


Abstract
Objectives: To assess the association between chemotactic chemokine (C-C motif) ligand 5 (CCL5) -28C>G polymorphism and tuberculosis (TB) risk.
Methods: PubMed, Web of Science, and WanFang were searched up to April 2015 for eligible studies on CCL5 -28C>G polymorphism. Data was extracted, and pooled odd ratios (ORs) as well as 95% confidence intervals (95% CI) were calculated.
Results: Eight case-control studies were extracted from 8 articles on the polymorphism involving 1852 TB cases and 2068 controls. The results of meta-analysis showed that significant reduced risks were found for the polymorphism with the risk of TB in Asians and Arabs as follows: OR=0.12, 95% CI=0.06-0.26, p=0.000 for mutant homozygous (GG) versus wild-type homozygous (CC) for Asian descent, OR=0.14, 95% CI=0.07-0.28, p=0.000 for GG versus CC in the Arab descent.
Conclusion: Our findings demonstrated that CCL5 gene -28C>G polymorphism might be a protective factor for the development of TB.
Tuberculosis (TB) is one of the most important infectious causes of death worldwide.1 According to reports from the World Health Organization (WHO), more than 8.8 million new TB cases were reported in 2010, and 1.1 million patients died.2 Numerous studies showed that only one-third of the population exposed to Mycobacterium tuberculosis (M. tuberculosis) were infected asymptomatically, and less than 10% of them developed TB,3 indicating that the individuals had different susceptibility to TB. Although the underlying etiological mechanism of TB infection was still unclear, the host genetic gene is considered to be one of the reasons for the incidence of TB, and may be impact on the disease before the onset. In recent years, genetic variants, including Toll-like receptors-2,4 nucleotide-binding oligomerization domain 2,5 interleukin-12B,6 cytotoxic T-lymphocyte-associated protein 4,7 and so on, were demonstrated to be associated with TB susceptibility, while their roles in the incidence of TB were conflicting. Among various cytokines, the chemotactic chemokine (C-C motif)chemokine ligand 5 (CCL5), also called regulated upon activation and normal T cell expressed and secreted (RANTES), is an 8 kDa protein belonging to T-helper type 1, and produced by macrophages in the presence of infection with M. tuberculosis. It could not only mediate migration, activation of T-cells and macrophages,8 but also play a major role in the antimycobacterial immune responses by recruiting mononuclear cells to the site of infection.9 At present, several single nucleotide polymorphisms (SNPs) in the CCL5 gene have been found. For example, -403G>A, -28C>G SNPs have been identified in the promoter of CCL5, which may regulate the transcriptional activity of CCL5.10,11 In 1.1 T/C (allele T mutate into allele C), a functionally important polymorphism located in the first intron of CCL5 was found to regulate the transcription level of the gene by differentially binding to alternative forms of nuclear proteins.12 Several studies have reported the association between CCL5 polymorphisms and TB, the results were inconsistent due to limited sample sizes and different study populations. Therefore, we performed a systematic review and meta-analysis in this article to summarize the associations between CCL5 -28C>G gene polymorphism and TB susceptibility.
Methods
We carried out this systematic review and meta-analysis in accordance with the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions,13 and the results were reported in accordance with the PRISMA Statement.14
A literature research was conducted by using PubMed and Web of Science, and WanFang up to April 9, 2015. Relevant studies were identified by searching from following terms: [‘CCL5 OR RANTES gene’] AND [‘genetic polymorphism OR polymorphisms OR SNP’] AND [‘tuberculosis OR TB’]. Potentially relevant genetic association studies were evaluated by examining their titles and abstracts,15 and all published studies matching the selected eligible criteria were retrieved and incorporated in this study. The study protocol was approved by the Ethical and Science Committee of the Ministry of Health.
Selection criteria
Studies were selected for this meta-analysis if they met the following criteria: 1) studies that evaluated the association between the CCL5 -28C>G polymorphism and TB, 2) a case-control study design, 3) recruited pathologically confirmed TB patients and TB free controls, and 4) had detailed genotype frequency of cases and controls or could be calculated from the article text. The exclusion criteria were 1) case-only study, case reports, and review articles, and 2) studies without the raw data of the genotype of TB15 (Figure 1).
The process for the screening of 8 potentially relevant studies included in the meta-analysis. CCL5 - chemotactic chemokine (C-C motif) ligand 5, TB - tuberculosis.
Data extraction
The 2 investigators independently extracted the data and reached a consensus for all items. If the 2 investigators generated different results, they checked the data again and discussed to come to an agreement. If they could not reach an agreement, an expert was invited to the discussion. Data extracted from the selected articles included the first author’s name, year of publication, country of origin, ethnicity, number of cases and controls, and minor allele frequency in the controls. Different ethnicity was categorized as Asian and Arab.
Statistical analysis
Before assessing the effects of CCL5 polymorphisms on the susceptibility to TB, we tested whether genotype frequencies of controls were in Hardy Weinberg Equilibrium (HWE) by using x2 test. We also quantified the effect of heterogeneity by I2 test. When a significant Q test (p<0.1) or I2 >50% indicated heterogeneity across studies, the random effects model was used, or the fixed effects model was used.16 The odds ratio (OR) and 95% confidence interval (CI) were employed to estimate the risk of TB with the CCL5 gene. A x2-test-based Q statistic test was performed to assess the between-study heterogeneity.17 Analysis of sensitivity was performed to evaluate the stability of the results. Finally, potential publication bias was investigated using Egger’s regression test.18 P<0.05 was regarded as statistically significant. Meta-analysis was performed by Review Manager 5.1 and Stata 12 (Stata Corporation, College Station, Texas, USA) software packages.
Results
Search results
The search strategy retrieved 12 potentially relevant studies. According to the inclusion criteria, 8 studies with full-text were included in this meta-analysis and 4 studies were excluded. The flow chart of the study selection is summarized in Figure 1. As shown in Table 1, there were 8 case-control studies with 1852 TB cases and 2068 controls concerning -28C>G polymorphism. As for the 3 ethnicities addressed, 5 studies focused on Asian populations,19-23 2 on Arab populations,24,25 and one on a Caucasian population.26 Because of the insufficient samples available for Caucasian groups, we have performed subgroup analysis in the Asian and Arab groups. In 2 studies,19,21 the distribution of the genotypes in the control group was not in HWE (p<0.05). Then, a sensitivity analysis was performed by excluding these studies from the analysis.
Characteristics of 8 potentially relevant studies included in the meta-analysis.
Associations between CCL5 -28C>G polymorphisms and TB
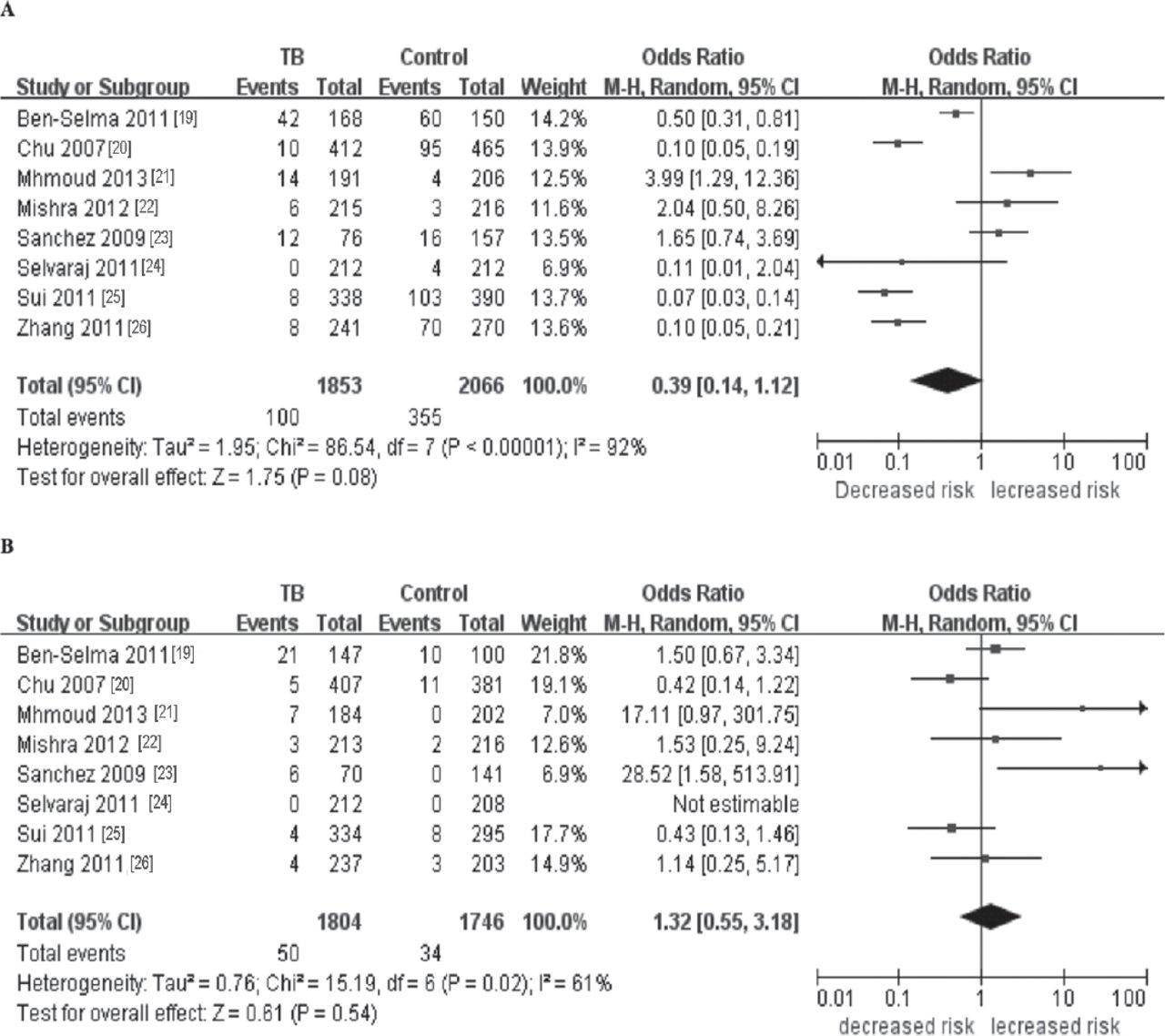
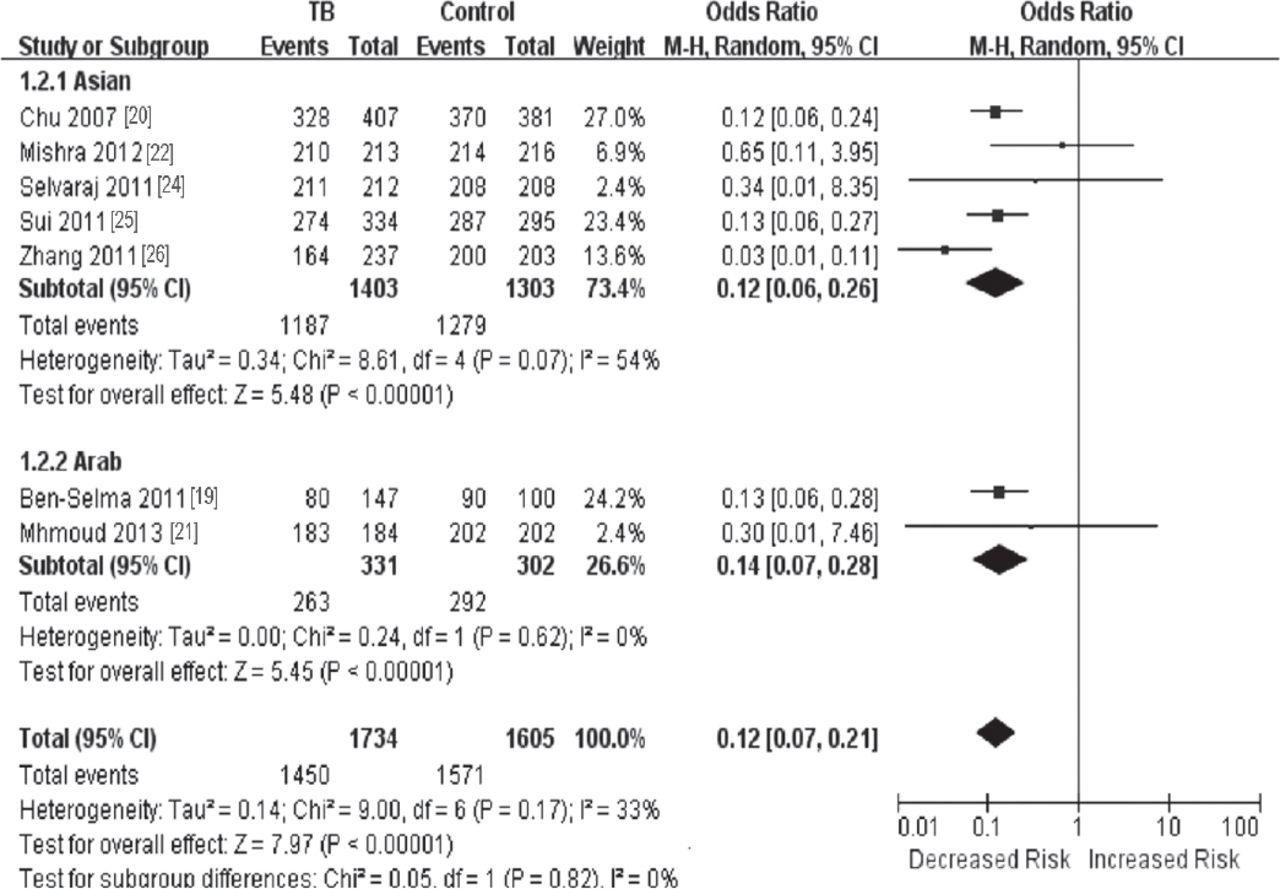
The analysis on CCL5 -28C>G polymorphism, qualified into 8 studies (Table 1), revealed that there was no difference in CCL5 -28C>G genotype distribution between TB patients and control populations (Table 2, Figure 2). To avoid the heterogeneity of ethnicity, we performed a subgroup analysis, reduced risk was found in the Asian descent (mutant homozygous [GG] versus CC: OR=0.12, 95% CI=0.06-0.26, p=0.000) and in the Arab descent (GG versus CC: OR=0.14, 95% CI=0.07-0.28, p=0.000) (Table 3, Figure 3). Sensitivity analysis was performed by sequential omission of individual studies. For analysis on -28C>G polymorphism, we examined the influence of these studies that were not in HWE on the pooled OR by repeating the meta-analysis while excluding each study. The results showed that the estimated pooled OR were not changed, indicating that our results were statistically robust. For the other polymorphisms, the significance of pooled OR in all individual analyses was not altered excessively by omitting any single study.
Pooled analysis for the associations between polymorphisms of CLL5 -28C>G and the risk of TB.
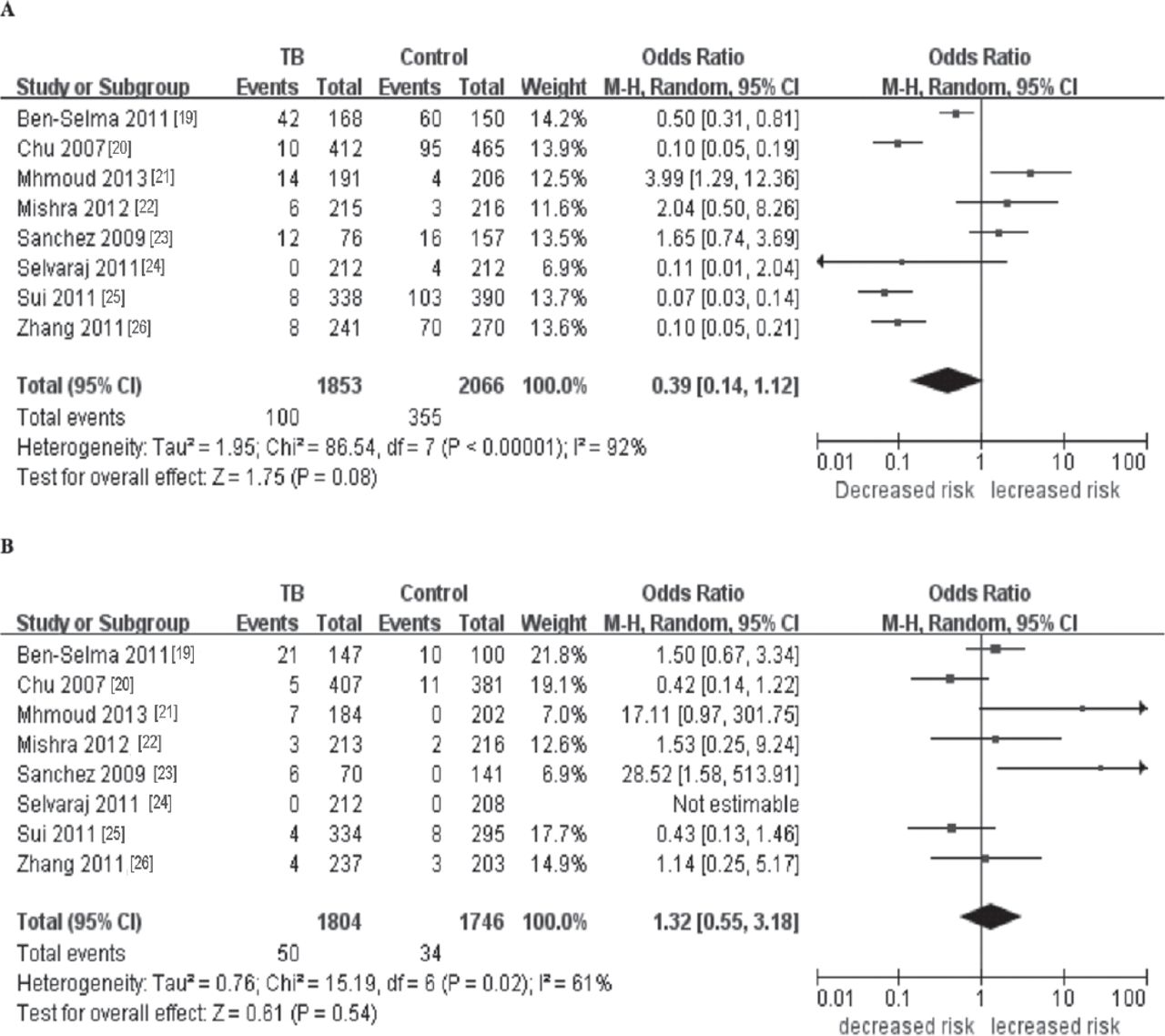
Meta-analysis of the association between CCL5 -28C>G polymorphism and susceptibility to TB. A) CG+GG versus CC. B) GG versus CC. CCL5 - chemotactic chemokine (C-C motif) ligand 5, TB - tuberculosis, CC - wild-type homozygous, GG - mutant homozygous, CG - mutant heterozygous
Subgroup analysis for the associations between the polymorphisms of CLL5 -28C>G and the risk of tuberculosis.
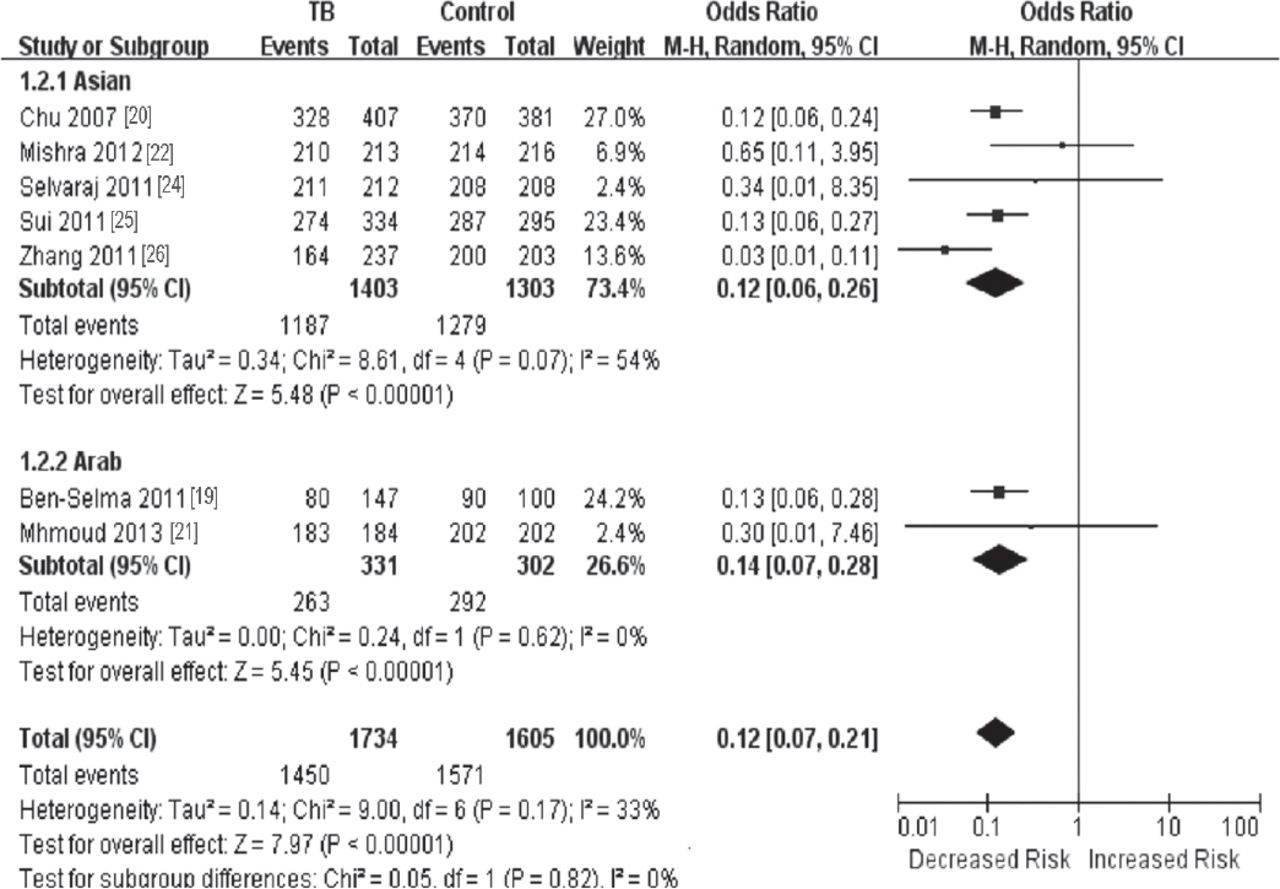
Subgroup analysis of CLL5 -28C>G polymorphism by ethnicity (GG vesus CC). TB - tuberculosis, 95% CI - 95% confidence interval, df - degrees of freedom, CCL5 - chemotactic chemokine (C-C motif) ligand 5, TB - tuberculosis M-H - Mantel Haenszel test
Test of heterogeneity
There was significant heterogeneity for overall comparisons (dominant model: p=0.000; heterozygote comparison: p=0.020; homozygote comparison: p=0.020; recessive model: p=0.010). In the subgroup analysis by ethnicity, results were similar in the Arab population. While in the Asian population, there was significant heterogeneity for minor allele (G versus C, p=0.040), but not for dominant comparison (mutant heterozygous [CG]+GG versus CC p=0.550), recessive comparison (GG versus CG+CC: p=0.990), heterozygote model comparison (CG versus CC: p=0.790) and homozygous model (GG versus CC: p=0.070) (Table 2).
Q-test and I2 statistics were employed to test the heterogeneity among the selected publications. Heterogeneity was observed in all of the models. Thus, when a significant Q test (p<0.1) or I2 >50% indicated heterogeneity across the studies, the random effects model was used, or else the fixed effects model was used (Tables 2 & 3).
Publication bias
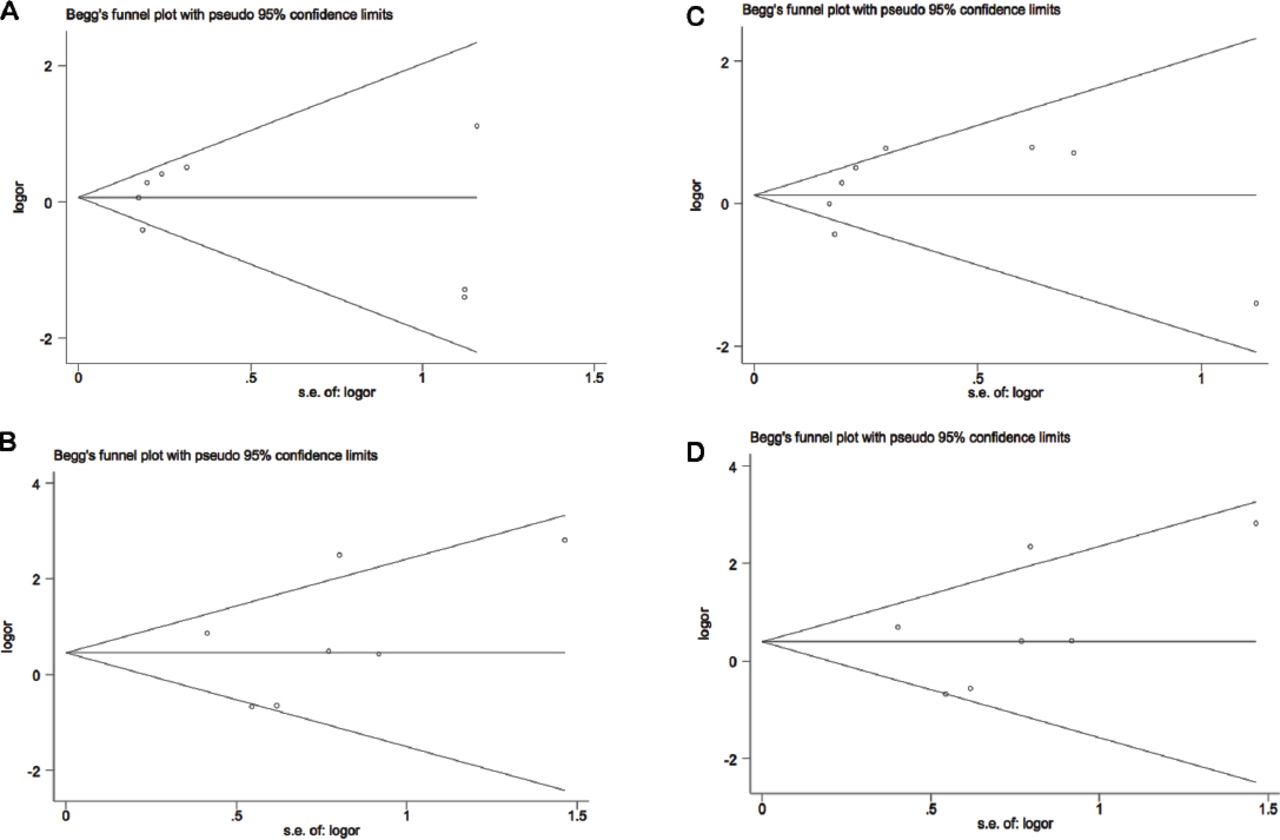
We used the Begg’s funnel plot and Egger’s test to address potential publication bias in the available literature. The publication bias of the meta-analysis on the association between CCL5 -28C>G polymorphism and susceptibility to TB was detected. The shape of funnel plots did not reveal any evidence of funnel plot asymmetry. Egger’s test also showed that there was no statistical significance for the evaluation of publication bias (P dominant model = 0.543, P heterozygote comparison = 0.887, P homozygote comparison = 0.441, P recessive model = 0.393) (Figure 4).

Begg’s funnel plot for publication bias. A) CG versus CC, B) GG versus CC, C) dominant model, and D) recessive model. Each point represents a separate study for the indicated association. logor - natural logarithm of OR. OR - odds ration, horizontal line - means effect size, s.e. of logor - standard error of logor, OR - odds ratio
Discussion
Tuberculosis has been one of the most important illnesses in the history of the world, it was never understood why only some people, and not others, developed to the disease. Recently, published genome-wide association studies (GWAS),27-29 demonstrated that host genetics strongly influence susceptibility to TB. Since it acts as a chemokine for T cells, monocytes/macrophages, eosinophils, and basophils, CCL5 was supposed to be a strong candidate for increasing susceptibility to TB. Chensue et al30 revealed that CCL5 promoted granuloma formation in M. tuberculosis-infected lungs in a mouse model. Sadek et al31 reported that CCL5 levels on bronchoalveolar lavage fluid in patients with active PTB increased nearly 8 times higher than that in the control group. According to a previous study,32 there is a significant association between the CCL5 -403 G>A polymorphism and increased risk of TB. Another study33 showed that genetic polymorphism -28C>G in CCL5 is not associated with increased TB risk. Although the exact molecular mechanism was still unclear, several polymorphisms in CCL5 have been reported previously,19-26 and the results were controversial.
Via a comprehensive meta-analysis, we evaluated the association of one common polymorphism in the CCL5 gene with the risk of TB. In this meta-analysis, we included a total of 8 case-control studies. The pooled results indicated that there was no association between CCL5 -28C>G polymorphism and TB under all models: allele contrast (G versus C), homozygote (GG versus CC), heterozygote (GC versus CC), dominant (GC+GG versus CC), and recessive (GC versus GG+CC) model. To avoid the heterogeneity of ethnicity, 8 eligible case-control studies were stratified into 2 subgroups (Asian and Arab). We found that CCL5 -28C>G GG genotype reduced the risk of TB in 2 subgroups by ethnicity analysis, which suggested a possible role of ethnic differences in genetic backgrounds and the environment they lived in. But because only 2 studies in an Arab population selected, these results should be interpreted with caution, and more studies are needed for further analysis in the future.
We attempted to minimize the likelihood of bias by developing a detailed protocol before initiating the study, some insurmountable limitations of this meta-analysis may affect the results and even the subsequent conclusions. First, there was a potential language bias, because the PubMed, Web of Science, and Wanfang digital database search engines were used to identify articles and to exclude articles written in languages other than English and Chinese. This might have prevented the researchers from accessing all relevant studies. Second, the number of published studies was not sufficiently large for a comprehensive analysis, and some studies with small size may not have enough statistical power to explore the real association. Third, the overall outcomes were based on individual unadjusted ORs; a more precise estimation should be adjusted by menstrual status, age, environmental, and other confounding factors. In spite of these limitations, our meta-analysis had several advantages. First, a substantial number of cases and controls were pooled from different studies, which significantly increased the statistical power of the analysis. Second, the quality of case-control studies included in current meta-analysis was satisfactory and met our inclusion criterion.
In summary, we have shown that the CCL5 -28C>G polymorphism was associated with the susceptibility to TB and the -28C>G GG genotype appeared to reduce the risk of TB in Asian and Arab population. However, large and well-designed studies are warranted to validate our findings. As TB-related genetic factors may interfere with non-genetic risk factors, such as environment, future studies should therefore be stratified accordingly. In addition, gene-gene and gene–environment interactions should also be investigated in the future.
Related Articles
Liu Q, Li W, Li D, Feng Y, Tao C. The association of interleukin-10 -1082, -819, -592 polymorphisms and tuberculosis risk. Saudi Med J 2015; 36: 407-417.
Somily AM, Naeem T, Habib HA, Sarwar MS, Kunimoto DY, Kambal AM. Changing epidemiology of tuberculosis detected by an 8-year retrospective laboratory study in a tertiary teaching hospital in central Saudi Arabia. Saudi Med J 2014; 35: 691-698.
Amoudy HA, Ebrahimi BH, Mustafa AS. Immune responses against Mycobacterium tuberculosis-specific proteins PE35 and CFP10 in mice immunized with recombinant Mycobacterium vaccae. Saudi Med J 2014; 35: 350-359.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 5, 2015.
- Accepted September 30, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}