


Abstract
Objectives: To evaluate the effectiveness and retention of learning automated external defibrillator (AED) usage taught through a traditional classroom instruction (TCI) method versus a novel self instructed video (SIV) technique in non-critical care nurses (NCCN).
Methods: A prospective single-blind randomized study was conducted over 7 months (April-October 2014) at the Universiti Kebangsaan Malaysia Medical Center, Kuala Lampur, Malaysia. Eighty nurses were randomized into either TCI or SIV instructional techniques. We assessed knowledge, skill and confidence level at baseline, immediate and 6-months post-intervention. Knowledge and confidence were assessed via questionnaire; skill was assessed by a calibrated and blinded independent assessor using an objective structured clinical examination (OSCE) method.
Results: Pre-test mean scores for knowledge in the TCI group was 10.87 ± 2.34, and for the SIV group was 10.37 ± 1.85 (maximum achievable score 20.00); 4.05 ± 2.87 in the TCI and 3.71 ± 2.66 in the SIV (maximum score 11.00) in the OSCE evaluation and 9.54 ± 3.65 in the TCI and 8.56 ± 3.47 in the SIV (maximum score 25.00) in the individual’s personal confidence level. Both methods increased the mean scores significantly during immediate post-intervention (0-month). At 6-months, the TCI group scored lower than the SIV group in all aspects 11.13 ± 2.70 versus 12.95 ± 2.26 (p=0.03) in knowledge, 7.27 ± 1.62 versus 7.68 ± 1.73 (p=0.47) in the OSCE, and 16.40 ± 2.72 versus 18.82 ± 3.40 (p=0.03) in confidence level.
Conclusion: In NCCN’s, SIV is as good as TCI in providing the knowledge, competency, and confidence in performing AED defibrillation.
The ability to perform defibrillation promptly and competently in patients with ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT) is a major determinant to increase the chances for survival. Early defibrillation is the strongest predictor of survival from cardiac arrests due to VF and pulseless VT1,2 It is estimated that one-third of in-hospital sudden cardiac arrests are not appropriately handled or defibrillated within the recommended time, namely, within 3 minutes of arrest.3 Cardiac arrest emergencies may happen anywhere, and in non-critical care wards are usually first handled by nursing staff. Accordingly, the in-ward nurses are important frontline and primary responders for critical or resuscitation situations. It is therefore crucial for ward nurses to be able to perform good basic life support (BLS) and operate automated external defibrillators (AED) effectively. Critical care ward nurses handle emergencies regularly, but non-critical care nurses (NCCN) face these situations less frequently. In the Nursing Department at Universiti Kebangsaan Malaysia Medical Center (UKMMC), NCCN attended BLS/AED courses during their training years. Although it is a requirement to possess the skill of operating an AED whilst in service, many have not had the opportunity of attending a refresher course. Therefore, a large number of nurses may require re-training in AED use to maintain their competency. However, due to busy schedules and inadequacy in the number of available classes4,5 most are unable to attend refresher classes. Traditional classroom instruction (TCI) training for AEDs consumes significant resources, namely, time, manpower, and space. Moule et al6 in 2008 performed a non-randomized comparison of e-learning and classroom delivery of BLS with AED and suggested that computer training could develop skills in cardiopulmonary resuscitation (CPR) and AED more effectively than classroom training for nurses and others. In non-monitored hospital beds and during procedures in diagnostic facilities, defibrillation may be delayed when patients develop sudden cardiac arrest.3 The American Heart Association (AHA) in 2010 advised the use of AEDs for the in-hospital setting to facilitate early defibrillation in staff who have no rhythm recognition skills or have infrequent experience with defibrillators.7 This highlights the importance of non-critical nurses operating AEDs effectively as many do not know how to use a manual defibrillator. Studies have shown that in medical students and doctors, self-instruction videos (SIV) were as good or better than TCI for the acquisition of emergency skills such as CPR, cervical collar application, and splintage.8 In nursing students, a computer-based course (HeartCode BLS) with voice advisory manikin (VAM) feedback improved the subsequent performance of CPR in terms of hand placement, depth of compression, and ventilation.9 However, very few studies assessed the competency in CPR-AED among non-critical care nurses using a SIV based programme. We performed this study to determine whether NCCN were able to learn the use of AEDs via SIV and retain their competency (knowledge and skills) for a period of 6 months at least, as well as those who learned through TCI courses.
Methods
This was a prospective, single-blind, randomized controlled trial performed among NCCNs working in UKMMC, a tertiary referral and academic center located in the capital city of Kuala Lumpur, Malaysia. The study was conducted between April and October 2014. This study was approved by the Universiti Kebangsaan Malaysia’s Research and Ethic Committee, which strictly adheres to the Helsinki Declaration.
Development of the self-study package
In the initial phase of this study, the research team concentrated on making the Self-Learning Package (SLP) teaching video: This contained an introduction, learning objectives, triggers for use, and steps in operating the AED. It was performed in English and the native language (Bahasa Malaysia). The theoretical parts of the SLP were delivered using the Screencast-O-Matic application. Practical aspects were performed by the researchers who videoed and edited the whole procedure using a 2-camera technique to optimize visualization of the tasks. Volunteers were used as actors. Simulation of the defibrillation with the AED was performed on the volunteers and a manikin.
Assessor and facilitator preparation
To standardize the marking process, calibration of the assessors was implemented by briefing and attending several training sessions. The assessors were given videos of several CPR/AED performances and asked to mark the performance using a validated 11-point checklist prepared by a panel of experts of emergency physicians and medical educationists in UKMMC.
The facilitators were AHA-certified instructors who were actively conducting BLS-AED courses on a regular basis. They were briefed regarding the study, and shown the SLP video so that the identical teaching content could be delivered to the TCI groups. The assessors and facilitators comprised 2 different groups of people.
Participant recruitment
An invitation to participate in this study was sent to all the non-critical care units in UKMMC: internal medicine, surgical, pediatrics, oncology, psychiatry, and obstetric and gynecology wards. Nurses working in healthcare clinics, operating theaters, day-care, and radiology departments were also invited. All registered nurses working in the specified units who had worked continuously from January 2013 to October 2014 in UKMMC were included. Those working in critical care units, for example, intensive care unit, coronary care unit, high dependency ward/unit, pediatrics intensive care unit/pediatrics high dependency unit, emergency department (ED); or those who had recently transferred out from these units, or who did not give consent were excluded.
Selected nurses were then randomized into parallel groups: Group A: TCI and group B: SIV. Sample size was calculated via OpenEpi software available online (Atlanta, GA, USA) (http://www.openepi.com/). This gave a number of 76, where a 20% drop out rate was added giving a final sample size of 90 nurses.
Research design
Both groups underwent a pre-test that assessed knowledge, confidence level, and competency on AED uses. Each nurse was given a unique number that was used throughout the study for data collection and assessment to minimise bias. The initial 40 participants were divided into 2 subgroups. 20 nurses attended TCI, and were further divided into subgroups giving tutor-participant ratios of 1:6-7. The other 20 nurses attended a SIV group teaching session. The cycle was repeated for a total of 80 participants.
Questionnaires were used to record demographic data consisting of section A for personal data, and section B for professional data and working experiences. Twenty multiple choice questions of single best answer were used to assess their AED knowledge and its use. A 5-point Likert scale was used to gauge confidence levels of the participants on AED. Competency was assessed using an 11-point objective structured clinical examination (OSCE) checklist.
Group A underwent training sessions using TCI methods on AED use for one hour immediately following their pretest. During the session they were given a 15-minute lecture together with a hands-on training session using an AED (Laerdal’s AED trainer-2 followed the 2005 Guidelines and Philips HeartStart Adult Training Pads) (Phillips Medical Systems, Bothell, WA, USA). The immediate post-test assessment (0-month) was carried out within 7-14 days after training.
Group B, underwent the SIV training. They were given a SLP that consisted of the learning objectives, video lectures on CPR/AED, on the stepwise approach for AED use, and frequently asked questions. They were given 7 days to complete the task of going through the SLP and hands-on practice with the AED. Within this 7-day period they were also given free access to the Skills lab situated in the ED of UKMMC. They were allowed to bring the SLP DVD during the hands-on practice, but no instructor or facilitator was present. A Simulation lab technician was present to prepare the manikin-AED and handle administrative matters, namely, log in/out. Screening was carried out via their unique code number to ensure that only SIV group nurses were allowed access to the practice lab. Immediate post-test assessment (0-month) was performed within 7-14 days after the pretest. Both groups were re-assessed for retention on all 3 components 6 months after the training and post-test.
Data analysis
Data collected were tabulated and analysed using the Statistical Package for Social Science version 20 (IBM Corp., Armonk, NY, USA). Parametric testing (student t-test) of mean differences was conducted as the data was normally distributed.
Results
Eighty nurses were selected out of the 100 nurses available for this study. They were randomly allocated into groups: group A (TCI) consisting of 39 nurse and group B (SIV) consisting of 41 nurses. There were no differences in age, gender, working unit, and working experience between the groups (Table 1). The participants were between 23-46 years of age for group A (TCI, N=39) with mean ± standard deviation (SD) of 30.62 ± 5.37, and 24-39 years of age for group B (SIV, N=41) with mean ± SD of 31.32 ± 4.07. Most of the nurses (96.0%) were female. There were no significant differences between the groups in terms of previous courses attended (BLS and ACLS), and previous experience in operating an AED (Table 1). Among the nurses who had worked for >5 years, only 25% of group A attended a BLS course and 3.8% attended an advanced cardiac life support (ACLS) course, while 30% of group B attended a BLS course, and 5% attended an ACLS course. Only one person (from the SIV cohort) had previously experienced operating an AED although 24 nurses had observed AED use prior to the study.
Demographic data on participating nurses-baseline characteristics of the study population.
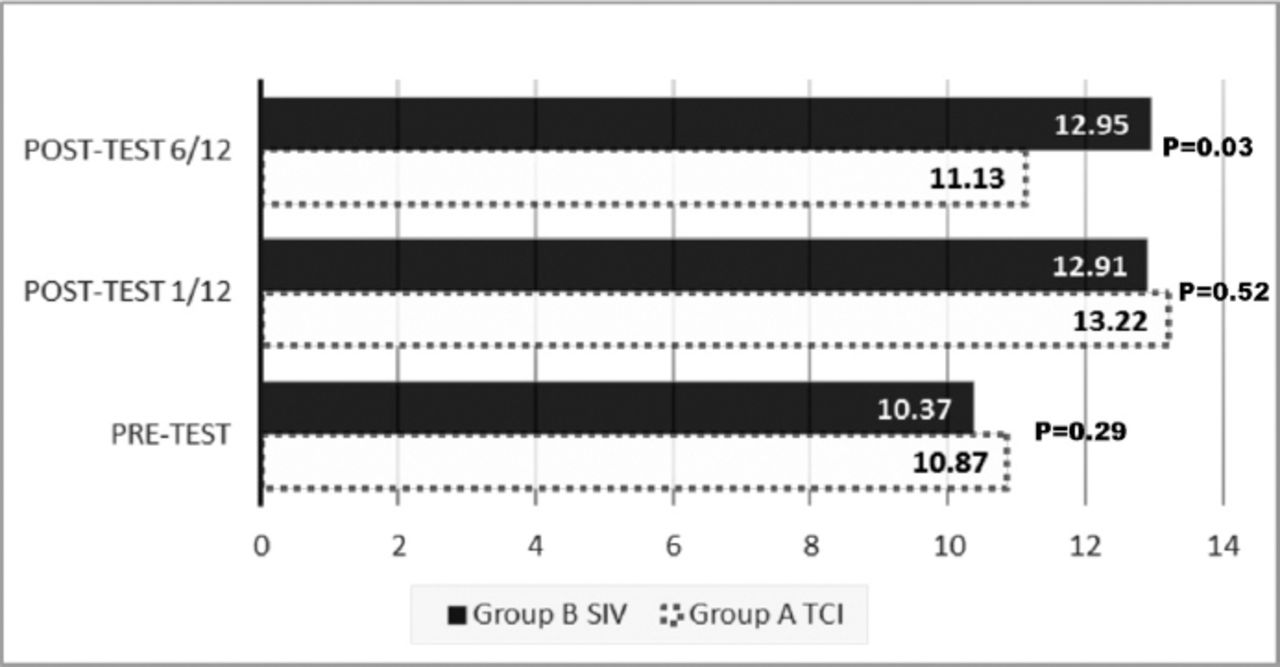
There was no significant difference between TCI and SIV in baseline (0-month) mean scores for knowledge 10.87 ± 2.34 versus 10.37 ± 1.85, out of a total score of 20 marks. At immediate post-test, both groups achieved improvement by more than 20% (13.22 ± 1.92, TCI versus 12.91 ± 2.08, SIV). At 6 months, there was a significant difference in the post-test retention between the groups: the TCI group scored 11.13 ± 2.70 compared with 12.95 ± 2.26 in the SIV (p=0.03) (Figure 1).
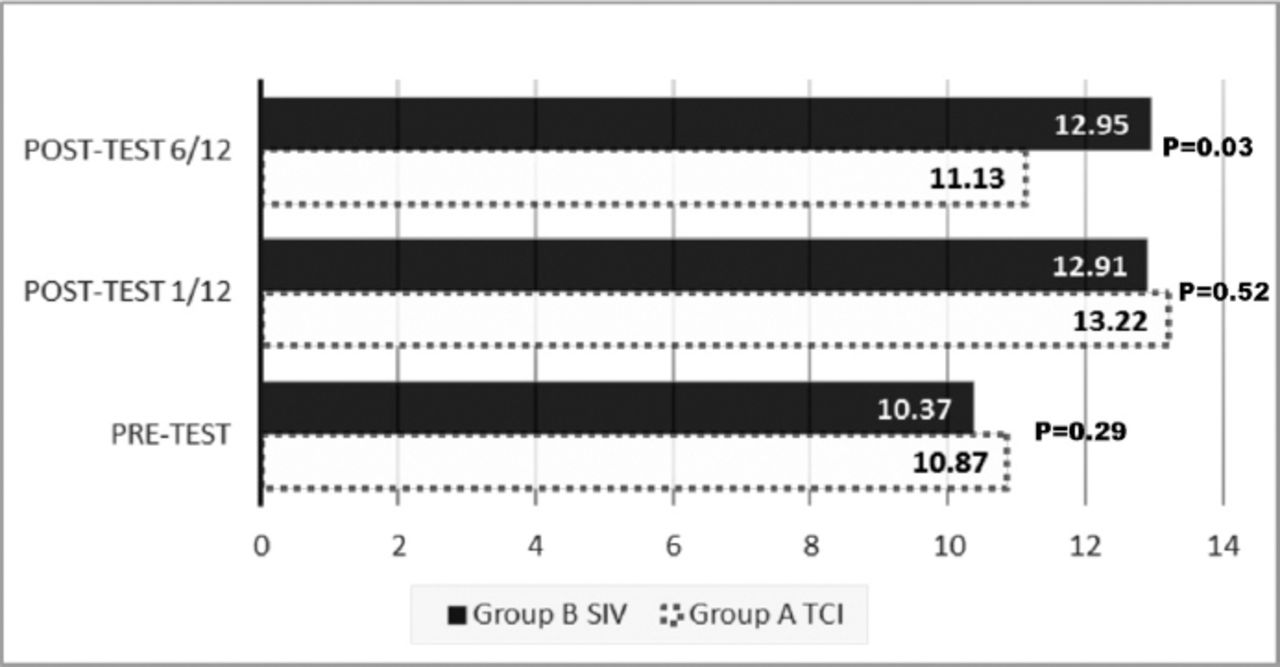
Data on pre (-1-month), post (0-month) and retention 6-month assessment on automated external defibrillators knowledge for both groups. *P<0.05 is considered significantly different. **Total score for knowledge is 20 marks. SIV - self-instruction videos, TCI - traditional classroom intervention
In the skills performance OSCE, both groups scored similarly in the pre-test assessment. There was an improvement at the immediate post-test for both TCI and SIV groups. The SIV group demonstrated better retention at 6 months although this did not reach statistical significance (Table 2).
Data on pre (0-month), immediate-post (1-month), and retention-post (6-month) assessment on competency in AED use for group A and group B.
Table 3 depicts the competency among the participating nurses with 34 out of 37 (91.0%) in the TCI group compared with 31/34 (91.2%) in the SIV group able to successfully perform defibrillation immediately after exposure to the different teaching methods. At 6 months, 7 out of 16 (43.75%) of the TCI and 13 out of 21 (61.90%) of the SIV group were able to successfully defibrillate using the AED, but this did reach statistical significance. The retention skills at 6 months are shown in Table 3.
Objective structured clinical examination outcome (successful defibrillation) on pre, post and 6 months assessment for both groups.
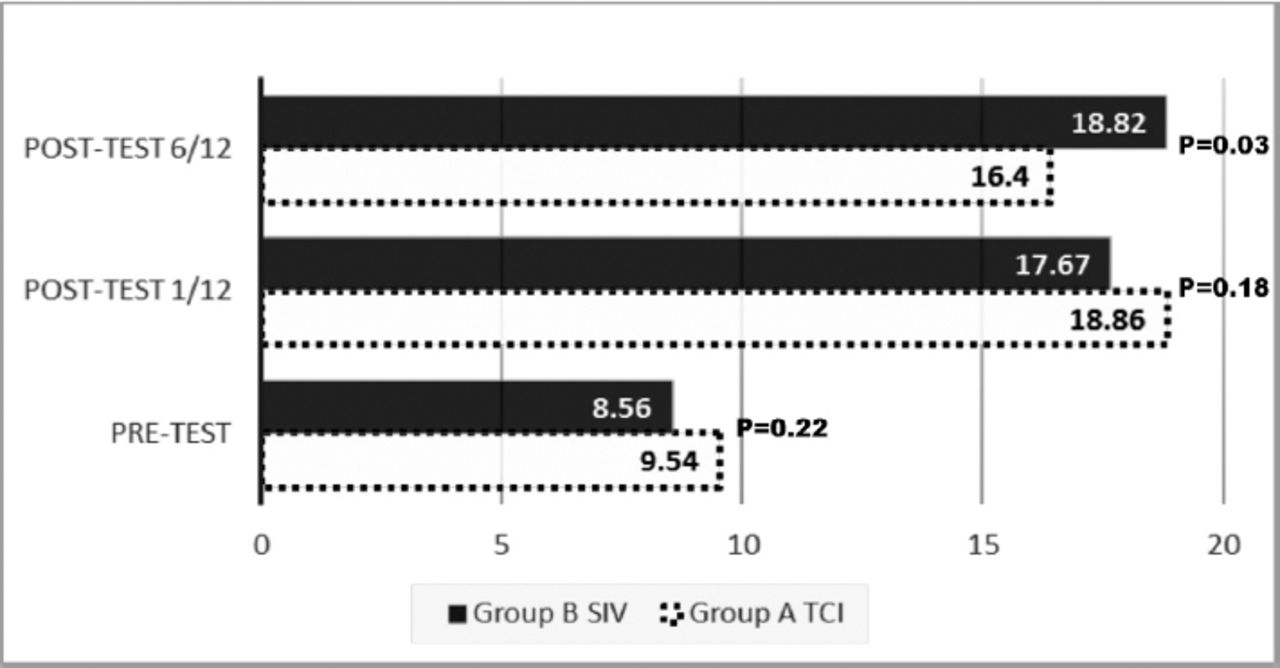
In the confidence scores the mean scores in pre-test assessment for both groups (TCI and SIV) were 9.54 ± 3.65 and 8.56 ± 3.47 out of a total maximum of 25 marks (p=0.22). There was a clear improvement in both groups 18.86 ± 3.60 for TCI versus 17.67 ± 3.71 SIV in the immediate post-test period. However, at the 6 month test, there was a significant difference - the SIV group maintained their improvement (18.82 ± 3.40), while the TCI group demonstrated a reduction to 16.40 ± 2.70 (p=0.03) (Figure 2).
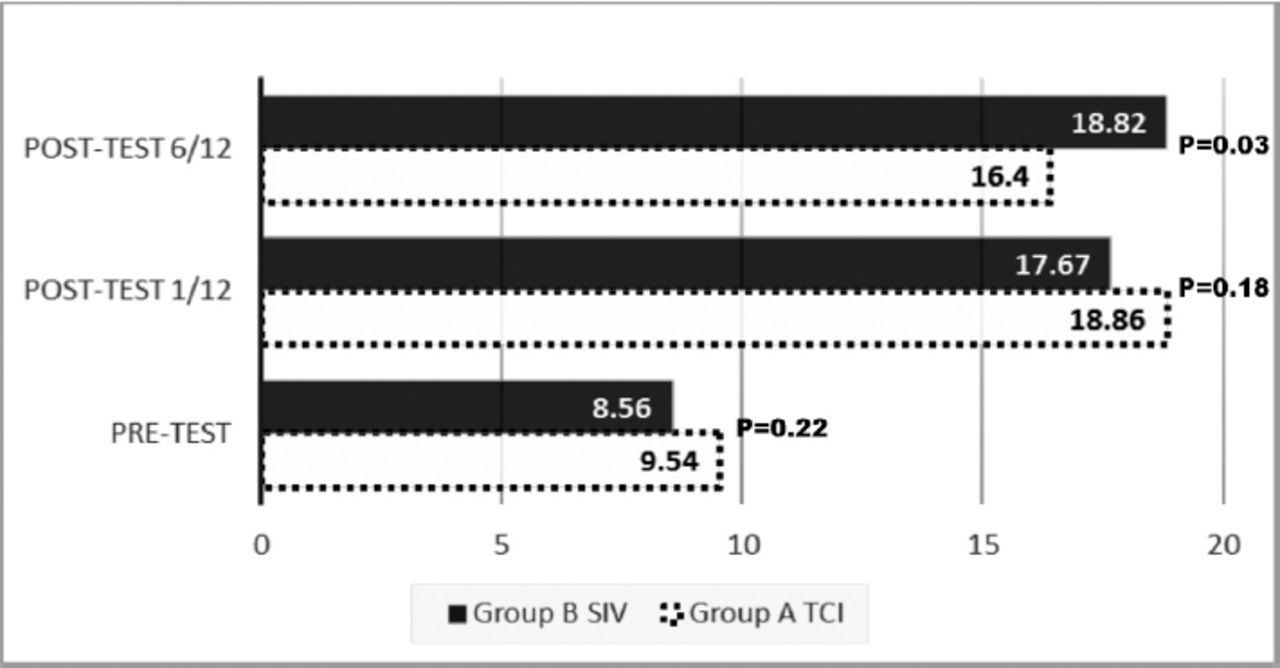
Data on pre (-1-month), post (0-month) and retention 6-month assessment on confidence score for both groups. *P<0.05 is considered significantly different. **Total score for confidence level is 25: <5 is not confident; 6-10 slightly confident; 11-15 confident; 16-20 slightly more confident; and 21-25 very confident. SIV - self-instruction videos, TCI - traditional classroom intervention
Discussion
In this study we noted that the NCCNs who used the SIV technique of learning CPR/AED demonstrated better retention in all 3 assessment categories - knowledge, skill performance, and confidence level, although a significant difference was noted only for knowledge and confidence level.
In terms of knowledge, there was a significant improvement in knowledge mean scores (p<0.05) for both groups regardless of the methods used (TCI or SIV) for training and scores increased in the immediate post-test period of TCI by 21.2% and of SIV by 26.6%. At the 6-month post-test assessment we expected both groups to have reduction in their knowledge. However, the SIV group demonstrated significant knowledge retention level and their scores improved by 0.28 ± 2.80. In contrast, the TCI group demonstrated usual pattern of knowledge decay (Figure 1).
We are unable to compare our results with other studies as we could not find any prior publications that have assessed these specific aspects. We attribute the better marks obtained by the SIV group at 6 months to the continuous access and availability of the DVD by the nurses involved. This helps in knowledge refreshment among the SIV group nurses. One of the top scorers in the SIV group stated that she had watched the DVD more than 5 times during the study. We agree with other studies that knowledge deterioration is unavoidable and necessitates regular refresher courses, but suggest that the use of SIV can be a practical and cost-effective alternative to standard TCI teaching.10,11
Skill performance using an AED was assessed using an OSCE method. The NCCN’s showed an unsatisfactory level of skill competency prior to the study with only 16 (20%) of the nurses successful in delivering a shock during the pre-test assessment. This is in contrast with Mattei et al12 who found that physiotherapists and nurses in the United Kingdom could deliver a shock successfully despite no prior experience using AED. Reasons that might contribute to this difference include language differences since English is not the mother tongue for the majority of the nurses involved in our study, whilst the AED instruction is in English. Arumugam et al13 recently highlighted that Malaysia’s graduate nurses had weak proficiency, communication skills, and confidence in English. The participating nurses were asked regarding language issues. Ten out of 80 said that they could understand the instructions given by the AED device but they would prefer if the instruction was delivered in their native Bahasa Malay language.
There was a significant improvement in performance between the pre-test and the immediate post-test assessments (Table 2). The incremental mean score in post-test assessment was better in the SIV group compared with the TCI group, but this did not reach significance. The post test results at 6 months declined in both groups (Table 2). These results concur with other studies,10,14-17 which have shown deterioration in skills occurring in the post-training period. Again the SIV method showed a better outcome as evidenced by less deterioration at 6 months with a 19.8% reduction in the SIV group versus a 25.7% reduction in the TCI group, although this did not reach significance.
It is interesting that at 6 months the number of nurses in the SIV group able to perform a successful defibrillation, regardless of their OSCE scores, was better than the TCI group (Table 3). This could be attributed to the fact that in the SIV group, they were able to access the DVD at any time within this period, while the TCI could only rely on their past experience, which they had acquired 6 months previously. Even though they were not allowed access to the skill lab or the AED for training, the results still showed that viewing alone can help the NCCN perform the skills better at the 6-month post-test period.
Knowledge and technical skills are clearly important. However the individual must additionally have the confidence and motivation to use an AED. For confidence levels, both our instruction methods produced improvement in the confidence of the nurses in using an AED as evidenced by the improvement in their scores. The TCI group had better scores compared with the SIV group in the immediate post-test period. However, the reassessment at 6 months showed that the SIV group demonstrated better retention scores than the TCI group. This is a 4.9% reduction for the TCI group but an increase of 11.0% in the SIV group (Figure 2). This again could be explained by the availability of DVD with the participants in the SIV group helping to refresh their skills and thereby increasing their confidence.
An important limitation was the relatively small sample size with high dropout rate. We obtained a sample of 80 participants, which was more than our calculated sample size (n=76), but during the 6-month follow up period the number dropped to 37 participants. The main reason was that the staff could not get leave from busy schedules. A bigger sample size would improve the results obtained. A single assessor was used in scoring the performances of the participants since they have undergone the strict process of assessor calibration. Furthermore, all the assessors are part of the BLS instructor team that is familiar with the checklist and participant performance. However, a team of 2 assessors would be a better option to reduce possible bias. The SIV group was given a video package that have dual language, which was in English and Malay. Therefore there was no issue of language barrier in the group. Only the AED instruction was in English and both group used the same AED device. The AED instruction in participants’ native language will greatly improve their confidence in using the device.
We suggest that future training in CPR-AED should allow participants access to skills labs or training facilities after the initial training period. From our study we noted that, even without the presence of an instructor, participants can perform self-directed training and retain the knowledge, skills, and confidence required for longer periods. The presence of a study-aid, such as a video CD or DVD may further enhance this positive effect. Future studies should also explore the duration period before refresher training is required for individuals who have undergone the SIV mode of training.
In conclusion, SIV is as good as TCI in providing the knowledge, competency, and confidence in performing AED defibrillation among non-critical care nurses. This could be a useful avenue in the development of a retention skills program in AED usage skills using the SIV method.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company. The study was funded by the Universiti Kebangsaan Malaysia, Bangi Selangor, Malaysia (Grant No. UKM-PTS-2013-149).
- Received January 25, 2016.
- Accepted February 12, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.