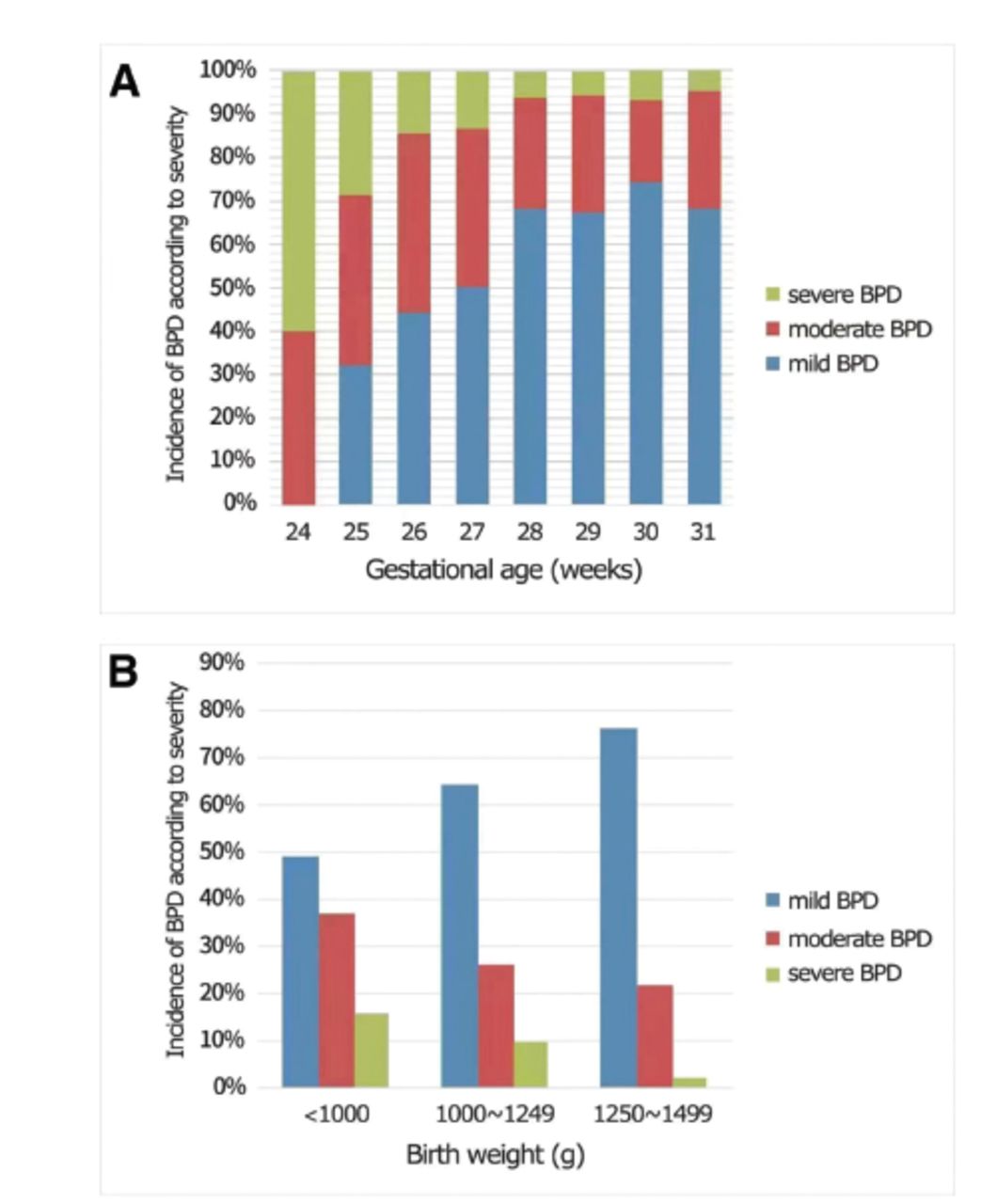
In this study, oxygen or respiratory support was required for 36.0% (922 out of 2561) of VPIs at 36 weeks’ corrected GA or at discharge. The study collected data of 922 VPIs having BW of <1500 g and a diagnosis of BPD. The incidence of BPD was 95.2% (40 out of 42) at 25 weeks’ GA or less, 80.1% (209 out of 261) at 26-27 weeks’ GA, 53.1% (438 out of 824) at 28-29 weeks’ GA, and 16.4% (235 out of 1434) at 30-31 weeks’ GA. Among them, 518 (56.2%) were male, and 404 (43.8%) were female. Mean GA was 28.9 (27.7-30.0) weeks and mean BW was 1150 (970-1300) g. Bronchopulmonary dysplasia severity-dependent stratification of the infants showed that there were 64.0% (590/922) for mild cases, 27.1% (250/922) for moderate cases, and 8.9% (82/922) for sBPD cases. Figure 1 displays a flow chart of the infant selection process. The Spearman’s correlation analysis revealed that both GA and BW were negatively linked to BPD severity (γ= -0.188, -0.230), implying higher BPD severity with lower GA and BW (Figure 2).

- A flow chart of the infant selection process. NICUs: neonatal intensive care units, BW: birth weight, NICHD: the National Institute of Child Health and Human Development, BPD: bronchopulmonary dysplas

- Histogram of bronchopulmonary dysplasia incidence according to severity by: A) weeks of gestational age at birth and B) birth weight. BPD: bronchopulmonary dysplasia
Unlike mild BPD, moderate and sBPD correlated significantly with low GA and BW (p<0.05). Patients with sBPD had higher rates of one-minute Apgar score of ≤7 (p<0.017) and lower usage of antenatal corticosteroid (p<0.05). The sBPD group showed lower GA and BW (p<0.05) and higher occurance of one-minute Apgar score of ≤7 (p<0.017) than the moderate BPD group (Table 2).
- Comparison of baseline characteristics.
Compared to the mild BPD group, the moderate and sBPD groups had significantly higher hsPDA, LOS, RBCTs of ≥3, and invasive mechanical ventilation of ≥7 days (p<0.017 for all) rates, as well as longer cumulative days of antibiotic use, duration of respiratory ventilations (both invasive and noninvasive), and overall length of stay (p<0.05). Moreover, the sBPD group exhibited higher rates of NI, ROP, intervention for ROP, EUGR, and postnatal steroid use (p<0.017). The sBPD group also exhibited higher incidences of hsPDA, NI, and ROP, longer days of postnatal steroid use, higher rates of RBCTs ≥3 and invasive mechanical ventilation of ≥7 days (p<0.017), and longer total hospital stay and durations of invasive mechanical ventilation (p<0.05) than the moderate BPD group (Table 3).
- Comparison of complications and main treatments.
Patients with moderate and sBPD took longer to achieve full feeding and targeted oral caloric intake (110 kcal/kg.d) along with extended parenteral nutrition and cumulative fasting (p<0.05) than those with mild BPD. In contrast to mild BPD, the sBPD group exhibited delayed enteral nutrition, required longer to reach targeted intake of total calorie (110 kcal/kg.d), and exhibited lower initial-week cumulative calories and slower GV (p<0.05). Compared to moderate BPD, those with sBPD exhibited delayed enteral nutrition and required longer parenteral nutrition, cumulative fasting, and targeted total calorie intake (110 kcal/kg.d) (p<0.05; Table 4).
- Comparison of growth and nutrition.
Variables that were significant in the single-variable analysis (Tables 2, 3, and 4) were used in the multivariate analysis (Table 4). However, GA was excluded since GA was highly correlated with BW. The results indicated that after adjusting for BW, the independent risk factors for BPD severity were: invasive mechanical ventilation ≥7 days, RBCTs ≥3, hsPDA, NI, and longer durations required to start enteral feeding and reach total calories of 110 kcal/kg.d. Antenatal corticosteroid was identified as a protective factor.
As seen in Table 5, preterm infants without antenatal corticosteroid had an odds ratio (OR) for sBPD of 2.316 (95% confidence interval [CI]: [1.620-3.310]) compared with those with (χ2=4.61, p<0.001). Those with invasive mechanical ventilation of <7 days had an OR of 0.169 (95% CI: [0.120-0.238]) compared with those without (χ2= -10.12, p<0.001). Those with <3 transfusions had an OR of 0.237 (95% CI: [0.171-0.330]) compared with those ≥3 (χ2= -8.55, p<0.001). Those who did not develop severe hsPDA had an OR of 0.524 (95% CI: [0.377-0.729]) compared with those who developed (χ2= -3.85, p<0.001). Preterm infants did not develop NI had an OR of 0.520 (95% CI: [0.380-0.711]) for sBPD (χ2= -4.10, p<0.001) compared to those developed NI. The OR for sBPD was 1.006 (95% CI: [1.003-1.009]) for each additional day longer required to start enteral feeding (χ2= -4.10, p<0.001). For each additional day to reach 110 kcal/kg.d, the OR for sBPD was 1.019 times (95% CI: [1.002-1.036], χ2=2.21, p=0.0268).
- Correlative factors for the severity level of bronchopulmonary dysplasia.
Discussion
Bronchopulmonary dysplasia negatively impacts preterm infants’ outcomes. Survivors of moderate-to-severe BPD exhibit long-term decline in lung function and poor motor/cognitive development.23 The present study found the prevalence of BPD was 36.0% (922/2561) among VPIs with BW of <1500 g, of which a high percentage had mild/moderate BPD (840/922, 91.1%). Lower GA and BW correlated with greater BPD severity, which is in line with previously reported findings.24,25
As anticipated, the present study showed that VPIs who received invasive mechanical ventilation of ≥7 days had higher odds of sBPD (OR=6.55) than those who did not. This finding is consistent with results reported by Zhang et al26 and Sharma et al.27 It is believed that barotrauma/volutrauma and oxidative stress caused by mechanical ventilation arrest the development of pulmonary vasculature and alveoli.28
Antenatal corticosteroids are currently the standard therapy for preterm infants in higher income countries, but their role in BPD management is debated. Antenatal corticosteroid therapy is believed to promote the surfactant maturation and reduce the incidence of RDS. However, only few studies have found antenatal corticosteroids positively affected BPD, while many other studies have not shown such effects.29,30 They found that there was no significant difference in the incidence of BPD among surviving infants aged 22-28 weeks’ gestational age, regardless of whether they had full or partial antenatal exposure to corticosteroids compared to those without exposure.30 Our study identified antenatal corticosteroid use (OR=0.414, 95% CI: [0.288-0.596]) as a protective factor for moderate-to-severe BPD. This difference may be attributed to the fact that nearly half of the infants included in the present study were of >28 weeks GA, while our data revealed a higher incidence of BPD in infants of <28 weeks GA compared to those of >28 weeks GA.
The present study found that RBCT of ≥3 times, hsPDA, and NI were significantly correlated to an increased risk of sBPD, aligning with prior research.31-35 But the mechanisms behind their impact on lung development is unclear. Red blood cell transfusion might aggravate oxidative stress and cause oxidative injury in the lungs of preterm infants. Hemodynamically significant patent ductus arteriosus might affect lymph drainage, and injury triggered by respiratory ventilation and oxygen toxicity leads to pulmonary edema and the decline of infants’ respiratory status, eventually resulting in BPD.36 Nosocomial infection might increase inflammatory mediator secretion, eventually affecting pulmonary vascular permeability.37 Lapcharoensap et al38 reported that the reductions in NI was linked to lower BPD incidence rates among infants delivered earlier than 30 weeks’ GA and with BW of >1,500 g. However, studies on the effect of aggressive treatment of hsPDA and avoidance of RBCT on BPD severity are lacking. The role of early identification and treatment of NI, hsPDA, and avoidance of RBCT in the management of VPI at risk of sBPD should be further explored.
Nutrition is essential in BPD prevention and control. Bronchopulmonary dysplasia is seemingly exacerbated by malnutrition in a vicious cycle, compromising lung development and functionality. However, feeding difficulties among VPI can affect their nutrition status. Our study revealed that the delay in enteral feeding initiation and a long duration required to achieve total caloric intake (110 kcal/kg/d) constituted the independent risk factors for sBPD. The study involving 207 VPIs with BW of <1000 g by Thiess et al39 demonstrated that moderate-to-severe BPD exhibited evidently lower overall caloric consumption and carbohydrate supplementation during the initial 2 weeks of life compared with the no/mild BPD. Additionally, Al-Jebawi et al40 confirmed that in the case of ELBW infants, low caloric consumption during the initial week of life was linked to an elevated probability of moderate-to-severe BPD (OR=0.94, 95% CI: [0.91-0.97]). The present study suggested that increased BPD severity increases the risk of more severe clinical conditions including delayed enteral feeding (23 hours for the mild group, 24 hours for the moderate group, and 46.5 hours for the sBPD group), delayed full enteral feeding (29 days for the mild group, 33 days for the moderate group, and 36.5 days for the sBPD group), longer parenteral nutrition time (24 days for the mild group, 27 days for the moderate group, and 35.5 days for the sBPD group), fasting time (2 days for the mild group, 3 days for the moderate group, and 4 days for the sBPD group), longer duration of invasive respiratory ventilation, and comorbidities such as hsPDA, RBCTs, NI, and LOS. The worsening respiratory status of infants with BPD frequently interrupts progression to early enteral feeding and even full enteral nutrition, leading to restricted fluid intake and insufficient early calorie intake, which in turn worsen BPD. Therefore, exploration of strategies for early progressive nutrient supplementation could offer potential to decrease the incidence of moderate-to-severe BPD.
It should be noted that compared to the Vermont Oxford or Canadian Neonatal Networks, the morbidities were high in the present study.41,42 This may be due to the lack of prenatal counseling, effective resuscitation teams, and consensus in diagnosis and treatment in many centers in China, including the utilization of prenatal corticosteroids, prophylactic use of surfactants, and noninvasive ventilation support in the delivery room, which significantly affects the survival rates of VPIs without major complications. Moreover, a large proportion of VPIs did not receive comprehensive care and were discharged against medical advices, resulting higher incidences of morbidities among these infants.
Study limitations
The strength of this study lies in data collection from multiple centers, covering 28 grade A level III hospitals in 7 regions of China, which ensures data reliability. However, the study has some limitations. First, different strategies were used for perinatal management and infant nutritional care. Second, we did not include detailed data on delivery room resuscitation, use of surfactant, caffeine and diuretics, actual enteral and parenteral nutrition, and fluid intake in the first week. Third, we did not collect maternal infection data. Finally, our study focused solely on the short-term hospitalization outcome, necessitating long-term follow-up studies to evaluate prognosis and BPD-associated growth and neurodevelopment among VPIs.
In conclusion, this study identifies the potential modifiable risk factors for sBPD among VPIs with BW of <1500 grams in China. The results suggest that shortening the duration of invasive mechanical ventilation, decreasing blood transfusion frequency, administering aggressive treatment for hsPDA and NI, and employing early enteral nutrition and active nutritional strategies might be useful strategies for prevention and treatment of moderate-to-severe BPD. Further randomized prospective trials with more participants are required to elucidate the benefits of these strategies.
Acknowledgment
The authors gratefully acknowledge Medjaden Inc. (https://en.medjaden.com/) for English language editing.
Footnotes
Disclosure. This study was supported by the Natural Science Foundation of Xiamen, China (20221303) and Clinical Key Specialty of Fujian Province (specialty in neonatology), China.
- Received January 8, 2024.
- Accepted February 16, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.