


Abstract
Objectives: To evaluate the effectiveness of pre-surgical nasoalveolar molding (PNAM) in patients with unilateral cleft lip nasal deformities.
Methods: This was a retrospective study involving 29 patients with unilateral cleft lip and palate defects, of whom 13 were treated with palatal devices with nasal stents (PNAM group) and 16 were treated with palatal devices without nasal stents or surgical tapes (control group). Submental oblique photographs and orthodontic models were longitudinally obtained at the initial visit (T1) and immediately before (T2) and after cheiloplasty (T3). Asymmetry of the external nose, degree of columellar shifting, nasal tip/ala nose ratio, nasal base angle, interalveolar gap, and the sagittal difference in the alveolar gap were measured. The study was conducted in the Orthodontic Clinic at Tokushima University Hospital, Tokushima, Japan between 1997 and 2012.
Results: At T1, there were no significant intergroup differences in the first 4 asymmetry parameters. At T2, the PNAM group showed a significant improvement in all values compared to the control group. At T3, the PNAM group showed significant improvement in nasal asymmetry and columellar shifting. Model analysis showed significantly greater changes in the inter-alveolar gap and the sagittal difference of the alveolar cleft gap from T1 to T2 in the PNAM group.
Conclusion: The use of PNAM is indispensable for pre-surgical orthodontic treatment at the early postnatal age.
Cleft lip and palate (CLP) is the most common structural abnormality in the embryonic period of life, with an incidence of approximately one per 500-700.1-4 Generally, the medial nasal processes merge with the maxillary processes to form the upper lip and primary palate at the age of 6 weeks prenatally. Failure of the fusion of these prominences can result in unilateral and bilateral cleft lip and palate deformities, in which the maxilla and premaxilla cannot form a bony union, and the muscle fibers from the maxillary processes do not enter the prolabium.5,6 This induces discrepancies and displacement of the components of the nasomaxillary complex, including the upper lip, alveolus, palate, and nose, and affects various stomatognathic functions, including respiration, mastication, deglutition, and speech. In cases involving unilateral cleft lip and palate (UCLP), the nasal structures are markedly deformed due to outward rotation of the premaxilla on the affected side.7 This causes flattening and inferior displacement of the nasal tip. The deviation of the nasal septum deflects the columella and shifts the nasal base to the unaffected side.8 The lower deformed alar cartilage is depressed and rotated inferiorly.8 Pre-surgical nasoalveolar molding (PNAM) is a non-surgical procedure performed early after birth in CLP patients to normalize the upper lip, alveolus, and nostrils by using a palate device attached to a nasal stent.9 Several benefits of PNAM have been reported in the literature, including the fact that pre-surgical reduction of the alveolar cleft gap helps surgeons to perform successful gingivoperiosteoplasty.10,11 This procedure has been shown to reduce the need for secondary bone grafts during the period of the mixed dentition in more than 60% of the cases studied.12 One more benefit is that the pre-surgical alignment and correction of the deformity in the nasal cartilages minimizes the extent of primary nasal surgery required, thereby minimizing the formation of scar tissue and producing more consistent postoperative results.13 Most studies on PNAM have focused on the maxillary arch, facial growth, and dental development.14-16 However, few reports have longitudinally evaluated the changes in external nose shape during PNAM therapy. The present study aimed to retrospectively evaluate the effect of PNAM therapy on unilateral cleft lip nasal deformity in patients with complete UCLP.
Methods
Patients
Twenty-nine patients with UCLP who visited the Orthodontic Clinic at Tokushima University Hospital, Tokushima, Japan during the period between 1997 and 2012 were included in this study. All patients underwent lip surgery using the triangular flap method at approximately 3 months after birth in the Department of Plastic and Reconstructive Surgery, Tokushima University Hospital, Tokushima, Japan. Inclusion criteria included non-syndromic UCLP and parents’ agreement to pre-surgical infant orthopedics. Exclusion criteria included systemic diseases, facial trauma, or a history of pre-surgical orthopedic treatment or oral surgery in other facilities. Among these 29 patients, 13 visited the hospital from 2004-2012 and received pre-surgical orthopedics using PNAM (PNAM group). The average age of the patients at the time of commencing PNAM therapy was 6.6 weeks (range: 3.3 – 11.6 weeks), and the average duration of PNAM therapy was 11.6 weeks (range: 7.3 – 16.3 weeks). The remaining 16 neonates with UCLP who visited the hospital from 1997 to 2003 and underwent lip surgery without nose correction by a nasal stent were used as controls (control group). All patients in the control group received early orthopedic treatment using an elastic tape and/or a palatal device without a nasal stent. The average age of patients in the control group was 5.5 weeks (range: 1.6 – 11.4 weeks) and the average duration of the pre-surgical treatment was 9.3 weeks (range: 5.0 – 17.3 weeks). The age and gender distribution of subjects in the control group did not differ from those in the PNAM group. This study was approved by the Institutional Ethical Committee of Tokushima University Hospital, and performed according to the principles of Helsinki Declaration.
Design and structure of the PNAM appliance
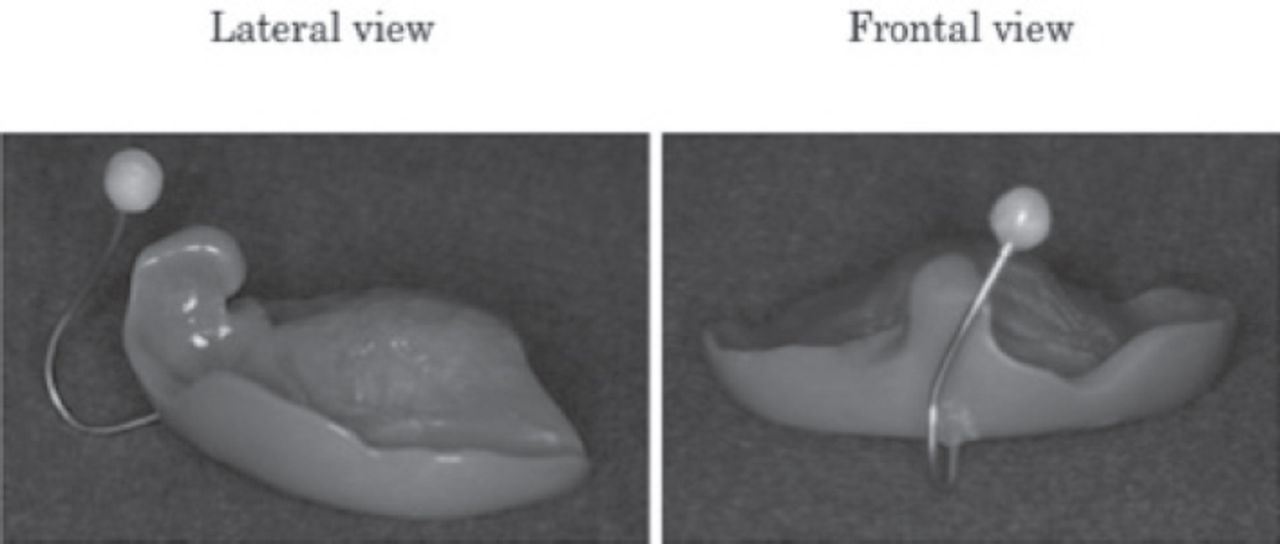
At the initial visit, an intraoral impression of the affected upper jaw was taken with alginate impression material and a working cast was fabricated. On the model, areas where the alveolar ridges were expected to grow during the infant orthopedics, such as the cleft space, were completely blocked out by wax. After this procedure, a palatal device similar to the appliance described by Grayson et al17 was fabricated using low-temperature polymerized burying, heating polymerization model resin (ACRONTM, GC, Tokyo, Japan) (Figure 1). Furthermore, a nasal stent wire, 0.8 mm in diameter, was embedded into the palatal device and emerged through its labial vestibular flange at the medial edge of the greater segment for nasal stent fabrication. At the initial visit, surgical tape was applied to the infant’s face to simulate the continuous orbicularis oris muscle band for molding the alveolar segments. The palatal device was set approximately one week later. After checking the fit of the plate and the feeding condition, a nasal stent wire was bent, and a nasal bulb, made of polymerization resin, was added to mold the nasal cartilage and nasal dome until mild blanching of the skin over the bulb was observed. The palatal device was held by surgical tape across the upper lip. The molding plate was adjusted every 2 weeks to gradually approximate the alveolar segments and to reduce the alveolar gap. At the same time, the stent was repositioned inside the nose underneath the apex of the alar cartilage on the cleft-affected side, so that the nostril was lifted to become symmetric. For both groups, the surgical tape was continuously used to support the palatal device wear and to draw the upper lip. Parents were instructed to change the tape every day and to keep the appliance in place at all times except during cleaning.

Palatal plate with nasal stent. Palatal plate with a nasal stent wire with 0.8 mm-diameter extended from the labial flange of the plate.
Photographic and model analyses
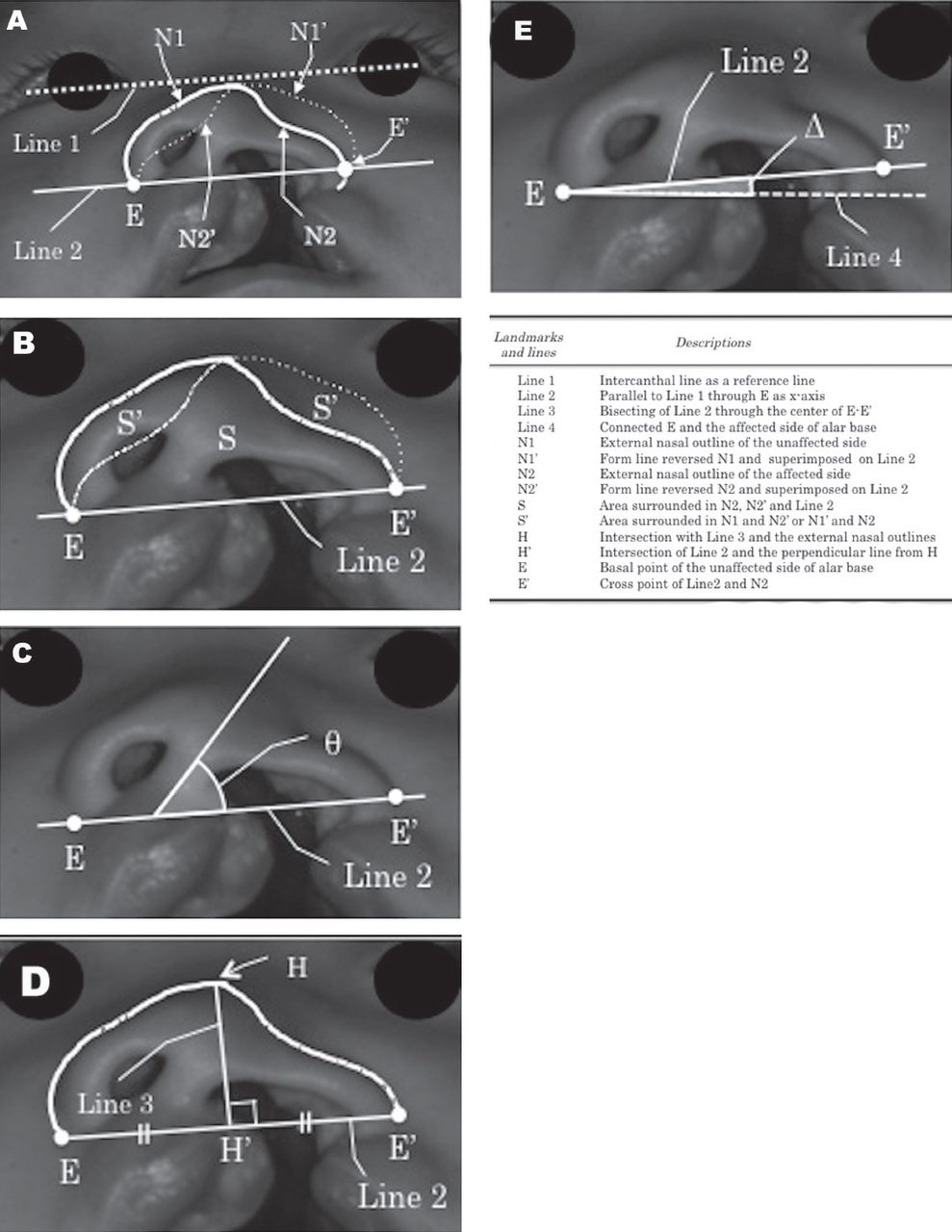
Submental oblique photographs, including those of the medial angle of eye, were taken at the initial visit (T1) and immediately before (T2) and after cheiloplasty (T3), and were used to assess the asymmetry of the external nose, the columellar angle, the nasal tip/ala nose ratio, and the nasal base angle.18 A mirror-image analysis was performed to objectively quantify the degree of nasal asymmetry and deformity. The landmarks used for measurement are depicted in Figure 2. On the tracing, the basal point of the unaffected side of the alar base (E) and the external nasal outlines of the unaffected (N1) and affected (N2) sides were defined, and 4 lines are drawn: Line 1 connecting both medial ocular angles was drawn as a reference line, Line 2 was drawn parallel to Line 1 through E as the x-axis, and the intersection point of Line 2 and N2 was defined as E’. Line 3 was perpendicular to Line 2 through the middle point between E and E’, and the intersection point of Line 3 and the external nasal outline (N1 or N2) was defined as H. Line 4 was connected at E and the affected side of the alar base. Furthermore, the external nasal outlines N1 and N2 were mirrored along Line 3, and the mirror drawings were then superimposed over the opposite side, indicating N1’ and N2’.

Construction of landmarks and lines used in the photographic analysis for unilateral cleft nose deformity. A) Definitions of landmarks and reference lines; B) Symmetry of the external nose was defined as a ratio of cross-sectional areas, S and S’, and calculated from the following formula: (S + 2S’)/S; C) Angle of columella was determined as an angle made by the columellar axis (median line of columella) and Line 2; D) The nasal tip/ala nose ratio was defined as a ratio of the nasal height (HH’) to nasal width (EE’); E) Angle of the nasal base was defined as an angle between Line 2 and Line 4.
The symmetry of the external nose was defined as the ratio of the cross-sectional areas, S and S’, and calculated using the following formula: (S + 2S’)/S, where the area S’ was surrounded by the two lines N1 and N2’ and the area S was surrounded by the three lines N2, N2’, and Line 2. This measurement characterizes the degree of nasal form asymmetry. If the nasal form is perfectly symmetrical, the value of this measurement is almost one. The columellar angle (q) is defined as an angle made by Line 2 and the columellar axis. This measurement characterizes the inclination of the columella. If the value of q is almost 90 degrees, there is little deviation. The nasal tip/ala nose ratio was defined as the ratio of the nasal height to the nasal width. Here, the nasal height was the vertical distance from H to Line 2 where the intersection between Line 2 and Line 3 was defined as H’, and the width of the external nose was the distance between E and E’. If the nasal form is morphologically good, the value of this measurement is high. The angle of the nasal base (Δ) was defined as an angle between Line 2 and Line 4. Therefore, the nostrils become more symmetric as the value of this Δ is almost 0 degree.
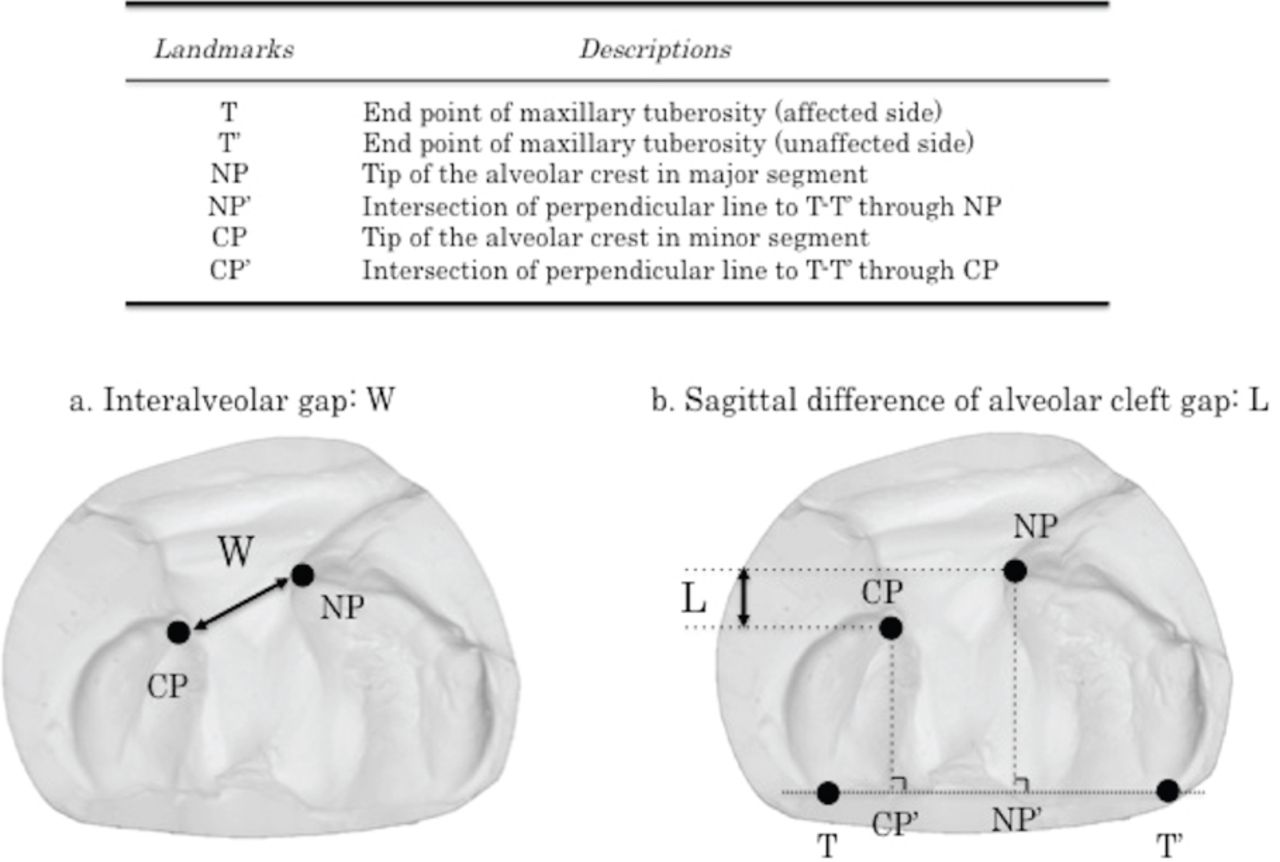
On the intraoral casts taken at T1 and T2, the 3 reproducible reference mucosal points were defined on the basis of the findings in Kramer et al.19 (Figure 3). One line connecting the bilateral tuberosity points (T and T’) was drawn as a reference line. Among the 2 points, the NP point indicates the tip of the alveolar crest in the major segment, while the CP point was defined as the tip of the alveolar crest in the minor segment. The interalveolar gap (W) is the distance between NP and CP. Two more lines were drawn perpendicular to the reference line (T-T’) through the NP and CP points, and intersected the reference line at NP’ and CP’, respectively. The sagittal distances were measured as the distances between NP and NP’ and between CP and CP’, and the sagittal difference of the alveolar cleft gap (L) was calculated as the sagittal distance of NP-NP’ minus CP-CP’.

Landmarks and linear measurements for model analysis. A) The measurements of the interalveolar gap (W) was determined as the distance between NP and CP. B) The sagittal difference of alveolar cleft gap (L) was determined as the difference of NP-NP’ and CP-CP’.
To eliminate inter-examiner errors and ensure standardization, all measurements were made by one investigator (N.K.). Intra-examiner reliability was calculated by measuring all variables twice 2 weeks apart.
Statistical analysis
The data were not normally distributed, and accordingly, non-parametric tests were used in this study. The collected research data consisted of 29 data points for T1, 21 data points for T2, and 28 data points for T3. To detect the effectiveness of PNAM treatment for the external nasal form, mean values were compared between the control and PNAM groups at T1, T2, and T3 using the Mann-Whitney U test. Mean values of the same group were compared between T1 and T2 to observe the advantage of the treatment before surgery using Wilcoxon signed-rank test. To detect the effectiveness of PNAM treatment for the disrupted arch form, mean values were compared between the control and PNAM groups at T1 and T2 using the Mann-Whitney U test. Mean values of the same groups were compared between T1 and T2 to observe the advantage of treatment before surgery using the Wilcoxon signed-rank test. Probability less than 0.05 was considered significant. The analyses were performed using a statistical analysis software (StatView; SAS Institute, Cary, NC, USA) and the paired t-test was used to measure intra-examiner reliability by comparing all the variables that were measured twice 2 weeks apart. The casual error was calculated according to Dahlberg’s formula (Se2Sd2/2n), where Se2 was the error variance, d was the difference between the repeated measurements, and n was the number of double measurements made.20 According to Dahlberg’s formula, the mean error ranged from 0.03-0.23 mm for the linear measurements and from 0.19-1.20 degrees for the angular measurements.
Results
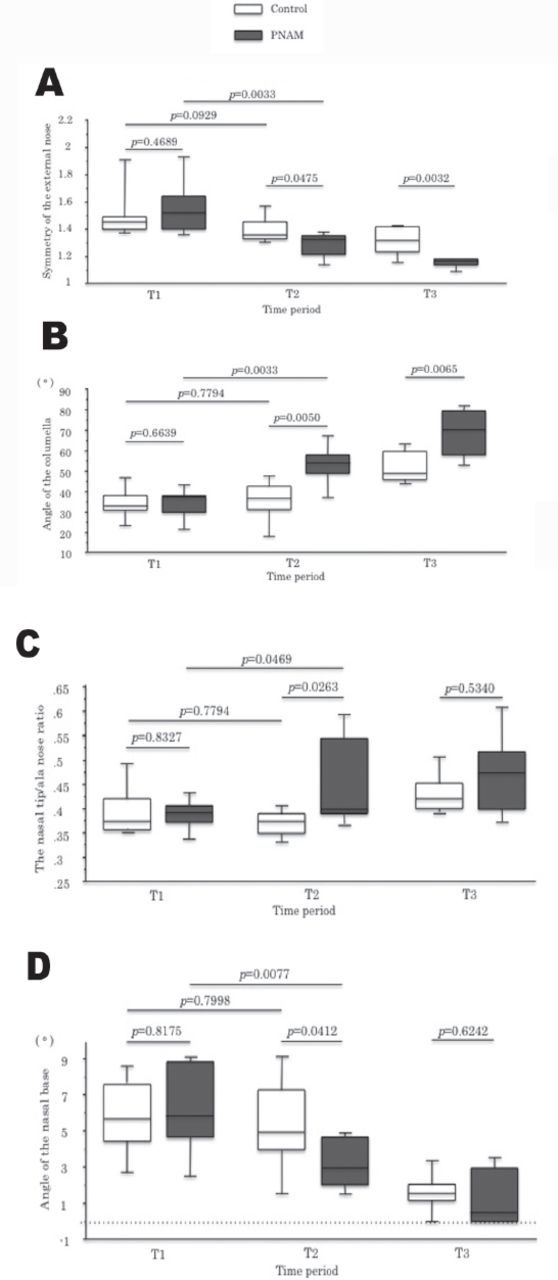
In the photographic analysis at T1, the values for asymmetry of the external nose (p=0.4689), the columellar angle (p=0.6639), the nasal tip/ala nose ratio (p=0.8327), and the angle of the nasal base (p=0.8175) showed no significant differences between the PNAM and control groups (Figure 4). This indicates that the severity of the nasal deformity was similar between the 2 groups.
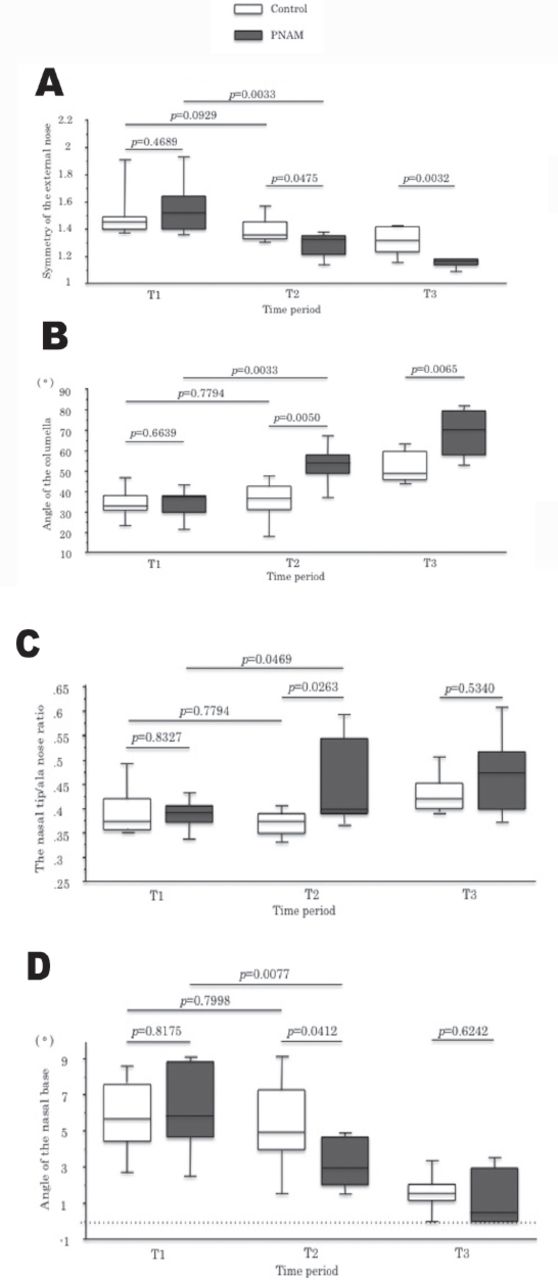
Changes in external nasal form at 3 different time points. A) Symmetry of the external nose; B) Angle of the columella; C) The nasal tip/ala nose ratio; D) Angle of the nasal base. T1 - initial visit (N=29), T2 - immediately before cheiloplasty (N=21), T3 - after cheiloplasty (N=28).
In assessments of the asymmetry of the external nose, mean values in the control group did not show significant differences (p=0.0929) between T1 and T2, while those in the PNAM group showed a significant decrease (p=0.0033) between T1 and T2, indicating a preoperative improvement in the nasal form asymmetry after PNAM treatment (Figure 4a). Furthermore, the mean values of the PNAM treatment group showed a significant decrease when compared to those of the control group at T2 (p=0.0475) and T3 (p=0.0032). These results indicate the effectiveness of PNAM treatment in improving nasal form asymmetry before and after surgery.
In assessments of the collumellar angle, the mean values in the control group did not show significant differences (p=0.7794) between T1 and T2, while those in the PNAM group showed a significant improvement (p=0.0033) between T1 and T2, indicating a preoperative improvement in the collumellar angle after PNAM treatment (Figure 4b). Furthermore, the mean values in the PNAM treatment group showed a significant increase compared with those in the control group at T2 (p=0.0050) and T3 (p=0.0065). These results emphasize the effectiveness of PNAM treatment in improving the collumellar angle before and after surgery.
In assessments of the nasal tip/ala nose ratio, the mean values in the control group did not show significant differences (p=0.7794) between T1 and T2 (Figure 4c). The mean values in the PNAM treatment group showed a significant improvement (p=0.0263) when compared to those in the control group at T2. However, the mean values in the PNAM treatment group did not show a significant improvement (p=0.5340) when compared to those in the control group at T3.
In assessments of the angle of the nasal base, the mean values in the control group did not show significant differences (p=0.7998) between T1 and T2, while those in the PNAM group showed significant improvement (p=0.0077) between T1 and T2 (Figure 4d). The mean values in the PNAM treatment group showed significant improvement (p=0.0412) when compared to those in the control group at T2. However, the mean values in the PNAM treatment group did not show significant improvement (p=0.6242) when compared to those in the control group at T3. These results suggest that PNAM treatment is effective in improving the nasal tip/ala nose ratio and the angle of the nasal base before the surgery but did not offer any advantages after surgery.
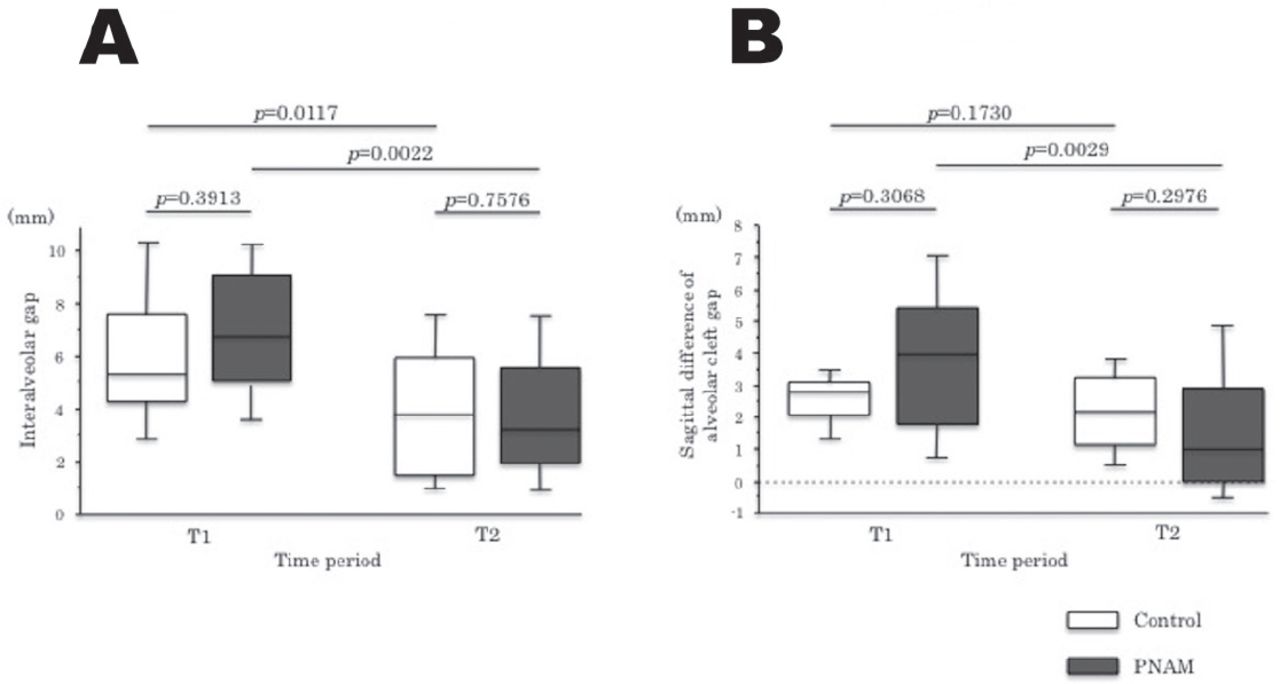
In the model analysis, the inter-alveolar gap showed no significant differences between the 2 groups at T1 (p=0.3913) and T2 (p=0.7576); however, the change in values from T1 to T2 were significantly decreased in the control (p=0.0117) and PNAM groups (p=0.0022) (Figure 5a). The sagittal difference in the alveolar cleft gap was also similar between the 2 groups at T1 (Figure 5b). From T1 to T2, the value of the sagittal difference significantly decreased (p=0.0029) in the PNAM group, although the values at T2 showed no significant difference (p=0.2976) between the 2 groups. This indicates that the basic orthopedic treatment is effective to improve the inter-alveolar gap and the nasal stent has advantages to the sagittal difference of alveolar gap.
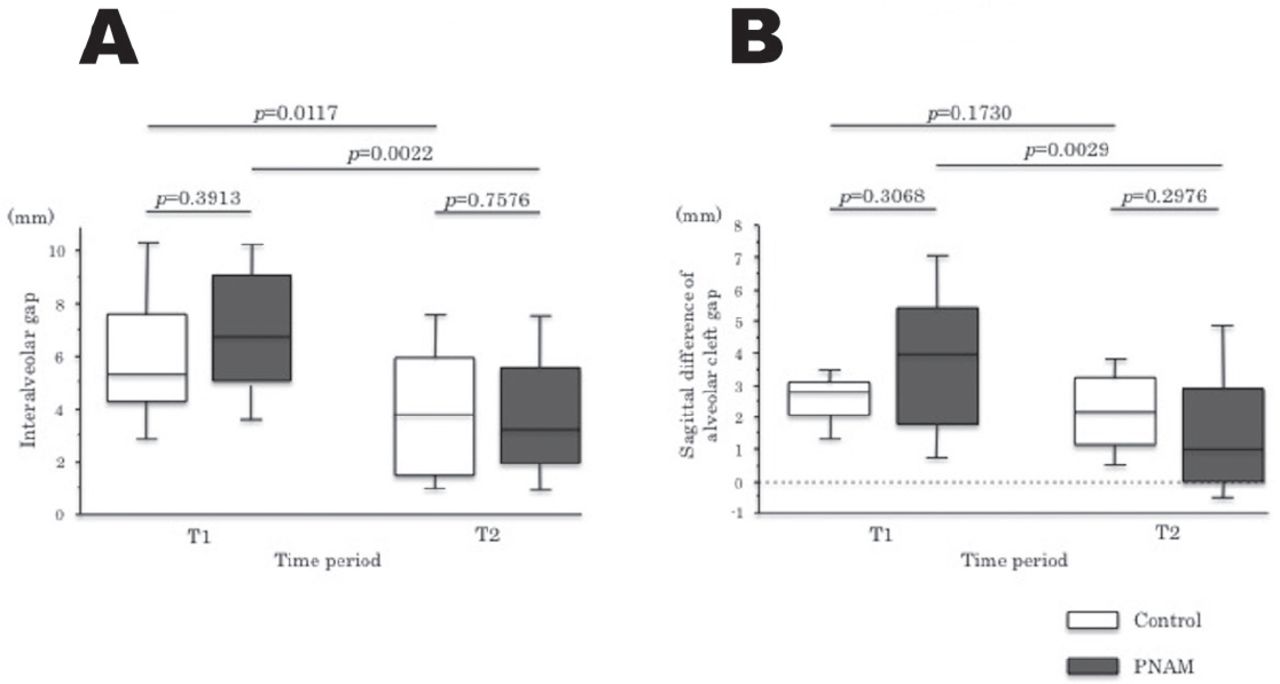
Changes in the disrupted arch form at the 2 different time points. A) Interalveolar gap (W); B) Sagittal difference of alveolar cleft gap (L). T1 - initial visit (N=29), T2 - immediately before cheiloplasty (N=21).
Discussion
We assessed the effectiveness of PNAM in pediatric patients with UCLP and found that the use of PNAM before surgery led to noticeable preoperative improvements in the asymmetry of the external nose, the columellar angle, the nasal tip/ala nose ratio, and the angle of the nasal base. Pre-surgical nasoalveolar molding also had beneficial effects on the asymmetry of the external nose and the collumellar angle after surgery.
There are many proponents of early correction of the cleft lip and nose. McComb21 reported that if the alar cartilages are not corrected during primary repair, the dome becomes “tethered” by its adhesion to the nasal lining, which makes it more difficult to correct in a later procedure. Broadbent and Woolf22 demonstrated that an unrepaired nasal deformity can worsen over time.22 Conversely, a well-performed repair of the nasal form at an early life is likely to maintain throughout growth and retain long-term esthetics.23,24
Nasal stenting has been used for maintenance of the alar cartilage form in clefts with stenosis.25-28 Matsuo et al29 demonstrated that the auricular cartilage could be molded with permanent results if the treatment was started within the first 6 weeks of life, due to the high degree of plasticity in the cartilage of infants during that period. They attributed this finding to the high levels of hyaluronic acid, which is a component of the proteoglycan aggregate of the intercellular matrix, in the cartilage.30 Thus, early soft tissue and cartilage molding plate therapy is most successful over the first 3-4 months of life postnatally. This led Matsuo and Hirose to emphasize the idea of correcting the nostril form symmetrically before primary lip repair.31 In addition, PNAM may minimize the amount of dissection of the cartilage, thereby reducing scarring and relapse. An additional benefit of the PNAM technique is the non-surgical “lip adhesion”. Maintaining the apposition of lip segments by using elastic tape not only enables better control of the orthopedic force to close of the cleft, but also facilitates traditional lip adhesion without a large scar after surgery, which may further interfere with secondary nasal correction.24
The average age to start PNAM therapy is the 26th day after birth and the average treatment period of PNAM is 110 days.32 In this study, PNAM therapy was started at 49.7 days after birth, on average. This is almost at the end of the ideal cartilage molding period, which was reported by Matsuo et al29 to occur over the first 6 weeks of life.29 On the other hand, the treatment period was 91.7 days, which is almost the same as that reported previously.33-35 Although the period of PNAM therapy was shorter in our study, a significant positive change was achieved. If nasal stenting was started a little earlier, the duration of PNAM use would have been longer and a more prominent effect might have been achieved.
The effectiveness of molding plate therapy is enhanced by adequately supporting the appliance against the palatal tissues and by taping the lip segments together across the cleft. A previous report demonstrated improved asymmetry of the nose only by taping.13 Thus, maintaining tight apposition of lip segments with tape is assumed to be more beneficial than the traditional lip adhesion, without consequent scarring. The lip adhesion alone produces uncontrolled orthopedic effects, whereas the lip-tape adhesion combined with the molding plate produces controlled movement of the alveolar segments.13 Moreover, taping of the cleft lip segments also serves to improve the alignment of the nasal base region by bringing the columella toward the midsagittal plane and expanding the nasal tip to project upward. This improvement in soft tissue position serves to reduce the complexity of the surgical repair. In addition, there may be a reduction in the need for alveolar bone grafting.
The advantages of PNAM may be considered from a soft tissue perspective as well as from the usual osseous perspective.36,37 One of the advantages of PNAM is the moldability of alveolar processes to guide the segments into a normal position. In addition, pre-surgical reduction of the alveolar cleft gap facilitates the performance of gingivoperiosteoplasty due to the probability of forming an osseous bridge. Ross and MacNamera38 advocated another possible benefit of presurgical infant orthopedics. As the maxillary segments are guided to the normal position, the lip segments come closer, thereby making cheiloplasty simpler to perform.
In this study, the nasal form of both groups with UCLP patients obviously showed asymmetry in terms of the columellar angle and the height at T1. The measurements related to nostril symmetry improved after PNAM therapy and immediately before cheiloplasty (T2) and the external nasal form of that group remained in good condition one month after cheiloplasty (T3). The columella was upright and the cartilages maintained a normal convexity. The contour of the nostril on the cleft-affected side was fashioned to nearly resemble the nostril on the unaffected side as the alar tissue was molded into a normal convex shape. Although these changes resulted in an improved nasal tip projection and alar cartilage symmetry, the measurements related to nasal base in the PNAM group did not show statistical significance at T3. This can be attributed to several factors; the small sample size used in this study, the insufficient overcorrection of the nasal base, and the postoperative contracture of the subsequent tissues. Although the nasal alar was adequately repositioned by PNAM before cheiloplasty, it seemed to have gradually subsided postoperatively into the original position by the alveolar bone defect, resulting in a relapse of the nostril form.
Furthermore, considering the reported correlation between the area of the nasal cavity bottom and the sagittal level of both major and minor segments, we examined the sagittal difference in the alveolar cleft gap using a study model.39,40 The PNAM therapy significantly reduced the discrepancy in the sagittal level of both major and minor segments (NP-CP), which was not seen in the control group. In PNAM, the force exerted by the nasal stent to lift the nasal cavity is assumed to act as an anchor. In other words, the elevation of the nasal soft tissue results in an intraoral molding force against the alveolar segments that is conducted down the nasal stent. This force facilitated more effective molding of the alveolar segments, and the major segment was modified by decreasing its projection and outward rotation. On the other hand, the minor segment was advanced in antero-medial direction, thereby normalizing the contour of the dental arch. Furthermore, in accordance with the decrease of alveolar cleft width, a significant reduction of columella deviation and an increase of nostril height were observed as a result of the appropriate use of PNAM. When the alveolar cleft width has been reduced to less than 6 mm, it was better to add the nasal stent to the molding plate appliance so that nasal cartilage molding may begin.36 Adding the nasal stent to correct the nasal cartilage deformity before the reduction of the alveolar cleft width to less than 6 mm may cause unfavorable results such as the lengthening of the circumference of the alar of the nose.13 For this reason, a severe alveolar deformity is generally reduced before altering the position of the nasal tip with a nasal stent. A previous study reported that a significant difference of width of alveolar gap was not seen over time in patients treated with or without PNAM.41 In the present study, we demonstrated successful treatment in patients with an alveolar cleft gap of more than 6 mm by PNAM. More successful results may be obtained when a smaller cleft remains between the alveolar ridges.
There were several limitations to this study. The sample size of the present study was not adequate to draw strong conclusions about PNAM. Therefore, high-quality clinical studies using sufficient samples and more sophisticated methodology are needed to estimate the efficacy of PNAM in improving cleft nasal deformity and their long-term stability.
The present study quantitatively demonstrated improvements in the nasal form of UCLP patients treated with PNAM. The incidences of a depressed dome, wide alar width, deficient columella, and alveolar malposition were greatly reduced in the PNAM group but persisted in the control group. In addition, it was notable that the external nasal form of patients in the PNAM group was maintained in good condition after the primary lip surgery. Based on these findings, we suggest that PNAM therapy is effective not only for induction of dental alveolar growth but also as a presurgical orthodontic treatment for improvement of the nasal form and the treatment result after the primary lip surgery. Although it is necessary to evaluate the long-term stability of these effects, it can still be concluded that the use of PNAM is desirable during the postnatal period when the nasal cartilages show high plasticity, and that this approach would provide good nasal forms in patients with UCLP.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company. This work was supported by Japan Society for the Promotion of Science KAKENHI, Tokyo, Japan Grant Number 26293436 (E.T.).
- Received September 5, 2017.
- Accepted December 18, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.