


Abstract
Objectives: To conduct a meta-analysis and investigate the diagnostic value of 64-slice computed tomography (CT) angiography for diagnosing coronary artery disease (CAD) in patients.
Methods: A comprehensive literature search from March 2005 to August 2014 was performed on the following databases: Cochrane Library; Medline; EmBase; PubMed; and BioMed Central database. As a reference standard, studies that assessed 64-slice CT angiography in detecting coronary artery stenosis (CAS) with invasive coronary angiography were included. Coronary artery stenosis was defined as ≥50% diameter stenosis. Diagnostic value was determined by pooling sensitivity, specificity, positive likelihood ratio (PLR) and negative likelihood ratio (NLR) values at segment-level analysis. Diagnostic accuracy was undertaken using area under the curve (AUC) value and summary receiver operating characteristic (SROC) curves. Publication bias was examined by Deek’s funnel plot asymmetry test.
Results: Eight studies were included in the analysis, enrolling a total of 579 patients (7,407 segment coronary vessels). At segment-level, pooled sensitivity value was 90% (95% confidence interval [CI]: 83-95%), specificity was 91% (95% CI: 61-98%), PLR value was 9.7 (95% CI: 1.8-53.3), and NLR value was 0.11 (95% CI: 0.05-0.22) for CAS. Optimal cut-off point of sensitivity was 90%, and specificity under the SROC curve was 91%. The AUC value was 0.94.
Conclusion: The 64-slice CT angiography is a reliable tool for detection of CAD when using a cut-off of ≥50% diameter stenosis in elderly population.
Coronary artery stenosis (CAS) is not only observed in coronary atherosclerotic heart diseases, but also in Kawasaki diseases associated with coronary damages.1,2 Conventional coronary angiography has been considered as the gold standard method for diagnosing coronary lesions. However, coronary angiography is unlikely to be accepted in the absence of significant lesions and risk of complications due to its invasive features.3 Therefore, an alternative noninvasive procedure for determining CAS is necessary. In recent decades, multi-slice spiral computed tomography (CT) coronary angiography has become one of the hot spots in cardiovascular imaging technology. This method has been applied for evaluating CAS, and was proposed as a potential alternative procedure for invasive coronary angiography.4 Multi-slice CT imaging technology advances have undergone 4-slice, 16-slice, 64-slice and 256-slice stages. Progress of multi-slice CT systems has allowed increased accuracy in quantifying obstructive lesions of coronary arteries.5 Many researchers have used multi-slice CT coronary angiography to determine CAS using invasive coronary angiography as a standard of reference.6,7 However, great variations in sensitivity, specificity, and diagnostic accuracy exist. The 64-slice CT scanner is widely used in current clinical practice due to its high temporal and spatial resolution. In order to assess the diagnostic accuracy of 64-slice CT in determining CAS, we conducted a meta-analysis of currently published studies that compared 64-slice CT angiography with conventional coronary angiography for diagnosing CAS.
Methods
Search strategy
This meta-analysis was conducted according to guidelines of the Standards for Reporting of Diagnostic Accuracy Initiative.8 A comprehensive literature search from March 2005 to August 2014 was conducted on the following databases: Cochrane Library; Medline; EmBase; PubMed; and BioMed Central database. The following medical subject headings in various combinations were used: computed tomography, multi-slice CT, coronary angiography, coronary artery stenosis, sensitivity, specificity, and positive or negative predictive value. Reference lists of all relevant citations were manually searched and retrieved to identify additional eligible studies.
Study selection
Inclusion criteria were as follows: studies that assessed 64-slice spiral CT for detecting CAS; used invasive coronary angiography as a reference standard; clearly provided or derivable absolute numbers of true-positive (TP), false-negative (FN), false-positive (FP) and true negative (TN) values; studies that were based on segment-level analysis and detected vessels ≥12 segments; and significant stenosis were defined as the presence of >50% reduction of luminal diameter in vessels larger than 1.5 mm. Review articles, comments, conference abstracts and non-original papers were excluded.
Data extraction and quality assessment
Two authors independently extracted data from each study, and any differences were resolved by discussion. If TP, FP, FN and TN data were not provided, data in the form of sensitivity, specificity, positive likelihood ratio (PLR) and negative likelihood ratio (NLR) were used for calculating the absolute numbers. The following data were recorded: first author’s name; year of publication; sample sizes; gender; age of subjects; segment number; as well as, TP, FP, FN and TN number based on per-segment category and prevalence of stenosis. Quality Assessment of Diagnostic Accuracy (QUADAS)-2 tool9 was used to evaluate the methodological quality of included studies.
Statistical analyses
Meta-analysis for diagnostic accuracy of 64-slice CT in patients with CAS was conducted by pooling sensitivity, specificity, PLR, NLR, and diagnostic odds ratio (DOR) estimates using a bivariate mixed-effects binomial regression model. Area under the curve (AUC) value and summary receiver operating characteristic (SROC) curve was computed to evaluate diagnostic accuracy. The PLR was calculated as sensitivity/(1-specificity), and NLR was calculated as (1-sensitivity)/specificity. The DOR was calculated as PLR/NLR. The I2 statistic <50%, and Cochran Q statistic value of p>0.10 indicated the presence of significant heterogeneity. A fixed-effect model was selected in the absence of significant heterogeneity; otherwise, a random effects model was used. Deek’s funnel plot asymmetry test was used to examine potential publication bias.10 All analyses were performed using STATA software version 12 (StataCorp LP, College Station, TX, USA). A p<0.05 was considered statistically significant.
Results
Characteristics of included studies
Figure 1 presents a flow chart for the study selection process. A total of 341 relevant citations were identified in the initial literature search. After title and abstract screening, 292 papers were excluded mainly because these were not original articles (review, meta-analysis, comments, and conference abstracts, or uninteresting outcomes). A total of 49 full-text articles were reviewed for detailed evaluation. Finally, 8 studies11-18 met the predefined criteria. Table 1 shows the characteristics of the included studies. Eight eligible studies enrolled 579 patients with 7,407 vessel segments. Among the 8 studies, 5 studies,11-14,17 enrolled patients based on consecutive cases, while 3 studies15,16,18 enrolled patients on selected patterns. The number of included patients varied from 52-104. All studies were published from 2005 to 2013. Most patients were male, and all studies used 64-slice CT angiography. Table 2 summarizes the methodological quality of studies based on QUADAS-2 tool. Overall, studies had a moderate to high quality.

Flow chart of study selection process.
Characteristics of studies included in the meta-analysis.
Quality assessment of included studies.
Segment-based analysis
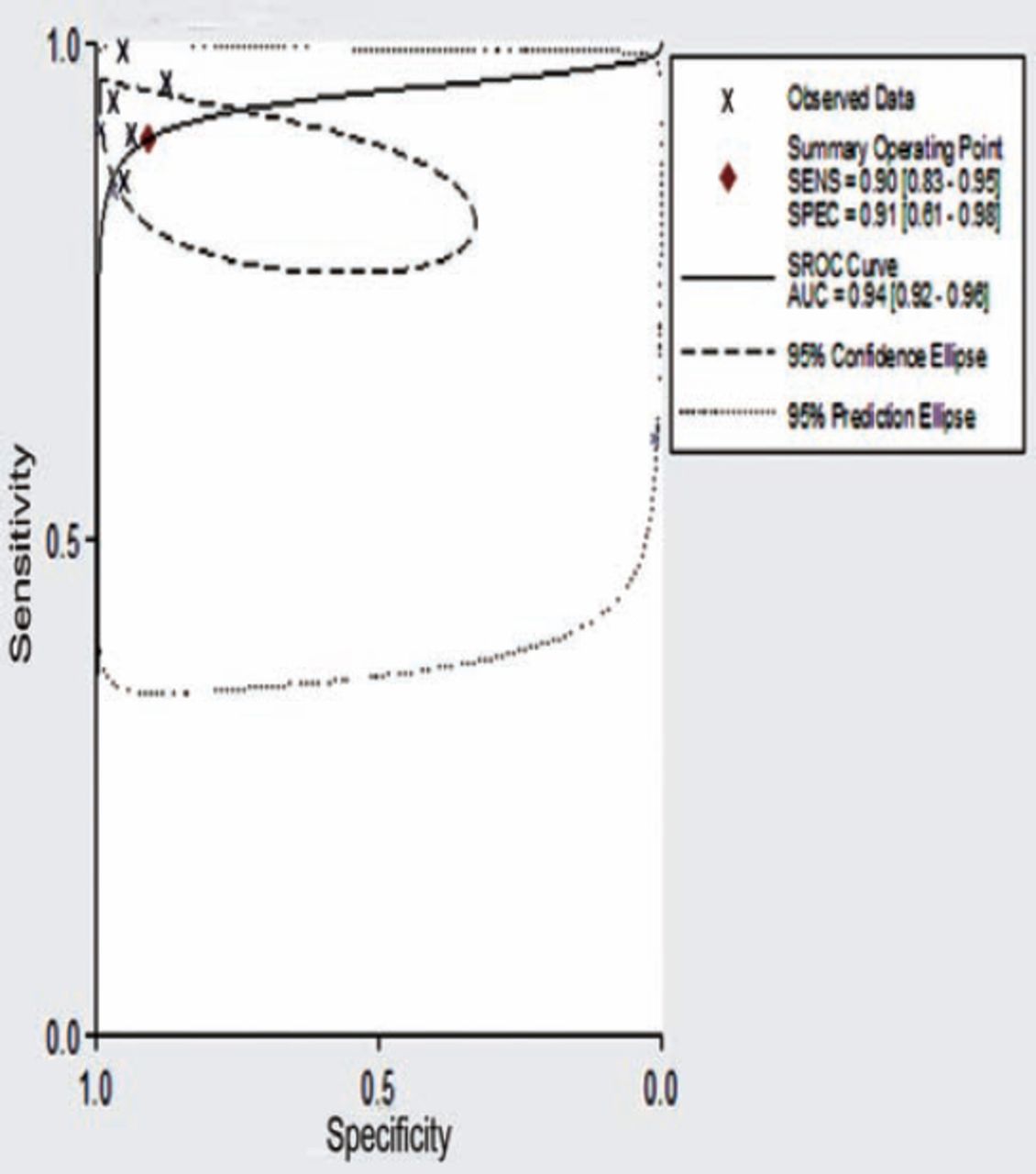
As shown in Figures 2A & 2B, a random effect model was applied due to significant heterogeneity among sensitivity (I2=99.77) and specificity (I2=99.93) results. Pooled sensitivity was 90% (95% confidence interval [CI]: 83-95%), and specificity was 91% (95% CI: 61-98%) at segment-level. As shown in Figure 3, pooled PLR was 9.7 (95% CI: 1.8-53.3), NLR was 0.11 (95% CI: 0.05-0.22), and DOR value was 90 (95% CI: 9-906) at segment-level. For 64-slice CT angiography (Figure 4), in determining CAS, optimal cut-off point of sensitivity was 90%, and specificity was 91% under the SROC curve as indicated in Figure 5, while AUC value was 0.94 (95% CI: 0.92-0.96).

Forest plots for sensitivity (A) and specificity (B) of 64-slice computed tomography angiography in determining coronary artery stenosis.

Forest plots for negative likelihood ratio and positive likelihood ratio of 64-slice computed tomography angiography in determining coronary artery stenosis.

An image showing that in 64-slice CCTA, the maximum intensity projection technique demonstrates normal coronary artery (A), and severe narrowing of the right coronary artery (B).

Summary receiver operating characteristic (SROC) curve with confidence and prediction regions around mean operating sensitivity and specificity points for determining coronary artery stenosis is shown. Red diamond represents the best diagnostic cut-off point. Peripheral relative (densely dotted) represents prediction confidence, while inner oval dashed lines indicate the confidence region.
Publication bias
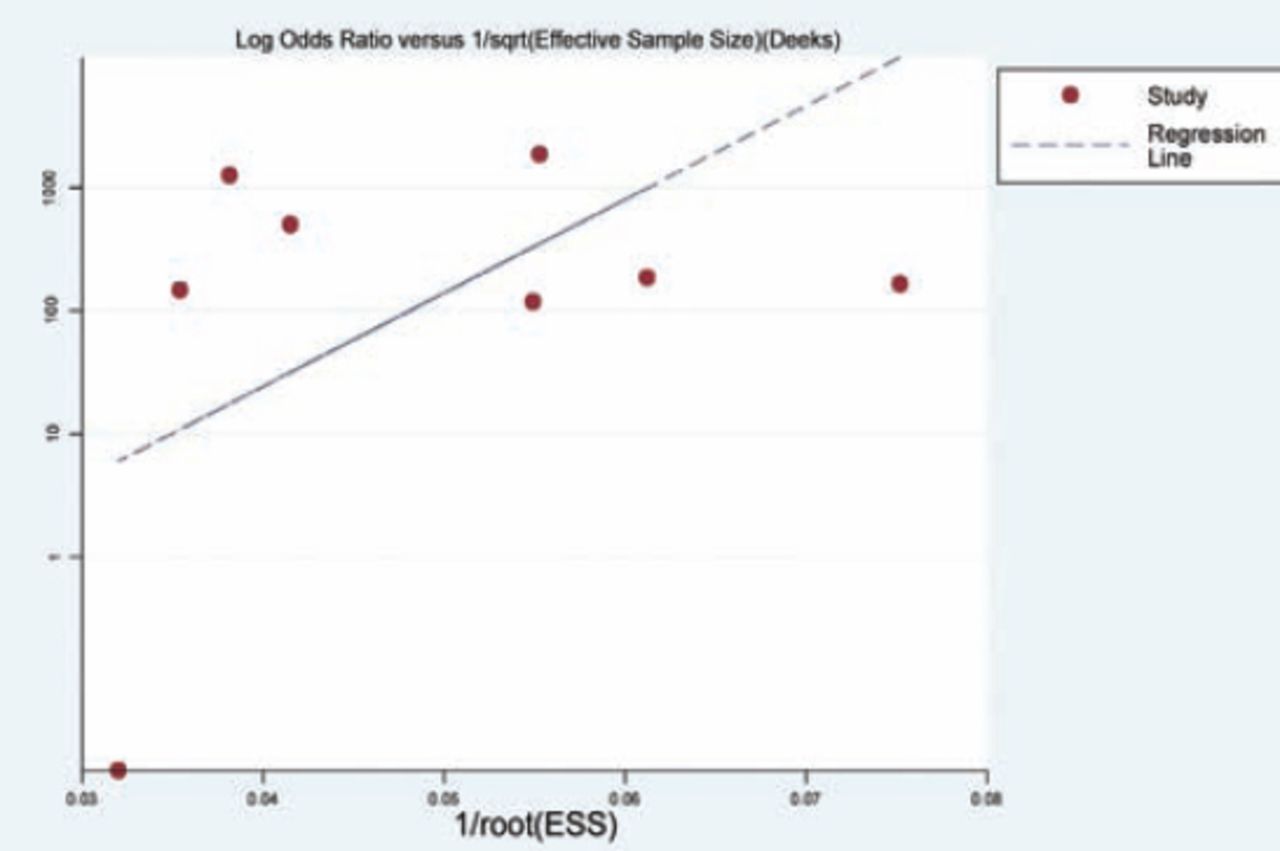
The p-value for slope coefficient in Deek’s funnel plot asymmetry test was 0.244, suggesting a low likelihood of publication bias (Figure 6). Spearman correlation coefficient indicated a threshold effect (Spearman correlation coefficient=-0.262; p=0.531).

An image showing Deek’s funnel plot with superimposed regression line for identifying publication bias.
Discussion
Eight studies that assessed the diagnostic accuracy of 64-slice CT angiography for detecting CAS were identified in this meta-analysis. Diagnostic performance of 64-slice spiral CT angiography for detecting significant CAS on a segment-based analysis indicated a sensitivity of 90%, and specificity of 91% using the bivariate mixed-effects binomial regression model in the elderly population. Coronary arterial lesions, including CAS in children, usually occur in Kawasaki coronary artery disease, or congenital anomalies. Higher incidence of CAS occurs in patients with coronary heart disease, particularly patients over 60 years old with an insidious onset. Invasive coronary angiography has long been considered as the gold standard method for detecting coronary lesions. However, conventional coronary angiography is unlikely to be accepted in some cases such as infants, young children, or severely atherosclerotic patients due to its invasive features. Therefore, it is necessary to search for alternative noninvasive procedures for determining CAS. The development of multi-slice spiral CT systems has provided the possibility of qualitative identification of coronary arteries. The 64-slice has a high temporal and spatial resolution compared with the 4-slice or 16-slice.19 A 64-slice CT scanner can nearly achieve isotropic voxels within 10 seconds, and has a potential of replacing conventional coronary angiography.
In the current study, we selected the bivariate mixed-effects binomial regression model to calculate sensitivity, specificity, PLR, and NLR values. The DOR was calculated because they did not depend on disease prevalence. The DOR was 90, which suggested a relatively high diagnostic accuracy. The SROC curve was the most appropriate summary statistic due to the diagnostic threshold variation among research studies. The SROC curve further indicated a high diagnostic accuracy for 64-slice CT angiography with an AUC of 0.94. It should be noted that the SROC curve and DOR are both difficult to use in clinical practice, while a likelihood ratio is a more clinically meaningful measure for diagnostic accuracy. The PLR value was 9.7, which suggested that patients with CAS had approximately 9.7 times likelihood of being diagnosed than patients without CAS. The NLR value was 0.11, which suggested that 64-slice CT angiography had an excellent ability to exclude coronary artery ≥50% stenosis.
Although 64-slice CT angiography has exhibited high diagnostic accuracy for detecting CAS in daily clinical practice, further confirmation is needed due to the robustness of our study; since these findings were obtained under specific conditions. Most of the patients in this study were in the elderly population with a mean age of 60.2 years old. Therefore, generalizing these findings for other age populations is limited. First, this might be explained by the low incidence of coronary stenosis in children or adolescents, and the cautious application of CT in children with CAD. Second, radiation burden has always been a concern in pediatric radiology, and the use of 64-slice CT for pericardial narrowing in children is unlikely due to the higher radiation burden of the 64-slice CT versus 256-slice CT and dual source CT,20 which limited the application of 64- slice CT in the diagnosis of coronary stenosis in children. Third, only those with ≥50% obstructive lesions in coronary arteries were included in the analysis. Lesions of coronary stenosis <50% could not be analyzed due to the limited number of studies and small sample size.
Diagnostic accuracy of coronary angiography using 128- and 256-slice CT in CAS was also reported in literatures. A well-designed meta-analysis summarized literatures on the diagnostic accuracy of 320-slice CT angiography for detecting CAS; and revealed that pooled sensitivity was 78%, specificity was 98%, PPV was 82%, and NPV was 97% at segment-level.21 These findings suggest that 320-slice CT angiography is lower than 64-slice CT angiography in diagnostic performance for determining ≥50% CAS at segment-level.
Computed tomography is accurate in CAD, but not so in quantifying the severity of a given stenosis. The CCTA can quantitatively evaluate the degree of CAS by detecting its diameter and area. However, its diagnostic value is not superior to coronary angiography. A well-designed meta-analysis22 indicated that there was a high correlation between CCTA and ICA in diagnosing CAS. However, standard errors may exist. Therefore, it was best to describe the extent of stenosis in a wide range. The CCTA has been clinically used for exclusion of significant coronary stenoses in patients with a probability of CAD. Coronary calcification is an important diagnostic concern affecting diagnostic accuracy of CCTA.23 When severe coronary artery calcification develops, CTA imaging can enlarge the calcified plaque and subsequently influence the quality of the coronary artery lumen; resulting in measurement errors of CAS. Increased coronary calcifications have been demonstrated to lower the predictive negative value of 64-slice CT angiography due to increased likelihood of false positive stenoses.24 Diagnostic performance of 64-slice CT angiography was significantly reduced in diabetic patients than non-diabetics with similar clinical characteristics.25 These findings suggest that 64-slice CT angiography could be used for screening CAS in low risk patients. In addition, high radiation exposure is another concern. Some attention must be given to potential health risks associated with ionizing radiation received during cardiac CT examinations.
There were a number of limitations in this study. First, per-patient data analysis is the most pertinent and realistic method for interpreting results, and we only conducted this study based on segment-level. Second, three studies enrolled selected patients and five studies enrolled consecutive patients. Thus, prevalence of coronary artery ≥50% stenosis might influence PLR and NLR results. Third, significant heterogeneity in this analysis was a challenge. Study sample size, patient’s characteristics, as well as the number of assessable segments all contributed to heterogeneity. Finally, a subgroup analysis was not conducted due to the relatively small study number or sample size of included studies.
In conclusion, the 64-slice CT angiography is a reliable tool for the detection of CAD when using a cut-off of ≥50% diameter stenosis in elderly populations. In particular, its low negative predictive value allows this method to serve as a screening procedure for identifying patients who have a relative risk of CAS. Diagnostic accuracy of 64-slice CT angiography for detecting CAS in children or adolescents remains inconclusive. Future studies for investigating the diagnostic value of 64-slice CT angiography in children or adolescents needs to be further evaluated.
Related Articles
Tan Q, Wang Q, Liu D, Zhang S, Zhang Y, Li Y. Intravascular ultrasound-guided unprotected left main coronary artery stenting in the elderly. Saudi Med J 2015; 36: 549-553.
Shi HW, Pu P, Deng W, Zhou H, Bian ZY, Shen DF, et al. Prognostic value of late gadolinium enhancement in dilated cardiomyopathy patients. A meta-analysis. Saudi Med J 2013; 34: 719-726.
Alosaimi FD, Baker B. Clinical review of treatment options for major depressive disorder in patients with coronary heart disease. Saudi Med J 2012; 33: 1159-1168.
Footnotes
Disclosure. This work was supported by grants from the Chinese Natural Science Foundation (No. 81370217 and No. 81300124), and the Jiangsu Foundation (No. BE2013632 and H201127), Jiangsu, China.
- Received May 26, 2015.
- Accepted August 27, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.