


Article Figures & Data
Figures
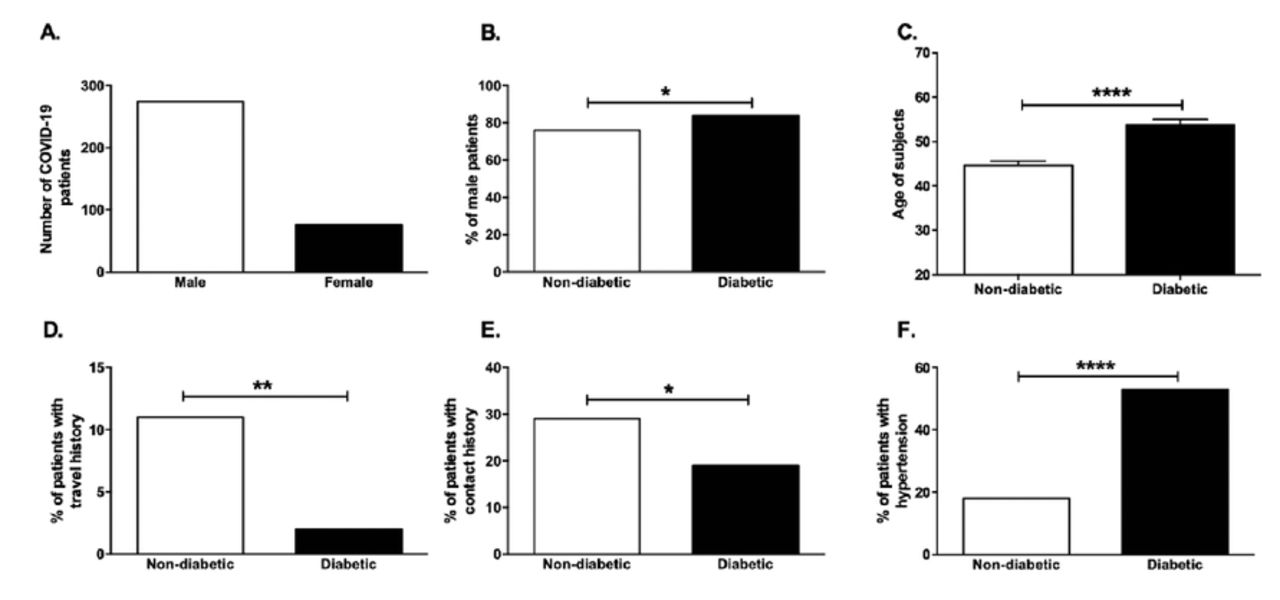
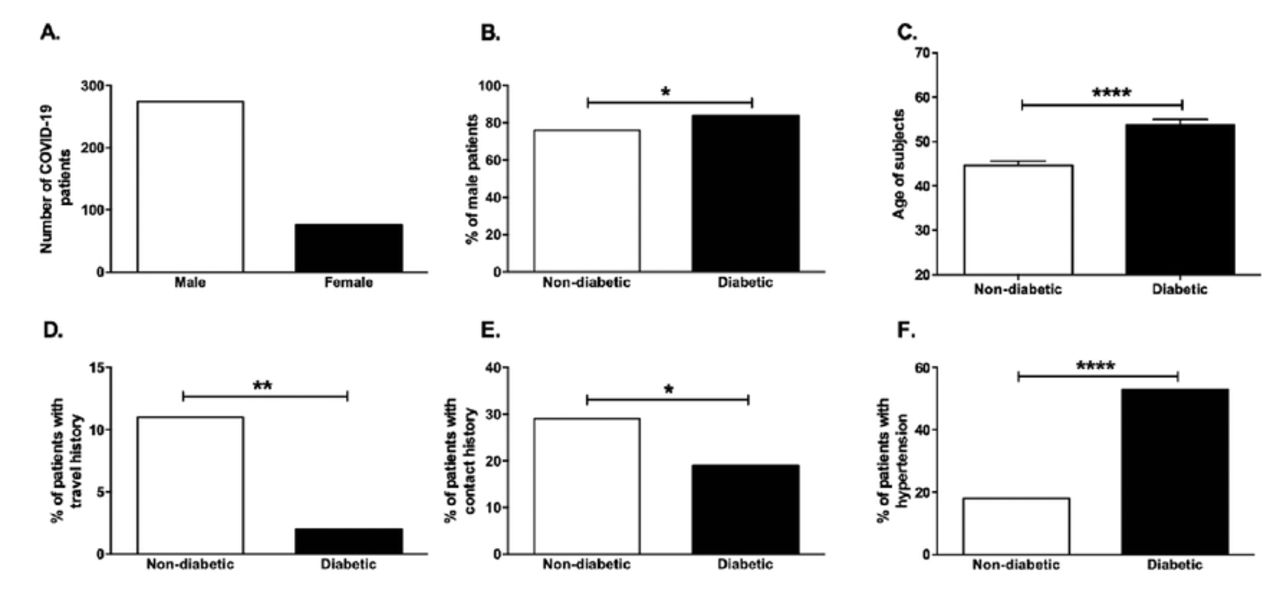
- Figure 1.
- Gender, age, and risk factors associated with COVID-19 infection. Bar graph showing A) the number of male and female of COVID-19 positive patients, B) the percentage of male subjects in the diabetic and non-diabetic COVID-19 patients. C) Age, D) travel history, E) contact history were compared between diabetic and non-diabetic COVID-19 patients. F) percentage of patients with hypertension. *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001
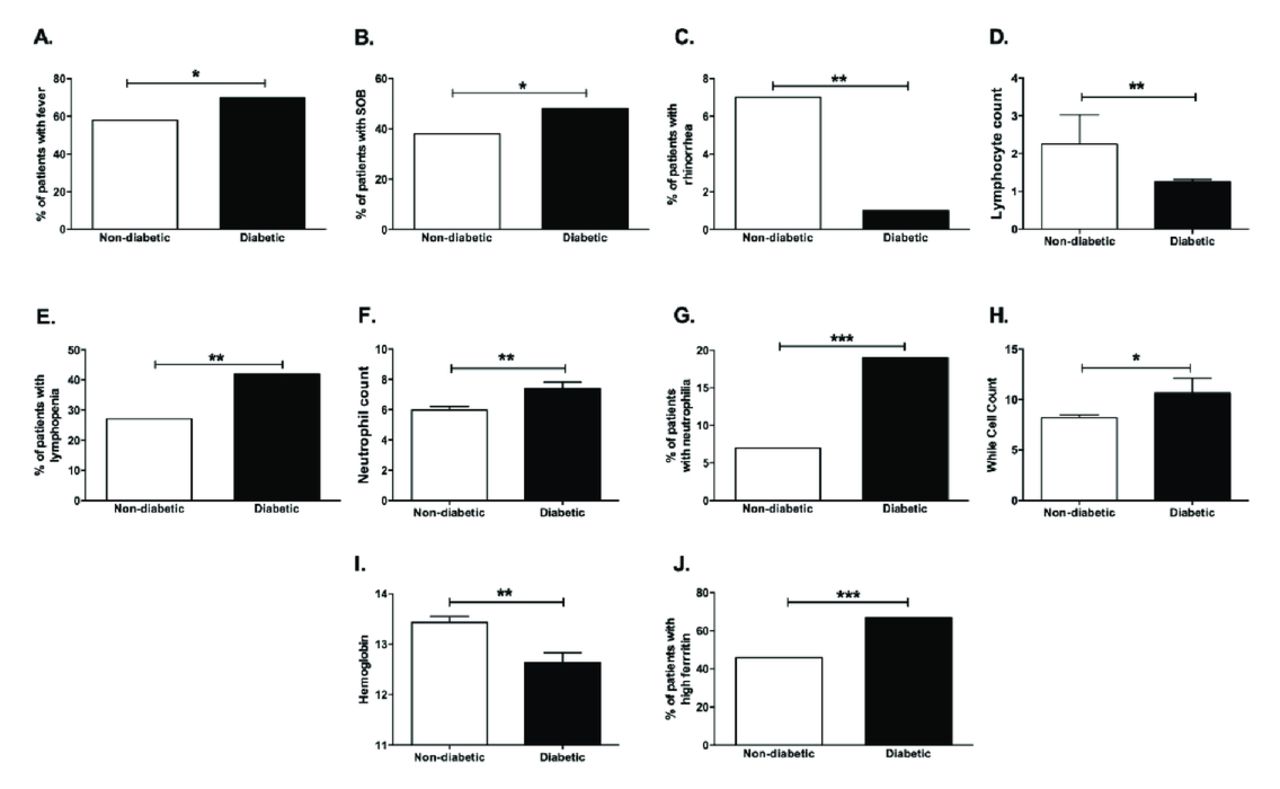
- Figure 2.
- Clinical symptoms and blood laboratory tests of COVID-19 subjects. Percentage of COVID-19 patients with A) fever, B) shortness of breath (SOB), C) rhinorrhea in diabetic and non-diabetic groups. D) Lymphocyte count, E) percent of patients with lymphopenia, F) neutrophil count, G) percent of patients with neutrophilia, H) white cell count (WCC), I) hemoglobin, J) percent of patients with high ferritin were compared between diabetic and non-diabetic COVID-19 patients. *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001
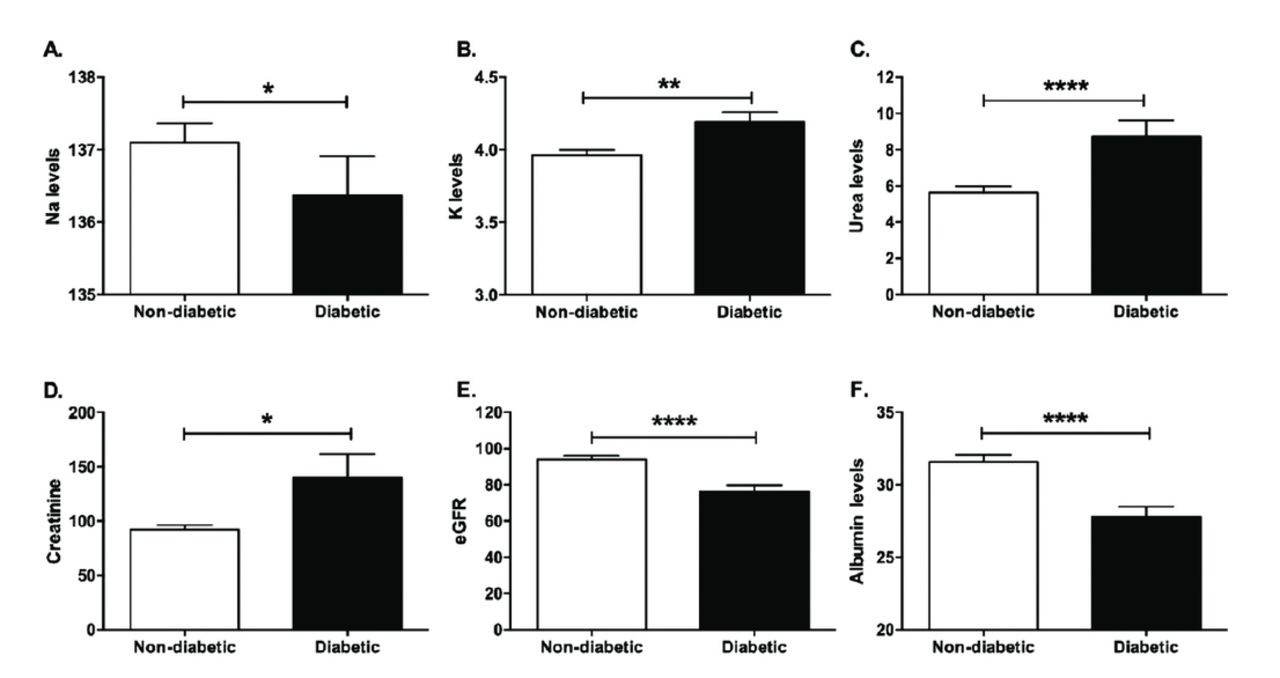
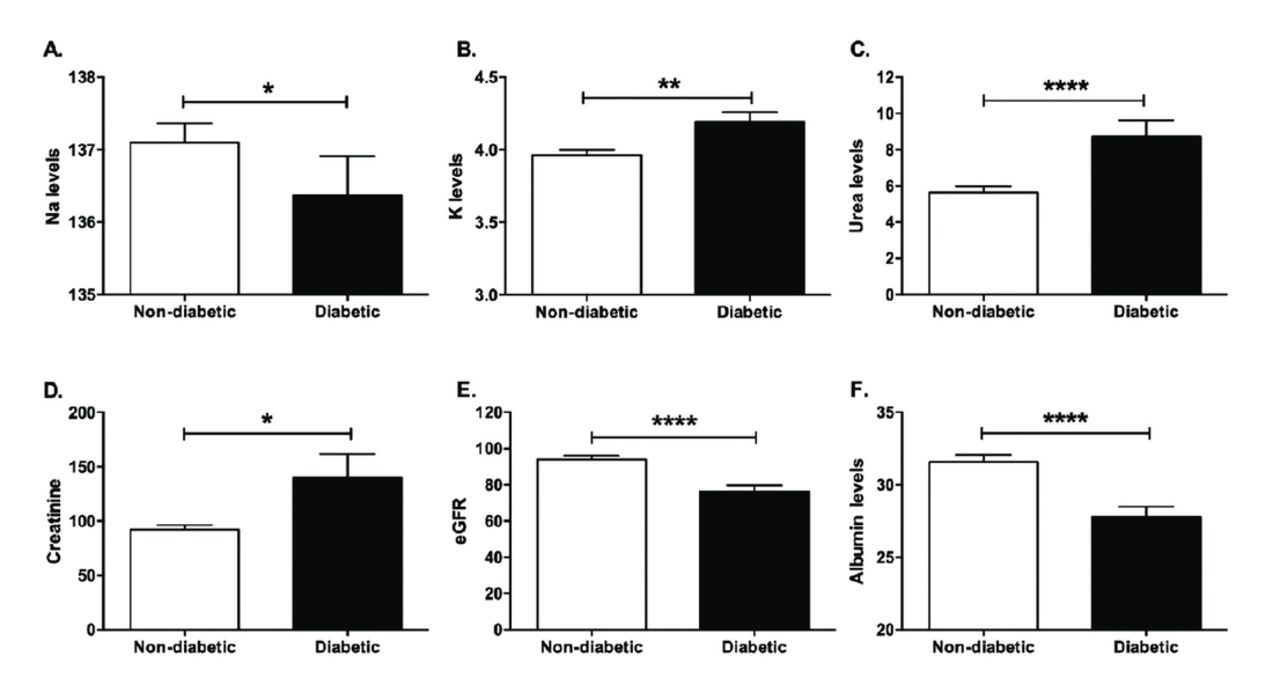
- Figure 3.
- Renal and liver function blood tests in COVID-19 subjects. A) sodium: Na levels, B) potassium: K levels, C) urea D) creatinine E) eGFR, and F) albumin were compared in the diabetic and non-diabetic groups. * p<0.05, ** p<0.01, *** p<0.001, ****p<0.0001
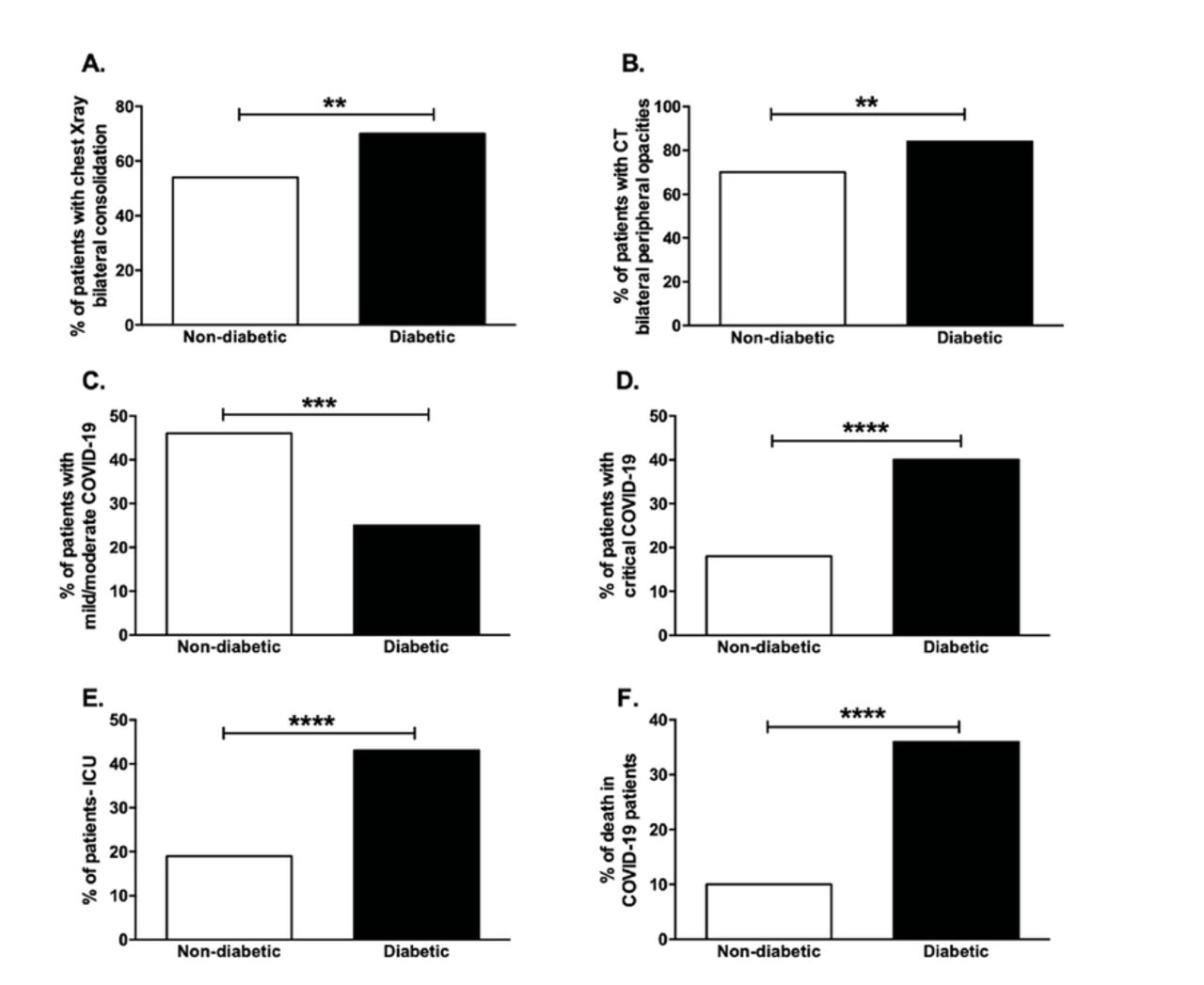
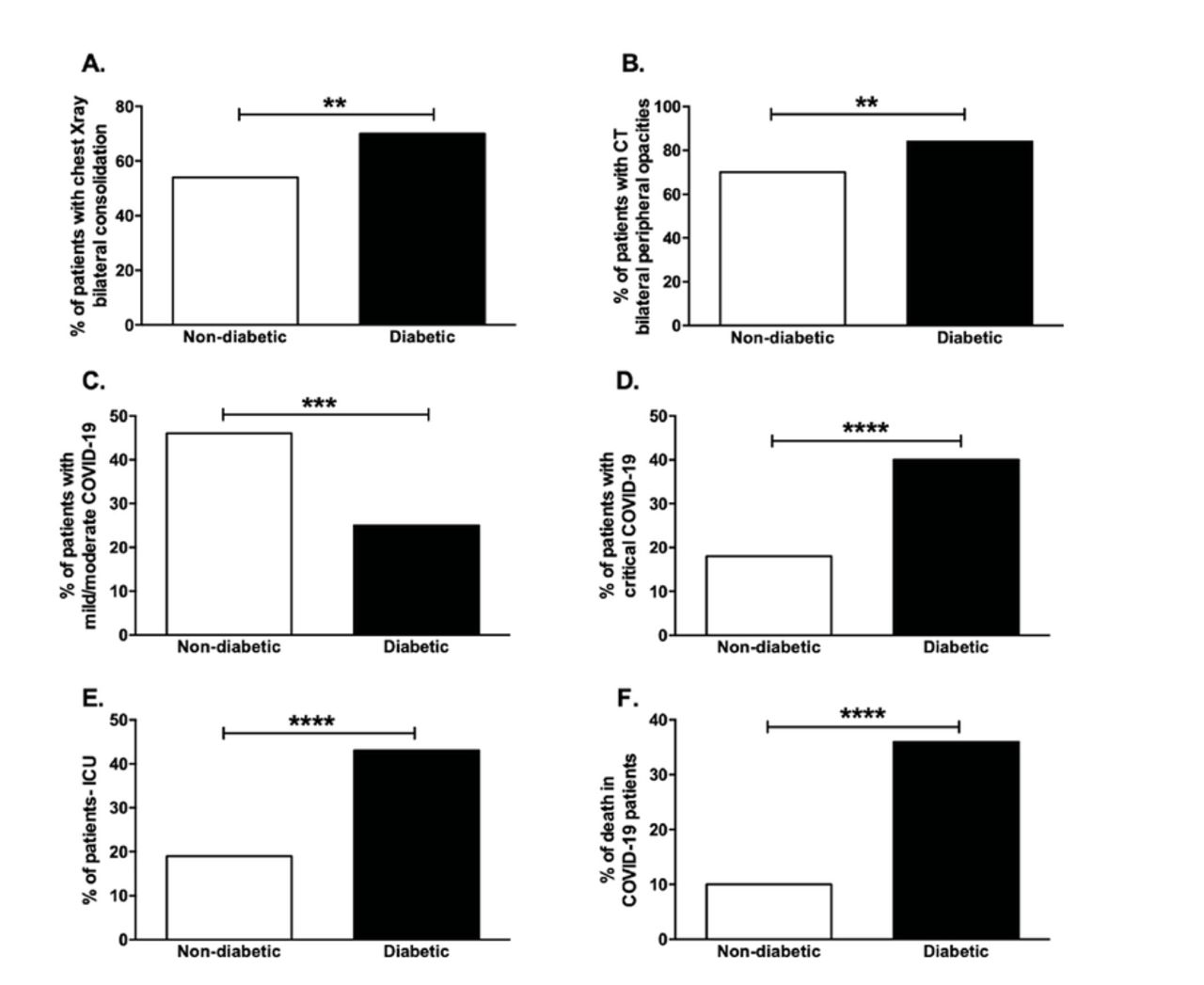
- Figure 4.
- Radiological assessment and clinical outcomes of diabetic COVID-19 patients. The percentage of patients with A) chest x-ray showing bilateral consolidation and B) CT scan showing bilateral peripheral ground-glass opacities was compared in diabetic and non-diabetic COVID-19 patients. The percentage of COVID-19 patients with C) mild/moderate and D) critical clinical outcome as well as the percentage of E) those admitted to ICU and F) death in COVID-19 were compared in diabetic and non-diabetic groups *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001
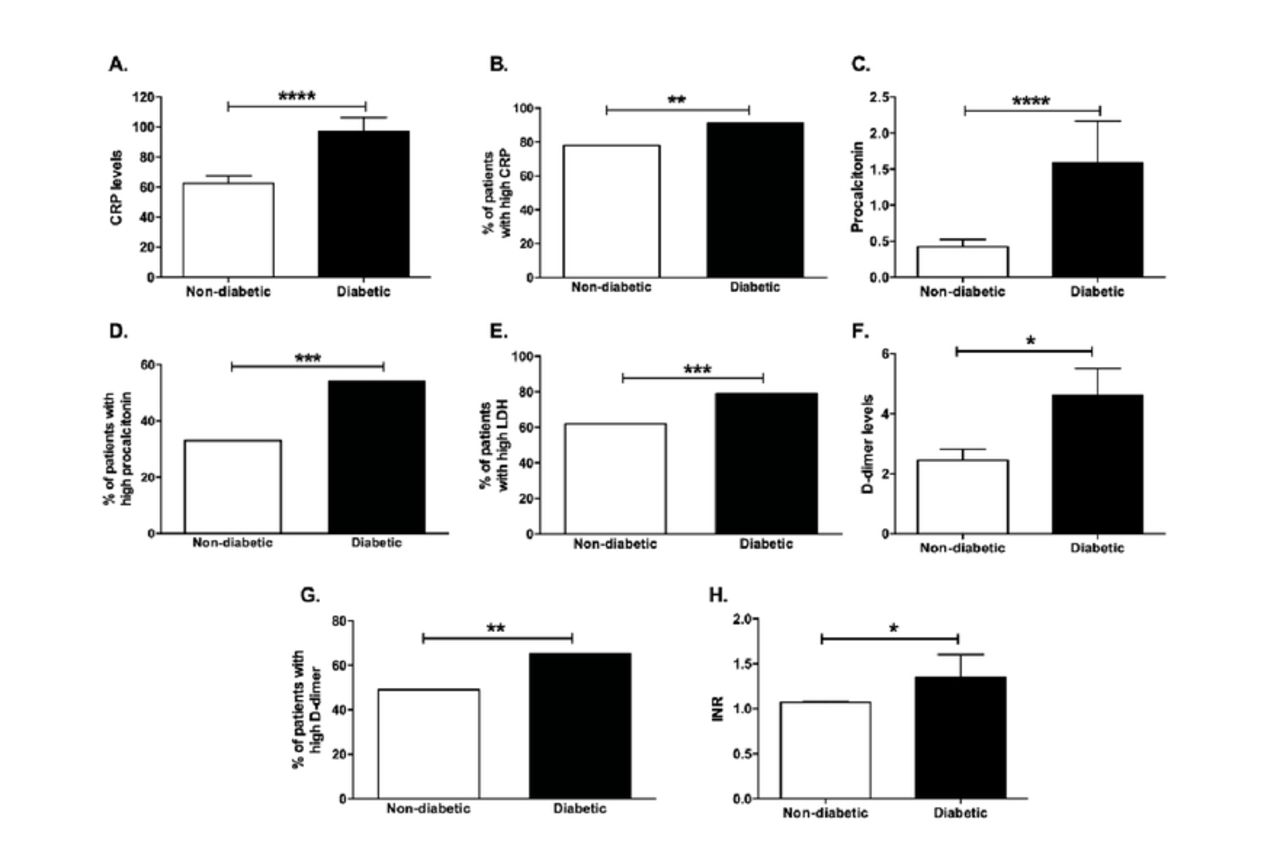
- Figure 5.
- Disease severity and coagulation markers in COVID-19 patients. A) CRP, C) procalcitonin, F) D-dimer, and H) INR levels in diabetic and non-diabetic COVID-19 patients. The percentage of patients with B) high CRP, D) high procalcitonin, E) high LDH, and G) high D-dimer in diabetic compared to non-diabetic COVID-19 patients. *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001


Tables
- Table 1.
- Demographic data and comorbidities of the diabetic and non-diabetic COVID-19 patients included in the study.
Variables Non-diabetic COVID-19 (n=239) Diabetic COVID-19 (n=111) P-value Demographic data Gender (M/F) 181/58 93/18 0.045 Age at diagnosis 44.64 ± 14.38 53.73 ± 12.79 <0.0001 Travel history (yes/no) 26/212 2/109 0.002 Contact history (yes/no) 69/170 21/89 0.026 Risk factors and comorbidities Old age (yes/no) 44/195 40/71 0.0002 CVD (yes/no) 7/232 6/105 0.127 HTN (yes/no) 43/196 58/52 <0.0001 Prior stroke (yes/no) 2/237 1/110 0.476 Cancer (yes/no) 2/237 0/111 0.167 Chronic lung disease (yes/no) 9/230 2/109 0.164 CKD (yes/no) 5/234 1/110 0.212 CKD: chronic kidney disease, CVD: cardiovascular disease, HTN: hypertension
- Table 2.
- Clinical symptoms, disease severity markers, and radiographic data of the diabetic and non-diabetic COVID-19 patients included in the study.
Symptoms/disease severity markers Non-diabetic COVID-19 patients (n=239) Diabetic COVID-19 patients (n=111) P-value Symptoms Fever (yes/no) 139/100 78/33 0.015 Cough (yes/no) 131/108 64/47 0.309 Fatigue (yes/no) 15/224 6/105 0.375 Anorexia (yes/no) 6/223 3/108 0.458 Shortness of breath (yes/no) 90/149 53/58 0.037 Sputum production (yes/no) 3/236 0/111 0.118 Myalgias (yes/no) 23/216 14/97 0.199 Headache (yes/no) 20/219 4/107 0.0504 Rhinorrhea (yes/no) 16/223 1/110 0.0095 Sore throat (yes/no) 24/215 10/101 0.381 Vomiting (yes/no) 6/233 3/108 0.458 Diarrhea (yes/no) 11/227 6/105 0.376 Nausea (yes/no) 6/233 2/109 0.34 Anosmia (yes/no) 1/238 1/110 0.289 Ageusia (yes/no) 1/238 0/111 0.248 Disease severity markers CRP 62.45 ± 79.65 97.23 ± 96.39 <0.0001 High CRP (>3) (yes/no) 185/52 101/10 0.002 D-dimers 2.449 ± 5.062 4.612 ± 9.093 0.042 High D-dimers (>0.5) (yes/no) 118/121 72/39 0.004 LDH 398.8 ± 353.2 409.8 ± 264.1 0.197 High LDH (>227) (yes/no) 144/89 87/23 0.0007 Procalcitonin 0.4242 ± 1.474 1.587 ± 5.974 <0.0001 High procalcitonin (>0.1) (yes/no) 79/159 59/51 0.0001 Ferritin 1028 ± 1277 1207 ± 1938 0.188 High ferritin (>388) (yes/no) 111/128 74/37 0.0002 Radiographic data Chest x-ray: bilateral airspace consolidation (yes/no) 120/104 72/31 0.003 CT chest: bilateral peripheral ground glass opacities (yes/no) 152/66 76/15 0.0060 CRP: C-reactive protein, LDH: lactate dehydrogenase
- Table 3.
- Blood, renal, and liver tests of the diabetic and non-diabetic COVID-19 patients included in the study.
Tests Non-diabetic COVID-19 patients (n=239) Diabetic COVID-19 patients (n=111) P-value Blood tests Neutrophil count 5.971 ± 3.808 7.395 ± 4.567 0.002 Neutrophilia (>14) (yes/no) 17/222 21/90 0.0005 Lymphocyte count 2.255 ± 11.83 1.256 ± 0.6693 0.006 Lymphopenia (<1) (yes/no) 65/174 47/64 0.003 Hb 13.43 ± 1.839 12.63 ± 2.110 0.002 WCC 8.225 ± 4.064 10.65 ± 15.36 0.015 Platelets 255.4 ± 103.5 257.5 ± 92.97 0.421 INR 1.07 ± 0.1523 1.349 ± 2.566 0.04 Prothrombin time 12.76 ± 6.622 12.45 ± 1.629 0.582 Renal and liver tests Na 137.1 ± 4.122 136.4 ± 5.687 0.03 K 3.963 ± 0.5484 4.191 ± 0.7182 0.005 Urea 5.632 ± 5.376 8.722 ± 9.491 < 0.0001 Creatinine 92.12 ± 65.74 139.6 ± 231.7 0.015 eGFR 94.1 ± 29.81 76.35 ± 34.28 < 0.0001 Bilirubin 15.62 ± 33.47 13.31 ± 9.124 0.77 ALT 76.01 ± 163.6 55.05 ± 40.9 0.545 AST 60.34 ± 156.6 48.98 ± 36.69 0.369 High ALT/AST (>63/37) (yes/no) 114/125 60/51 0.134 ALP 85.87 ± 51.19 90.28 ± 39.68 0.11 Albumin 31.58 ± 7.588 27.79 ± 7.43 < 0.0001 ALP: alkaline phosphatase, ALT: alanine aminotransferase, AST: aspartate aminotransferase, eGFR: estimated glomerular filtration rate, Hb: hemoglobin, INR: international normalized ratio, K: potassium ions, Na: sodium ions, WCC: white cell count
- Table 4.
- Illness severities and clinical outcomes of the diabetic and non-diabetic COVID-19 patients.
Severities/outcomes Non-diabetic COVID-19 patients (n=239) Diabetic COVID-19 patients (n=111) P-value Illness severity Mild to moderate (yes/no) 110/129 28/83 0.0001 Severe (yes/no) 85/154 39/72 0.469 Critical (yes/no) 44/194* 44/67 <0.0001 Clinical outcome Duration of illness (days) 5.714 ± 3.143 5.928 ± 3.15 0.549 Admission to intensive care unit (yes/no) 46/193 48/63 <0.0001 Death (yes/no) 24/215 40/71 <0.0001 ↵* one case was missing this information
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.