


Abstract
Iatrogenic ileostomies are routinely placed during colorectal surgery for the diversion of intestinal contents to permit healing of the distal anastomosis prior to elective reversal. We present an interesting case of spontaneous closure of a diverting ileostomy without any adverse effects to the patient. A 65-year-old woman, positive for hereditary non-polyposis colorectal cancer type-I, with locally invasive cancer of the distal colon underwent en-bloc total colectomy, hysterectomy, and bilateral salpingoophorectomy with creation of a proximal loop ileostomy. The ostomy temporarily closed without reoperation at 10 weeks, after spontaneously reopening, it definitively closed, again without surgical intervention at 18 weeks following the original surgery. This rare phenomenon has occurred following variable colorectal pathology and is poorly understood, particularly in patients with aggressive disease and adjunct perioperative interventions.
Whether following elective, or emergency colorectal surgery, fecal diversion away from fresh anastomoses is an essential component in patient recovery. Ileostomies are preferentially used over colostomies in this setting, when possible, due to better rates of reversal and infection,1 and are common means of anastomotic protection after excision of distal colon, or rectal cancers. Other indications include relief of intestinal obstruction and control of bacterial contamination in cases of peritonitis or non-healing sacral wounds in the incontinent patient.2 Recent investigations into early stoma reversal, as early as 10 days following the index operation, have demonstrated some success for multiple pathologies,3 while as many as 28% of colostomies and 21% of ileostomies are never reversed.4 Contrary to pathologic enterocutaneous fistulae (ECF), which often close spontaneously following conservative management,5 iatrogenic diverting stomae always require additional surgery to close, with only 3 exceptions reported in the literature to date.6,7 The factors contributing to this phenomenon are unknown, and the reported patient characteristics varied. Our experience with one such patient further demonstrates the potential for the human body to heal itself despite considerable synchronous pathology. Our objective in presenting this particular case is to highlight the clinical features of a spontaneous ileostomy closure.
Case Report
A 65-year-old woman underwent elective en bloc total colectomy, hysterectomy, and bilateral salpingoophorectomy followed by side-to-end stapled ileorectal anastomosis and loop ileostomy for locally invasive, moderately differentiated, T4N0M0 adenocarcinoma of the distal colon. This pathology was originally discovered 3 months prior following laparoscopic lavage and drainage of a contained colonic perforation. Intervening endoscopy and histopathologic analysis revealed a positive hereditary non-polyposis colorectal cancer type-I (HNPCC-I), but without synchronous pathology, thus we meriting the aggressive surgical approach. She had a good pre-operative nutritional state (serum albumin 43 g/L, normal 35-55 g/L) and recovered well from her surgery, achieving expected ileostomy output and oral alimentation within several days. There was no technical malfunction of the ileostomy. There was no incidence of skin breakdown, or surgical site infection. She tolerated her ileostomy quite well, the output of which stabilized between 500-600 cc of effluent per day. Shortly after discharge, she started passing small, infrequent stools without difficulty and began adjuvant chemotherapy with folinic acid, 5-flourouracil, and oxaliplatin (FOLFOX). As chemotherapy progressed, the right lower quadrant loop ileostomy steadily reduced output, retracted and epithelialized until it was completely covered 10 weeks after surgery. A brief period of spontaneous renewed drainage of roughly 100 mL per day resulted in refistulization, however, this also epithelialized and reduced output as her weight, activity, and per rectum bowel habits returned to normal, pre-operative levels. Since the second spontaneous closure 18 weeks after the original surgery, she has completed 6 of 12 cycles of FOLFOX, the stomal orifice has not reopened (Figure 1) and the fascial defect (Figure 2) has remained completely asymptomatic.

Completely closed ileostomy (arrows) in A) supine and B) standing positions.

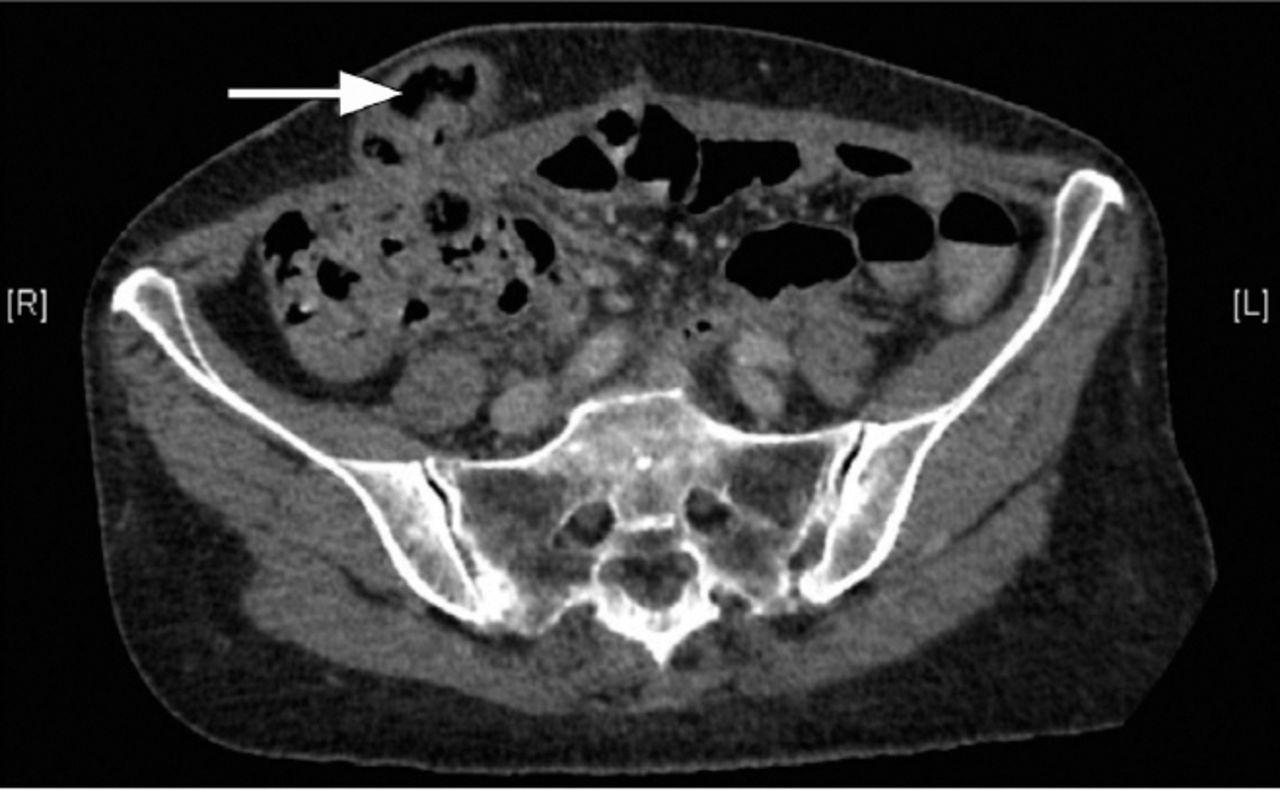
Cross-sectional computed tomography of spontaneously closed loop ileostomy (white arrow).
Discussion
Spontaneous closure of a stoma requires a balance of anatomic and metabolic factors that reflects the rarity with which this event occurs. Considering ostomies as iatrogenic ECF, their patency is usually ensured by fixation of the muscularis to the surgical opening in the rectoabdominal aponeurosis, marsupialization, and fixation of the mucosa to the dermal junction. These factors counteract the forces promoting ostomy retraction and epithelialization such as post-operative weight gain, insufficient mobilization of the diverting limb, and delayed resumption of distal transit of intestinal contents. By itself, retraction is a leading complication of stomas, occurring in up to a quarter of patients. Often preceded by disruption of the skin-mucosa suture line, retraction is associated with stoma edema, cellulitis, and possible intra peritoneal leakage of effluent requiring repeat laparotomy.8 However, in the 2 published reports of spontaneous stoma closures,6,7 as in our case, stoma retraction without such complication and the simultaneous resumption of normal bowel function per rectum seem to be the key elements permissive of spontaneous closure. The persistence of ECF and, in theory, stomae are relative to a variety of pathological, demographic, technical, and co-morbid considerations.9 Classically referred to using the FRIEND acronym (foreign body, radiation, infection/inflammation, epithelialization, neoplasm, distal obstruction) these disease states simultaneously maintain a preferential flow of effluent through an enterocutaneous tract while preventing cellular metabolism and wound healing. Despite considerable pathologies and comorbidities (Table 1), each patient in our review achieved gradual spontaneous stomal closure within 6 months and as early as 6 weeks following its creation.6,7 It seems that providing an appropriate treatment of the potentially confounding comorbidity, namely, resection and adjuvant chemotherapy for cancer, or providing definitive anti-tubercular therapy following tubercular perforation, and rapid reestablishment of an anabolic state via aggressive physical and alimentary rehabilitation, it is possible for spontaneous closure of a stoma to occur. Despite the potential attractiveness of this result, none of the reported patients were dissatisfied with their wound, any agency on the part of the surgeon, or stoma care specialist to provoke stomal retraction should be met with extreme prejudice. Retraction is an unfortunately common complication that usually leads to a lower quality of life and occasionally to operative revision.10 Rather, we advise early recognition and prudent observation of stoma retraction. Given resumption of normal bowel habits, nutritional optimization, appropriate treatment of comorbidities, stomal wound stability and patient comfort, this conservative approach may continue indefinitely and obviate the need for another surgery.
Comparison of reported cases of spontaneous stoma closure.
In conclusion, the rare event of spontaneous stoma closure has received novel recent attention in the literature. Given the presently reported lack of morbidity and high patient comfort with the result, this potential alternative outcome to an otherwise routine component of colorectal surgery should be acknowledged and observed by practitioners. The mechanisms of this event, however, remain poorly understood and additional reports are necessary to determine prognostic factors of both surgical technique and patient presentation that may produce this result.
Supplements
* Supplements will be considered for work including proceedings of conferences or subject matter covering an important topic
* Material can be in the form of original work or abstracts.
* Material in supplements will be for the purpose of teaching rather than research.
* The Guest Editor will ensure that the financial cost of production of the supplement is covered.
* Supplements will be distributed with the regular issue of the journal but further copies can be ordered upon request.
* Material will be made available on Saudi Medical Journal website
Acknowledgment
We would like to acknowledge Dr. Pascal Rousset, Radiologist, Department of Radiology, Hospices Civils de Lyon, Pierre Bénite, France for interpreting the image presented in Figure 2.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 25, 2016.
- Accepted April 13, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}