


Abstract
Objectives: To analyze the relationship between chronically ill patients’ behaviors in acquiring and verifying health information from a digital environment with health literacy and patient empowerment using a structural equation modeling approach.
Methods: This study was carried out in a public hospital in Turkey between February and May 2023. The study consisted of 365 participants and used descriptive and correlation-based designs for statistical analyses. It also executed computations for descriptive statistics and correlations to carry out a path analysis to assess model fitness and to identify direct and indirect effects.
Results: This study identified that Web 1.0 and health information acquisition and digital verification variables statistically and significantly affected access to information, understanding information, appraisal (valuing)/evaluation, and application/use variables. The study also found that access to information variables was statistically significant on identity/identicalness, self-control, decision-making, and recognition and comprehension. The tested model fit the data well and adequately explained the direct effects of the variables.
Conclusion: The study concluded by suggestively improving the chronically ill patients’ media or digital literacy levels through special training to stimulate their internet use effectively.
Nowadays, digital environments accessed for health information acquisition provide individuals with significant opportunities thanks to advancing technology and escalating internet access.1,2 In the digital world, health information search is actualize for a variety of causes, including information acquisition regarding health issues, coping with health-related concerns, reducing uncertainty (disambiguation), making healthy decisions, and requesting personal health information.3,4 However, studies reportedly indicated that much as the digital environment is typically a critical source for health information acquisition, the extensive information diversity raises the concern of finding relevant information.5,6 Additionally, many internet users who search for health information cannot properly evaluate the quality of websites, are open to misinformation, cannot fully comprehend the acquired information, and fail to contextualize information correctly.7
Studies revealed that health literacy plays a decisive role in health information acquisition, analysis, and attainment of the cognitive and social skills that enable individuals to access proper healthcare information on social platforms.8 A high level of health literacy fosters individuals’ acquisition and figure outing of health-related information in the digital environment, as well as significantly influence their healthy lifestyle, well-being, level of utilizing health services, patient satisfaction, level of adherence to treatment, reasonable drug use, and patient safety and life quality.9-11
Information acquisition in digital settings undeniably improves personal empowerment by offering diverse health services, such as advisory, education, and follow-up.12 Individuals who access the digital environment for health information acquisition will expectedly cooperate more with health professionals, improve their decision-making skills, use health services better, and thus feel more empowered.13 However, some other studies emphasized that as patients become empowered, their adherence to the doctor may be adversely affected, and they may feel exhausted, confused, or misdirected by the information acquired from digital platforms.14
Several studies reported that information acquisition from digital platforms is necessary and effective for patients to adopt behavioral changes and successfully manage the disease to prevent chronic illnesses.15-17 The literature also revealed that health information acquisition from digital media largely favorably impacted chronic illness management - despite a few contradictory citations.17,18 Therefore, the absence of any study in the literature assessing the relationship between the variables of acquiring and verifying health information in the digital environment, health literacy, and patient empowerment necessitated carrying out the current research. The findings of this study will anticipatingly make a substantial contribution to the available literature. This study aimed to identify the effect of digital health information acquisition and verification behaviors of chronically ill patients on health literacy and patient empowerment and assess the relationship between the relevant outcomes using a path analysis.

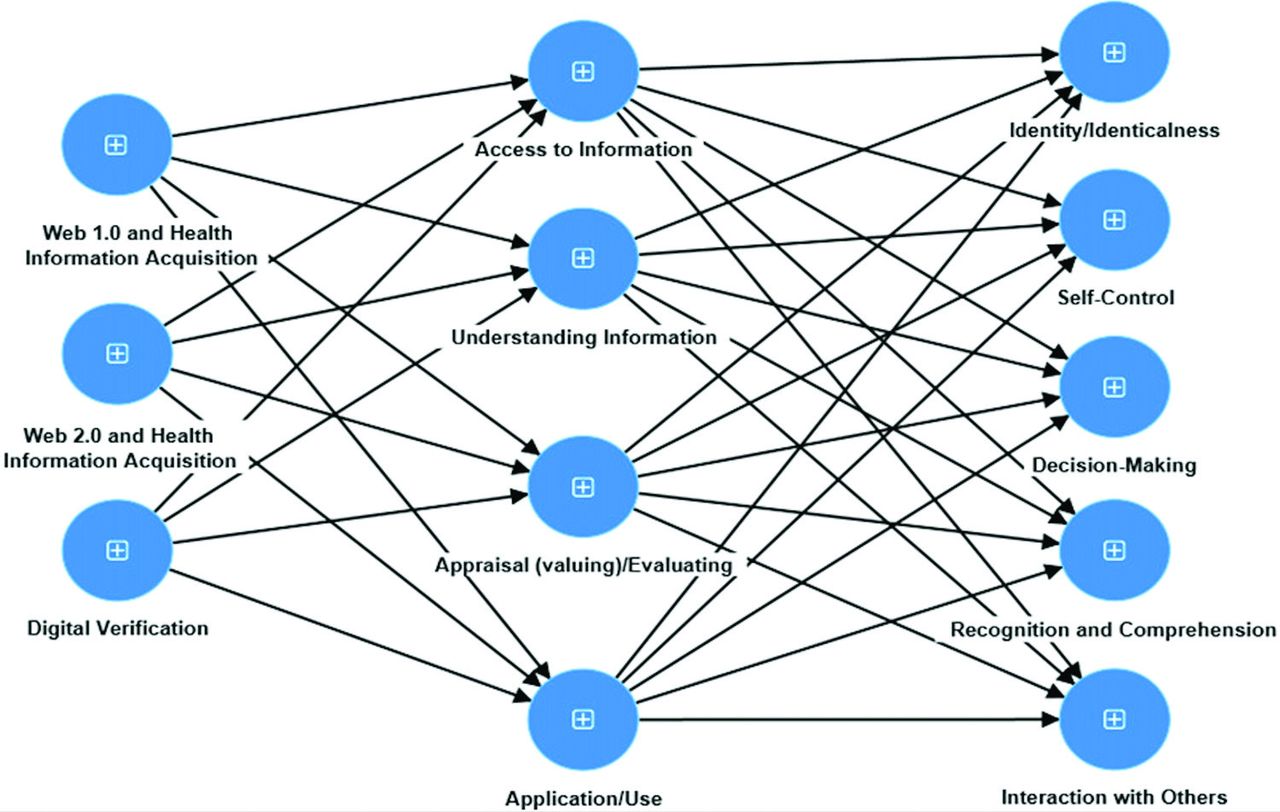
- Structural modelling of path diagram.
Methods
The study is in descriptive and correlational design. Using a set population sampling formula, the sample size calculator program computed the population size as 365 persons, with a 95% confidence interval and a 5% margin of error.
The study population consisted of patients who refered to the internal medicine outpatient clinic because of their chronic disease, between February and May 2023. The convenience sampling method was utilized for sample selection in the research. The inclusion criteria for the study are: voluntary participation, a chronic illness, and no communication problems. Those below the age of 18 and those who answered the questions incompletely were excluded from the study.
All procedures established for studies including human participants were in accordance with the 1964 Declaration of Helsinki. The ethical approval for this study has been adopted from the Faculty of Medicine, Sakarya University, Sakarya, Turkey (date: 15.02.2022, no.: 47). In addition, written consent was obtained from the participants in the study.
The researchers collected the study data through face-to-face questionnaires. Responding to the questionnaires took approximately 20 minutes. The researchers typically used a personal information form, the behavior scale for health information acquisition and verification in digital setting, patient empowerment scale, and health literacy scale to collect the study data.
The personal information form developed by the literature review involved 10 queries, including the participant’s gender, age, marital status, educational status, and economic status. This form also inquired on patients’ chronic illnesses, where they typically got information regarding their illnesses, which digital media utilized the most for information acquisition, how much time patients spent on the Internet during the daytime, and whether they would consider attending online training.
As developed by Çömlekçiet al,2 Scale for Health Information Acquisition and Verification consisted of 10 items and 3 sub-dimensions. While the “Web 1.0 and health information acquisition” sub-dimension describes the cases in that users prefer non-interactive environments instead of social media platforms while doing web-based health information searches. The “Web 2.0 and digital health information acquisition” sub-dimension also expresses the contexts in which users access health information through social media platforms such as Instagram, YouTube, or Twitter. However, the “digital verification” sub-dimension clarifies the methodologies that users execute to verify the acquired health information from digital media. The scale was a 5-point Likert-type and took the averages of the relevant items to calculate the scale values. Accordingly, higher scores on the scale signified an increase in participants’ digital health information acquisition and verification behaviors.
In patient empowerment scale, the lowest score from the 5-point Likert scale is 37, while the highest score is 185. This scale consisted of 5 sub-dimensions: identity/identicalness, self-control, decision-making, recognition and comprehension, and interaction with others.19
Health literacy scale consisted of 25 components and four sub-dimensions, containing access to information, understanding information, appraisal/evaluation, and application/use. The minimum score that can be obtained from the scale is 25, while the maximum score that can be obtained is 125.20
Statistical analysis
The study used the Statistical Package for the Social Sciences, version 25.0 (IBM Corp., Armonk, NY, USA) for Windows and Smart PLS 3 program to analyze the study data.21 The data were analyzed quantitatively. The study calculated the construct reliability (composite reliability [CR]) value for composite reliability, the average variance value (average variance extracted [AVE]) explained for convergent validity, and the Fornell-Larcker criterion, Heterotrait-Monotrait (HTMT) ratio values for discriminant validity within the scope of the measurement model.21
The study also used the following procedure for data analysis: as initially carrying out a confirmatory factor analysis to evaluate the reliability and validity of the study instrument, the study utilized a Smart PLS path model analysis to test the 3 hypotheses. The outcomes of this test would explicitly indicate the presence of significant correlations between the independent and dependent variables. Subsequently, the R2 value was used as an indicator for the overall predictive power of the model based on the following values: 0.67 as substantial, 0.33 as moderate, and 0.19 as weak.22,23 Then, the f2 value was used as a scale to set the effect size of predicting variables in the model based on the following values: 0.35 as large, 0.15 as medium, and 0.02 as weak.23 Finally, if the Q2 value for a dependent variable was higher than zero, it indicated that the model had predictive relevance. The statistical significance level was considered 2-sided and 5%.
Results
The average age of the study participants was 58.80±13.50 years. Approximately 55.6% of the participants were women, 80% were married, 52.9% received primary school education or below, and 69% retained a moderate economic status. Analysis of the participants’ pre-existing illness conditions revealed that 47.1% had hypertension, 60% had diabetes, 12.1% had chronic obstructive respiratory disease (COPD), and 3% had cancer. While almost 77.3% of the participants primarily acquired their illness-related information from healthcare professionals, 46.3% preferred to use the phone for information acquisition from the digital environment. Furthermore, approximately 77.1% of the participants expressed that they spent 0-2 hours of daytime on the internet, and 83% of the participants demanded that face-to-face education is much better than receiving online education.
Structural modelling of path diagram (Figure 1) demonstrates whether “health literacy” is a mediating variable on the way from “health information acquisition and verification in digital environment” to “patient empowerment” for chronically ill patients.
Table 1 displays the reliability and validity data for the variables within the context of the measure model. The Cronbach’s alpha value for all constructs was over 0.60 (between 0.721-0.930). Cronbach Alpha and rho_A values greater than 0.60 indicated that the scales were dependable, and the internal consistency of the variable utilized in the study was satisfactory.26 Additionally, all factor loads were higher than 0.4, and the CR values for all constructs were higher than 0.7 (ranging from 0.745-0.930) and is higher than its respective AVE. This data suggested satisfactory construct reliability and convergent validity. The AVEs were higher than 0.5 for all constructs.
- Reliability results of the variables related to the research model.
As presented in Table 2, the correlation coefficients for the variables were lower than the square root of the AVE values, indicating that the Fornell-Larcker criteria was satisfied. The analysis outcomes also disclosed that the HTMT values were below the threshold (<0.90). Therefore, based on the findings in Table 3, it is possible to finalize that the divergent validity was satisfied.
- Fornell-Larcker criterion analysis and Heterotrait-Monotrait ratio.
- Model analysis results.
The model analysis results in Table 3 and Figure 1 revealed that the ‘Web 1.0 and health information acquisition’ and ‘digital verification’ variables affected the ‘access to information’ variable statistically and significantly (p<0.05). Considering the explanation ratio of the model. However, the ‘Web 1.0 and health information acquisition’ and ‘digital verification’ accounted for 27.2% of the variation in the ‘access to information.’ Furthermore, the ‘Web 1.0 and health information acquisition’ variable statistically and significantly affected the ‘understanding information’ and ‘appraisal/evaluation’ variables (p<0.05). The explanation rates of the model for these 2 variables were 27.2% and 29.1%. Correspondingly, the ‘Web 1.0 and health information acquisition,’ ‘Web 2.0 and health information acquisition,’ and ‘digital verification’ had a statistically significant effect on the ‘application/use’ (p<0.05). These 3 variables of the model, however, explained 29% of the variation in the ‘application/use’ variable.
The findings also demonstrated that the ‘access to information’ had a statistically significant effect on the ‘identity/identicalness’ and ‘self-control’ (p<0.05), and the ‘access to information’ variable explained 66.8% and 73.1% of the variations in ‘identity/identicalness’ and ‘self-control’ variables.
The study further identified that the ‘access to information’ and ‘appraisal/evaluation’ affected the ‘decision-making’ statistically and significantly (p<0.05). considering the explanation ratio of the model, the ‘access to information’ and ‘appraisal/evaluation’ variables accounted for 73.6% of the variation in the ‘decision-making’ variable.
Finally, the ‘access to information’ and ‘application/use’ had a statistically significant effect on the ‘recognition and comprehension’ (p<0.05), and accordingly, these 2 variables explained 70.3% of the variation in the ‘recognition and comprehension’ variable. The analysis outcomes also exposed that the ‘access to information’ statistically and significantly affected the ‘interaction with others’ (p<0.05). Considering the explanation ratio, however, the ‘access to information’ variable accounted for 52.8% of the variation in the ‘interaction with others’ variable.
Discussion
The increment of digital communication tools in social life has diversified individuals’ information sources and improved their access to information. Since the subject is health-related information, the role of internet-based sources and social networks has gradually increased. The vast coverage of health-related information and its high level of anonymization has resulted in individuals adopting behaviors of searching out health information through online platforms.3 Yet, the diversified and increased information resources and facilitated information access have diminished individuals’ levels of concern and improved their self-reliance. At this point, health literacy is crucial to making it easier for individuals to access reliable health information on social media settings and to acquire and analyze it.18 Studies have reportedly indicated that a high degree of health literacy accelerates the processes of reading and understanding health-related information from digital sources.9 Advanced health literacy also facilitates individuals accessing and recognizing health-related resources, enabling them to protect and improve their health statuses. Therefore, using a structural equation model, this study revealed the relationship between health information acquisition and verification behaviors in the digital environment, health literacy, and patient empowerment.
The current study also determined that the health information acquisition behaviors through web portals without using social media platforms significantly and positively affected all sub-dimensions of the health literacy scale. Unquestionably, internet usage to search for and acquire information raises the literacy level of individuals (due to the diversity of information sources available in digital settings) and gives them search opportunities before making health-related decisions.24 In a study carried out in Nigeria found that the behavior of seeking for health information on the internet is among the determiners of health literacy.25 Another study with university students reportedly used the logistic regression analysis and identified the relationship between online health information-searching behaviors and health literacy variables. Correspondingly, Lee et al26 and Estacio et al27 also found comparable results in their search. As a result, it is viable to infer from the literature that the digital platforms enabling individuals to access information positively influence their personal decisions and behaviors and public health-related concerns. Furthermore, improving health literacy (especially for chronically ill patients) significantly contributes to disease processes, including diagnosis, treatment, and management.28
Digital verification behavior refers to users’ testing the relevancy of health information acquired from digital media using various methods.2 Yet, digital platforms are the settings where people may freely post and share whatever they wish, and personal and corporate comments may spread readily, especially on social media, with a limited verification process. Verifying the information available on the internet is critical to prohibit the rapid spread of false or unconfirmed information.29 This study, in this context, revealed that the digital verification practices of the participants increasingly influenced their behavior of applying or using health-related information, a sub-dimension of the health literacy scale. A research carried out with university students reported a linear relationship between students’ digital verification behaviors and their interactive health literacy.16 Correspondingly, Özen et al30 also emphasized that the verification process of the information reliability acquired by health professionals from the internet or other digital platforms would positively affect individuals’ health behaviors. Therefore, it is essential for health promotion to identify which platforms individuals utilize to access health information and to what content and in what forms they verify the relevance of the data acquired.
The current study found that the access to information sub-dimension of the health literacy scale substantially influences all sub-dimensions related to the patient empowerment scale. The term ‘access to information’ refers to the practices, including information gathering, data scanning, and classification, which individuals follow to access relevant information. The era in which we live is entitled the “information age,” accumulating information at an exceedingly rapid rate. Digital environs provide great convenience in adapting to this incredible speed. Digital platforms also enable chronically ill patients to access and use health-related information resources efficiently, express their individual preferences by fostering their self-efficacy, control, and competence skills, participate effectively in decision-making processes, access the resources they need, and develop strong relationships with others. As a result, these practices potentially help them improve their quality of life. In this context, Mano et al31 reported that telehealth and social media in accessing information and effective communication with physitians positively influence patient empowerment among chronically ill patients. They further indicated that especially digital platforms are frequently used by both patients and physicians as they serve prompt access to information. Jiang et al32 also stated that internet use for accessing health-related information is highly effective for patient empowerment based on their conclusions from hierarchical regression analysis. Some studies added to the literature, on the other hand, highlighted the possibility of accessing health-related misinformation from unsecured websites or social media platforms, which could then spread to large masses, leading to adverse and poor health outcomes.7,33,34 Therefore, accessing proper information would ideally raise individuals’ health literacy level, enabling them to control their health conditions and better perceive and assess the issues related to their illnesses.
Study limitations
This study also carried out a cross-section data analysis. The relationships among the variables being correlational do not imply cause and effect. The study participants’ high average age, combined with more than half of them having only completed primary school or below education level, may be viewed as a barrier to their usage of the internet or digital tools. Despite these limitations, the study findings provided practical outcomes for health professionals focused on health literacy and patient empowerment topics among chronically ill individuals.
In conclusion, the current study findings revealed that the chronically ill patients’ behaviors of health information acquisition from web environs without using social media platforms have an increasing effect on all sub-dimensions of the health literacy scale. The ‘access to information’ sub-dimension of the health literacy scale also positively affected all the sub-dimensions of the patient empowerment scale. Besides, digital verification behavior significantly improved the ‘access to information’ and ‘application/use’ sub-dimensions under the health literacy scale.
It is, therefore, necessary to raise the health literacy level for chronically ill patients to properly manage their illnesses and achieve self-efficacy, control, and competence over their health concerns. However, ensuring the reliability of the digital settings used frequently for information acquisition is also critical in this process. In this sense, given the issue of misinformation regarding health concerns impacting the entire world, it is viable to recommend feeding patients with specialized training to advance their media or digital literacy skills and enable them to utilize the internet efficiently. Health practitioners should also facilitate health-protective and educational programs to allow individuals to make health-related decisions in the light of the correct information.
Acknowledgment
The authors gratefully acknowledge Blue Tower educational services (http://www.bluetoweredu.com/) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 23, 2024.
- Accepted May 15, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.