


ABSTRACT
Echinococcosis is a parasitic infection that is distributed worldwide. Its clinical presentation depends on the size and location of the cyst. A 7-year-old was found with a superimposed infected pulmonary hydatid cyst that was initially misdiagnosed as complicated pneumonia. Our case underscores the challenges of diagnosing and managing echinococcosis, emphasizes the need for a high index of suspicion, and describes the disease’s ability to mimic other clinical entities.
Echinococcosis is a parasitic infection caused by tapeworms of the genus Echinococcus. It encompasses 2 distinct entities, cystic echinococcosis and alveolar echinococcosis, which are differentiated by the causative species Echinococcus granulosus and Echinococcus multicularis.1 The World Health Organization (WHO) has listed echinococcosis as a neglected disease and aims to control or eliminate it by 2050.2 It presents unique challenges due to the complexities associated with its diagnosis and management; in addition, it has the potential for metastasis akin to malignancy in nature given its high rate of recurrence post-treatment.1 We report a case in which the patient’s initial presentation was labeled as complicated pneumonia. Thus, the patient received a long course of antimicrobial therapy until a diagnosis of pulmonary echinococcosis (hydatid cyst) was obtained, which highlights the need for a high index of suspicion in echinococcosis diagnosis.
Case Report
A 7-year-old male with an unremarkable medical and surgical history presented initially with a week-long fever coupled with nocturnal cough and increased work of breathing. Other systemic reviews of the patient yielded unremarkable results. He was admitted to a local hospital in Al-Qurayyat, Saudi Arabia, where he received a 10-day course of ceftriaxone and vancomycin after being diagnosed with pneumonia. While the fever resolved, the patient’s persistent cough led to enhanced chest computed tomography (CT), which revealed complicated pneumonia. Given the CT findings, he was referred to King Fahad Medical City, Riyadh, Saudi Arabia. The patient continued to undergo antibiotic therapy for 2 more weeks.
Clinical findings
He remained afebrile but showed no improvement in his cough.
Diagnostic assessment
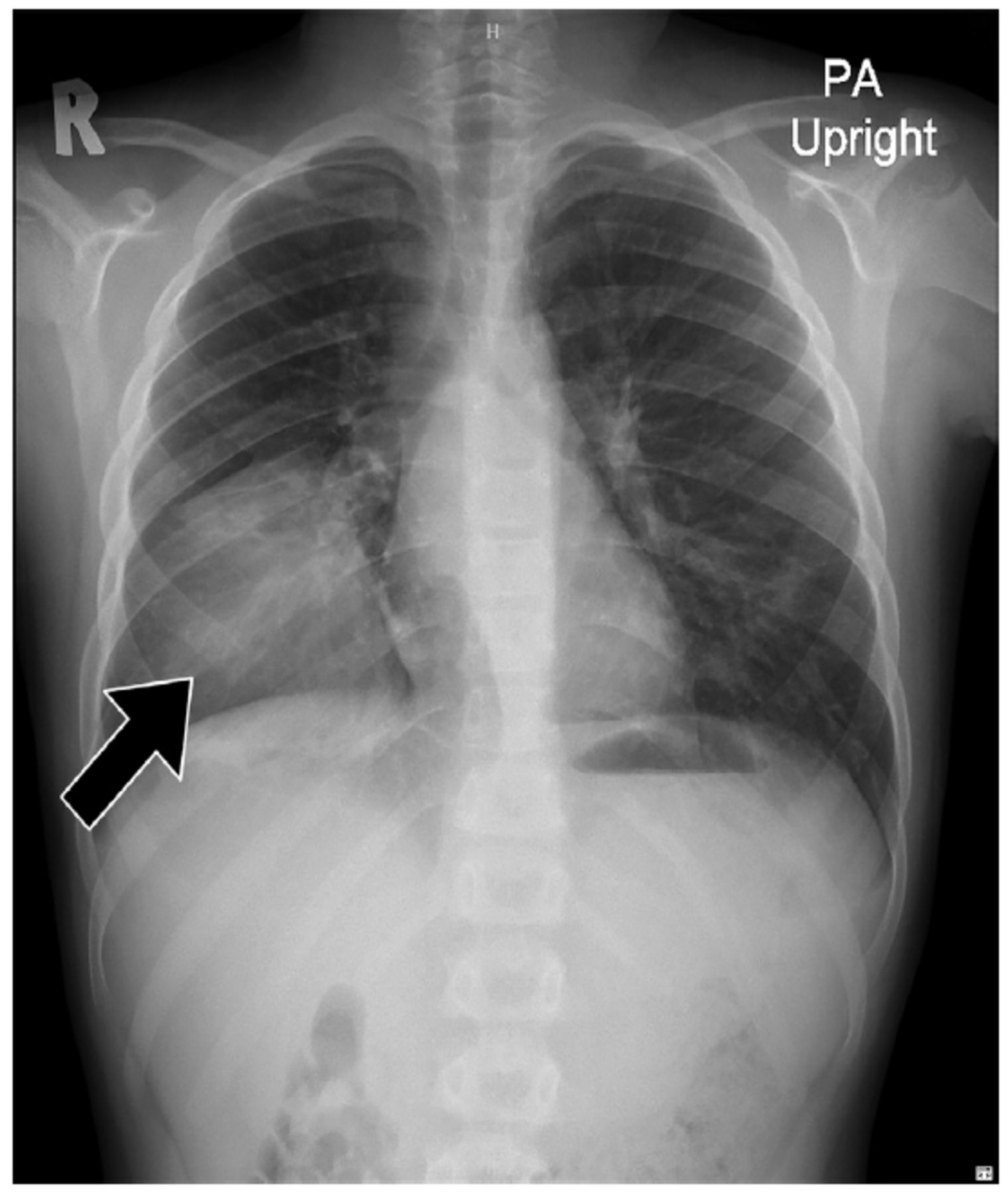
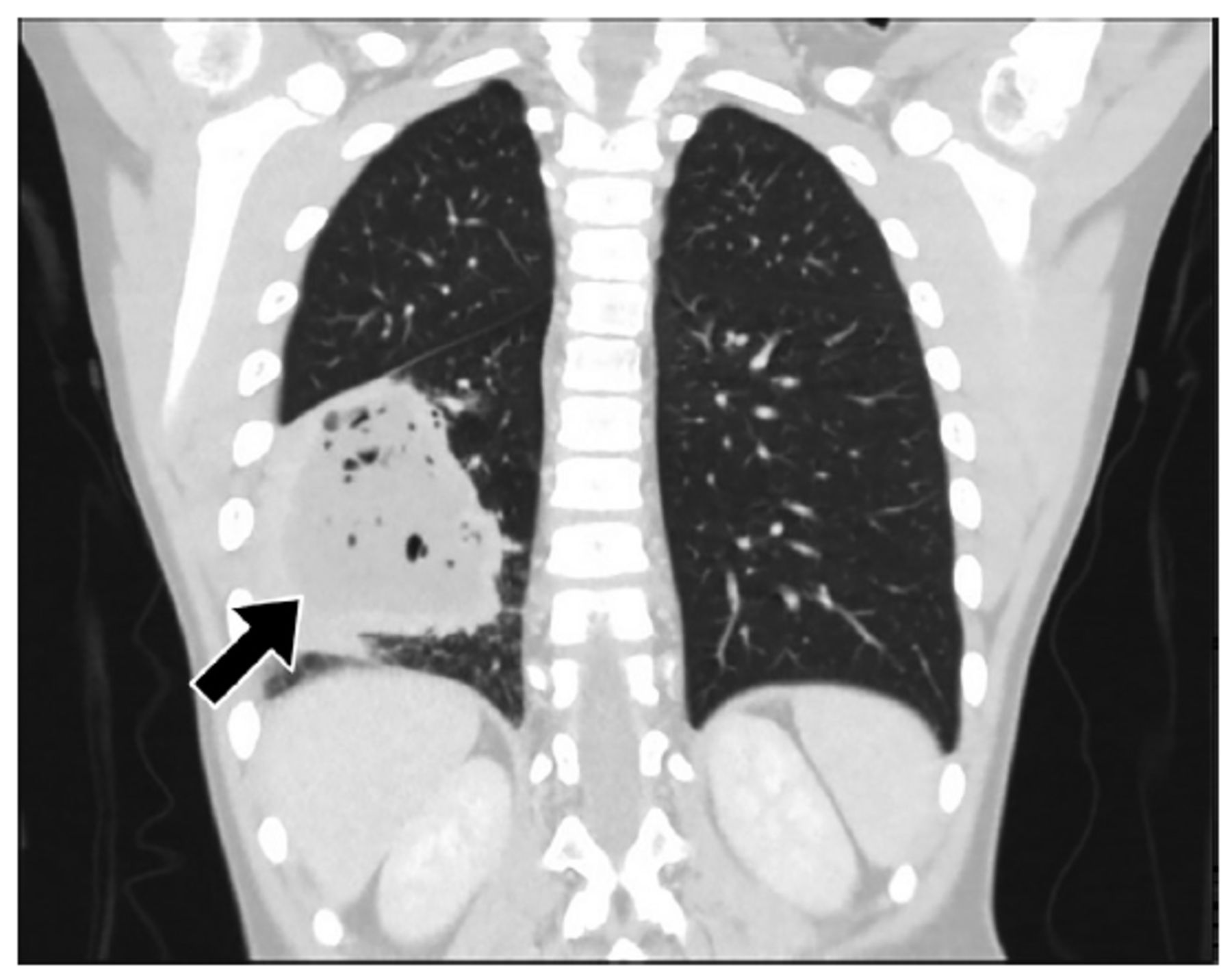
Laboratory results indicated white blood cell count within normal limits: 7.7 10*3/uL (4.3-11.3 *3/uL) of the white blood cells (34%) were neutrophils, 50% were lymphocytes, and 4% were eosinophils. A chest X-ray revealed well-defined rounded consolidation on the lower lobe (Figure 1). He was discharged on trial of bronchial asthma management with no noted benefit; and a repeat CT in an outpatient continued to suggest a diagnosis of complicated pneumonia with liquefied necrosis (Figure 2). A second opinion was sought, considering the positive exposure history to sheep and dogs, chest X-ray findings, and eosinophilia. Suspicion of hydatid disease was raised, and serology for Echinococcus antibody tests returned positive results - 7.2 (index blew 0.9 is considered negative) to support the diagnosis.

- Postero-anterior chest x-ray demonstrating the right lower lobe opacity.

- Enhanced chest computed tomography by intravenous contrast illustrate a Lower lung lobe cavitary lesion with central necrosis filed with fluid and pocket of air surrounded by a thick enhanced wall.
Therapeutic intervention
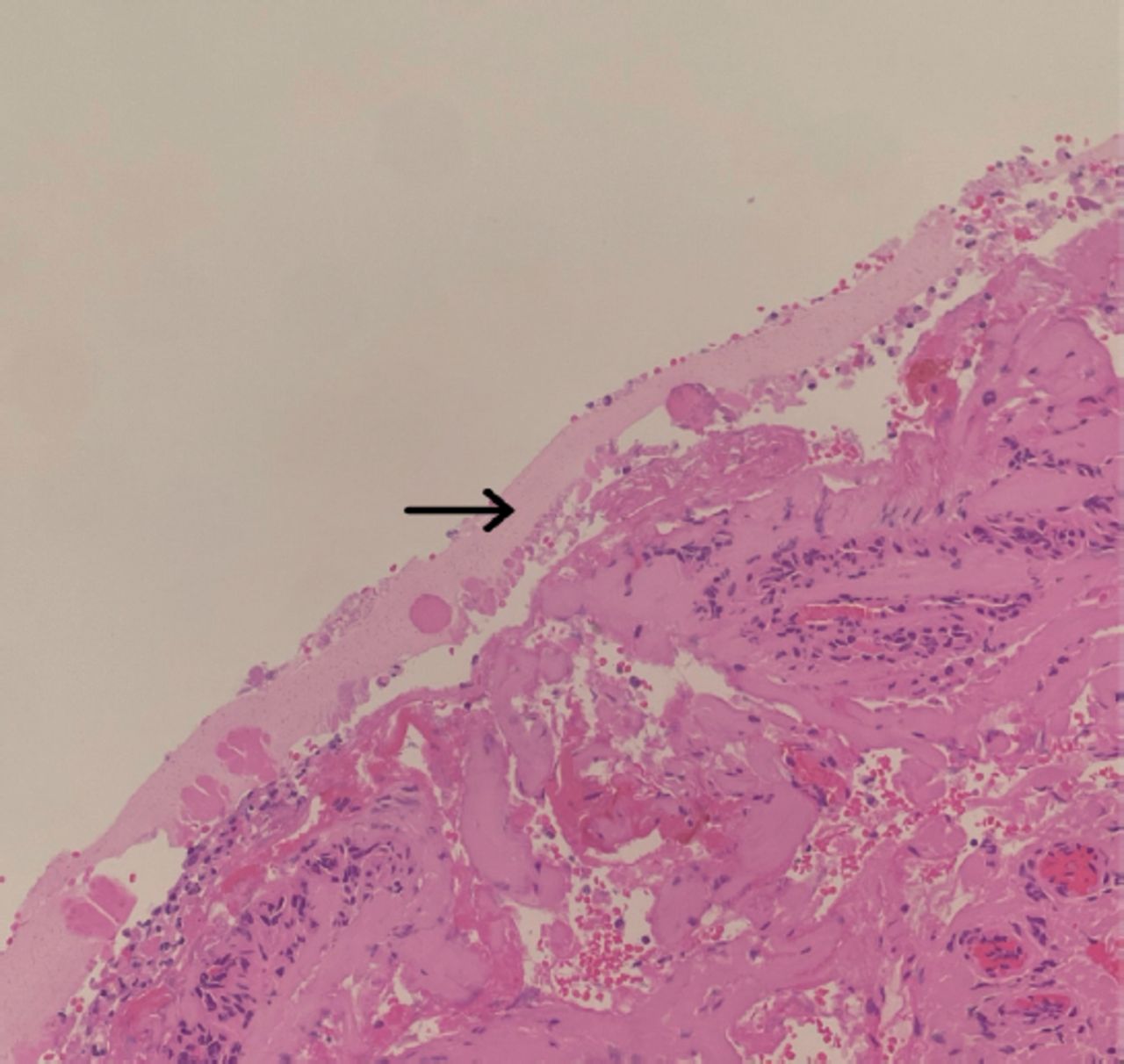
The patient was administered albendazole, followed by open thoracotomy and lobectomy. Histopathology confirmed the diagnosis of pulmonary echinococcosis, by demonstrating the cysts’ outer acellular laminated membrane (Figure 3). After resection, the patient continued with albendazole therapy.

- Grocott methamine silver stained histopathology section shows the characteristic Laminated membrane of the hydatid cyst (black arrow).
Follow-up and outcomes
He was followed in the clinic, and after 2 months, all his symptoms completely resolved.
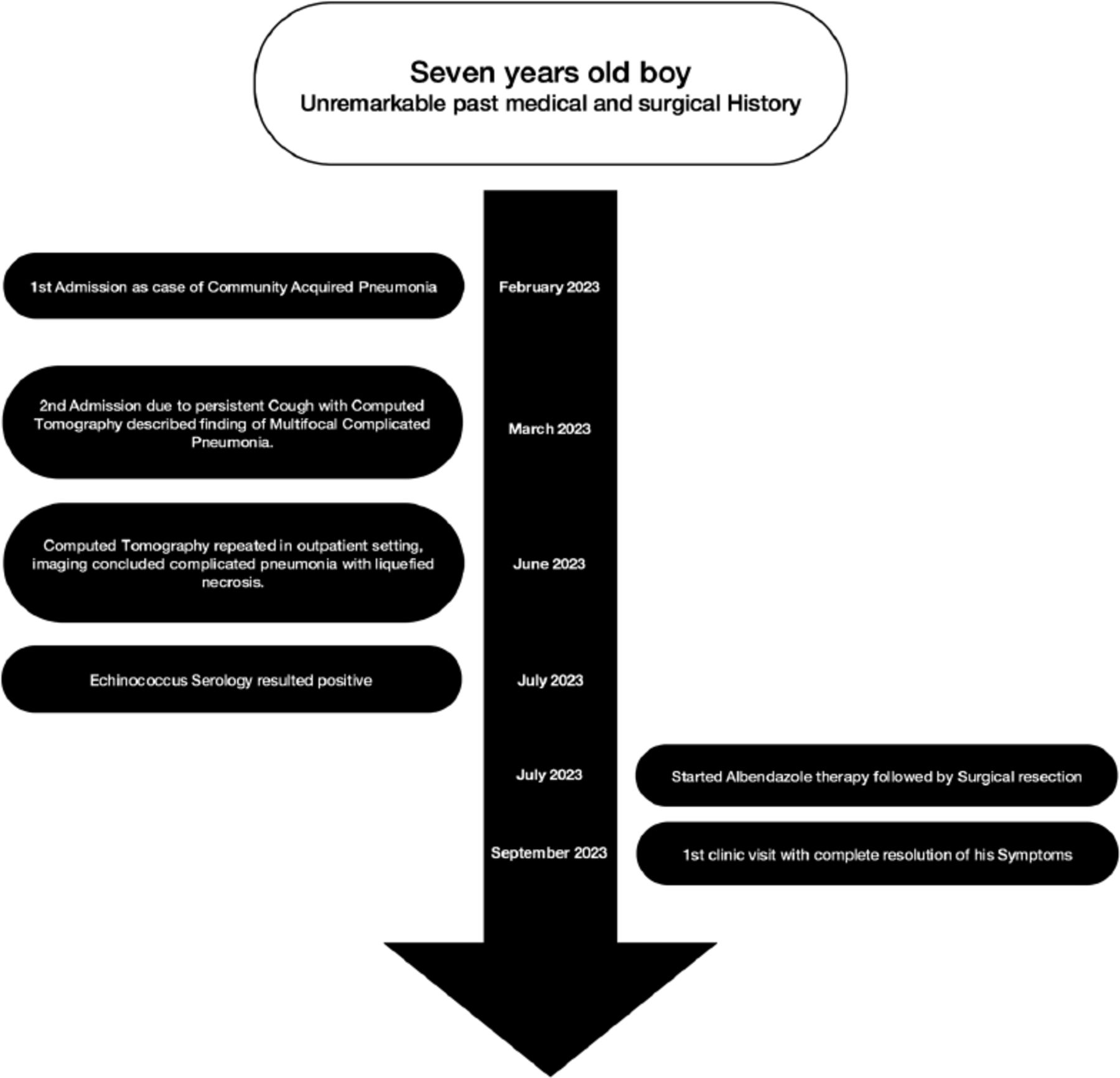
The key clinical findings and follow up for this patient are summarized in Figure 4.

- Flowchart visualizing patient timeline.
Discussion
Echinococcosis remains a significant public health obstacle around the world despite preventive efforts.2 The parasitic life cycle involves predator - prey interactions; the predator (such as dogs) act as definitive host to an adult worm, which produces eggs in the host’s intestine, which is passed into the feces. When the eggs are ingested by the intermediate host (such as sheep), they hatch and pass into the bloodstream through the portal and lymphatic vessels, where they settle into the body organs. Humans acquire the cestode though the consumption of infected animal meat, or (rarely) by direct ingestion of the eggs.1
Echinococcosis is an endemic disease in Western Saudi Arabia and its surrounding countries.3 Meat screenings revealed a disturbingly high rate of echinococcosis in slaughtered animals. Fawzia et al,4 who hail from the western region of Saudi Arabia, reported a prevalence of 69% for hydatidosis in slaughtered sheep and 19% in goats. Another study carried out in Al Baha, Southwest Saudi Arabia, revealed a rate of 32% for echinococcosis in camels and 12% in sheep.5 These rates combined with the prevailing herding lifestyle and socio-cultural shifts in pet ownership, particularly dogs likely contribute to significant epidemiological changes in Saudi Arabia.
The disease often remains asymptomatic for extended periods. Its symptoms are the result of space occupation, and clinical presentation varies depending on the site affected, making diagnosis challenging.1 Various cases in the literature highlight delayed or misdiagnosed cases due to unusual cyst locations or superimposed infections, complicating the clinical picture. One of the earliest recorded cases of echinococcosis occurred in 1987 and depicted an adult female with an echinococcal hepatic cyst communicating with a similar cyst in the lung, presenting as pulmonary consolidation and pleural effusion. Cultures of both pleural fluid and cyst content yielded substantial growth of Streptococcus milleri and Haemophilus parainfluenza.6 Lawandi et al7 reported a case involving a 9-year-old female initially diagnosed with a bacterial lung abscess. However, an elevation in eosinophil count led to CT imaging, which led to the diagnosis of ruptured hydatid cysts. Bhat et al8 described a 4-year-old female whose abdominal CT scan revealed a cystic mass related to the head and body of the pancreas. Initially labeled a choledochal cyst, the diagnosis of echinococcosis was only confirmed following surgical resection.
Current guidance in management is an effort endorsed by the WHO’s Informal Working Group on echinococcosis with the latest update published in 2009. The total surgical resection of the cyst is the recommended approach, but medical management is accepted in select cases. Benzimidazole remains the only anti-infective medication that halts the growth of the cestode; as such, it is used to reduce cyst size, decrease infectivity, and prevent relapse. The choice of treatment strategy should be based on a case-by-case approach guided by multidisciplinary teams.9 Efforts are in progress to update and develop existing guidance in management as part of the WHO’s plan to control or eliminate echinococcosis by 2050.2
Recent literature proposes a combination of benzimidazole plus praziquantel, Velasco-Tirado et al10 published a meta-analysis in 2018 in which they concluded that there is a potential benefit in combined treatment with albendazole plus praziquantel compared to albendazole monotherapy in reducing the risk of disease recurrence, seeding of infection in case of cyst rupture, and the formation of secondary cysts. However, further studies are needed to solidify these recommendations.
There is a beacon of hope in that disease elimination is endorsed by WHO, whose plans to control or eliminate echinococcosis by 2050 include ongoing efforts to develop vaccines targeting intermediate hosts, aiming to interrupt the chain of transmission and halt the spread of the cestode to humans.2
In conclusion, this case emphasizes the ability of echinococcosis to mimic other clinical entities, including common diseases such as pneumonia, which highlights the need to consider echinococcosis in pediatric patients presenting with respiratory symptoms, particularly in endemic regions. Early diagnosis and a multidisciplinary approach to management are crucial, given the disease’s potential for recurrence. Literature on echinococcosis is still lacking, which highlights the need for continued research and collaboration in the field of parasitology.
Acknowledgment
The authors would like to thank Scribendi Inc. (https://www.scribendi.com/) for the English language editing.
Footnotes
Disclosure.Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 24, 2024.
- Accepted March 24, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.