


Abstract
Objectives: To provide insights into the real-world usage of glucagon-like peptide-1 receptor agonists (GLP-1RAs) and sodium-glucose cotransporter 2 inhibitors (SGLT2i) among individuals with type 2 diabetes (T2D) from Bahrain, Kuwait, and Qatar who either had established atherosclerotic cardiovascular disease (eASCVD) or were at high risk of developing ASCVD.
Methods: This study of 1062 adults diagnosed with T2D from Bahrain, Kuwait, and Qatar is a sub-analysis within the Prevalence and Clinical Management of Atherosclerotic Cardiovascular Diseases in Patients with Type 2 Diabetes across Countries in the Middle East and Africa (PACT-MEA) study, a noninterventional, cross-sectional study. Participants were recruited from 13 primary or secondary care facilities between March and August 2022. Medical records of participants were reviewed to extract relevant data, including demographic characteristics, eASCVD status, ASCVD risk and glucose-lowering treatment. Appropriate descriptive and inferential statistical tests were performed.
Results: Among T2D participants with eASCVD, a significantly higher proportion (41.3%) received SGLT2i compared to GLP-1RA (10.5%, p<0.001). There were notable variations in GLP-1RA/SGLT2i utilization across countries (p<0.001): being lowest in Bahrain (2.3%/18.0%), 26.9%/58.2% in Kuwait and 10.5%/67.1% in Qatar. The use of both medications was significantly higher in individuals with body mass index (BMI) ≥30 kg/m2 (p<0.05).
Conclusion: Despite these cardioprotective agents being recommended by guidelines, the study findings suggest a suboptimal use of GLP-1RA and SGLT2i in a real-world setting.
Atherosclerotic cardiovascular disease (ASCVD) is the leading cause of morbidity and mortality in people with type 2 diabetes (T2D).1 Adults with T2D have around a 2-fold higher risk of morbidity and mortality from cardiovascular disease (CVD) than adults without diabetes.2 In recent decades, the prevalence of T2D and its associated cardiovascular complications has rapidly increased in the Middle East and North Africa (MENA) Region.3 This trajectory is expected to continue, resulting in increased healthcare costs, morbidity, and mortality.3 Within this region, the Gulf countries of Kuwait, Qatar, and Bahrain carry a disproportionately high burden of diabetes and CVD complications, which are the leading causes of death.4,5 However, the risk of adverse CVD-related outcomes can be mitigated by addressing risk factors such as atherosclerosis, hypertension, dyslipidemia, obesity, insufficient physical activity, inadequate glycemic control, and smoking.6
Glucagon-like peptide-1 receptor agonists (GLP-1RA) and sodium-glucose cotransporter 2 inhibitors (SGLT2is) are glucose-lowering agents that have shown efficacy in reducing the incidence of major adverse cardiovascular events (MACEs) and have been shown to reduce mortality compared to other glucose-lowering drugs.7-9 The GLP-1RAs and SGLT2 is improve glucose control and reduce triglyceride levels, whereas GLP-1RAs also promote weight loss and improve lipid control.10-12 Both medications have beneficial effects on cardiovascular risk.9
Despite these benefits, the recent CAPTURE study, a multinational, cross-sectional study of CVD prevalence in adults with T2D, found that GLP-1RA/SGLT2i use was low among patients with T2D and established CVD.13 This implies that cardiovascular risk management in patients with T2D is often suboptimal and inconsistent with current diabetes and cardiology guidelines. In patients with T2D, including those in Kuwait, Qatar, and Bahrain, many fall short of treatment targets for glycemic, blood pressure, or lipid control, significantly increasing their risk of ASCVD and CVD.14-16
International guidelines recommend the use of a GLP-1RA or SGLT2i for patients with T2D and ASCVD, high-risk indicators, kidney disease, or heart failure.1,6 However, there is a paucity of real-world evidence on the use of these medications in the MENA region, including Gulf countries such as Bahrain, Kuwait, and Qatar. The Prevalence and Clinical Management of Atherosclerotic Cardiovascular Diseases in Patients with Type 2 Diabetes across Countries in the Middle East and Africa (PACT-MEA) study was carried out across 7 countries in the region to address this knowledge gap. This study aimed to evaluate the proportion of patients with T2D with established ASCVD (eASCVD) or high ASCVD risk who received guideline-recommended treatment with a GLP-1RA or SGLT2i in these countries. Our study highlights data from 3 Gulf Region countries–Kuwait, Qatar, and Bahrain–to provide valuable insights into medication utilization, enabling healthcare professionals and policymakers to make informed decisions to enhance patient outcomes and alleviate the burden of ASCVD and T2D in the Gulf Region.
Methods
The PACT-MEA is a non-interventional, cross-sectional, observational study conducted at 55 centers in 7 countries.4 The overall study sample included 3726 individuals, and our analysis focused on data from 1062 participants from Bahrain (n=366, 9.8%), Kuwait (n=350, 9.4%), and Qatar (n=346, 9.3%). Participants across the 3 countries were recruited from 13 centers during scheduled visits. Local Institutional Review Boards reviewed and approved the study protocol and informed consent forms. Patients were required to sign the consent form before study-related activities took place. Consent was also subject to the patient having received verbal and written information informing them about the study in advance. This study was conducted in accordance with the Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Patients, the Guidelines for Good Pharmacoepidemiology Practices,17 and Strengthening the Reporting of Observational Studies in Epidemiology18 reporting guidelines.
In Kuwait, recruitment occurred from June to August 2022 at primary and secondary care facilities, including Farwaniya Hospital, Yarmouk Primary Health Care Center, Al-Omariya Clinic, Al-Jahra Hospital, Mishref West Clinic, and Mubarak Al-Kabeer Hospital. In Bahrain, participants were recruited between April and August 2022 at 4 secondary care facilities: Mohammed Bin Khalifa Bin Salman Khalifa Cardiac Center, Salmaniya Medical Complex, Bahrain Defence Force Hospital, and King Hamad University Hospital. In Qatar, 3 Hamad Medical Corporation secondary care facilities participated in recruiting participants from June to August 2022. National experts (who were part of the steering committee), and the Contract Research Organization created a roster of primary and secondary care facilities. The division of care settings was determined at the country level based on local treatment dynamics.
The inclusion criteria involved adult patients (age ≥18 years) diagnosed with T2D for a duration of ≥180 days who provided informed consent. Patients with type 1 diabetes or known congenital heart disease or malformations were excluded.
The study outcome was the proportion of participants with eASCVD or at high risk of ASCVD and receiving treatment with a GLP-1RA or SGLT2i. Additionally, we examined the proportion of participants meeting the reimbursement criteria based on local guidelines, where applicable. A chart review of the study population identified the prevalence of eASCVD (including coronary artery disease, cerebrovascular disease, and peripheral artery disease) and the proportion of patients with T2D classified as having high or very high ASCVD risk. The risk of ASCVD was evaluated and categorized according to the 2021 European Society of Cardiology guidelines on cardiovascular disease prevention in clinical practice.6
This study included a review of medical records and a survey of physicians. The study investigators conducted comprehensive medical chart reviews to collect data on demographics, anthropometrics, medical history of T2D, diabetes complications, ASCVD, cardiovascular risk factors, and pharmacotherapy. The physician asked the patient if the information was unavailable in the health records. Missing data points were noted for all study participants. Analyses were conducted using complete cases only, as the proportion of missing data was minimal for key study variables and unlikely to affect statistical power or introduce bias.
The survey involved physicians who were actively involved in the management of T2D within routine clinical practice. They were selected from both primary and secondary care settings. The types of specialties included general practitioners, family medicine physicians, endocrinologists, diabetologists, cardiologists, and internal medicine physicians. The Contract Research Organization’s deciphering system was used to internally program data from the physician survey.
Statistical analysis
Descriptive statistics were used to explore the distribution of participants’ characteristics and study outcomes. Categorical variables were expressed as frequencies and percentages, with 95% confidence intervals (CIs) as appropriate. Continuous variables were presented as means and corresponding standard deviations (SDs). The unweighted prevalence (in percentage) of eASCVD in T2D study participants was calculated for each country, and weighted prevalence was estimated for the overall T2D study population. One-way analysis of variance (ANOVA) tests were used to compare means across groups, while Chi-squared tests were used to compare proportions. Statistical significance was considered at p-value of < 0.05. Analyses were conducted using SPSS (version 23) and Stata (version 16.1).
Results
The study sample included 1062 adults with T2D (n=202 from primary care and n=860 from secondary care) from Bahrain, Qatar, and Kuwait. Study participants across the 3 countries had T2D for a mean duration of 13.4 years (SD=8.5) and a mean glycated hemoglobin (HbA1C) level of 7.9% (SD=1.9, 63 mmol/mol). The mean age of the overall study population was 57.9 years (SD=11.3), with males constituting 53.5% and females representing 46.5% of participants across the countries. More than 70.6% of the participants were below the age of 65, and 58.2% were aged between 45 and 64 years (n=618). Many patients had concomitant conditions and risk factors for ASCVD, including obesity (50.7%), dyslipidemia (81.6%), and hypertension (67.1%) as are presented in Table 1.
- Baseline characteristics of study participants.
The weighted prevalence of eASCVD in the T2D study participants in Bahrain, Qatar, and Kuwait was 22.2% (95% CI: 19.8–24.8), varying significantly by country (p<0.001). According to the 2021 European Society of Cardiology guidelines categories,6 the weighted distribution of ASCVD risk categories revealed that 64.7% of T2D participants across the 3 countries were classified as having a high risk and 35.3% as having a very high risk of ASCVD. Notable between-country differences in participants’ characteristics were observed for age (p=0.002), gender (p=0.024), HbA1C levels (p<0.001), and the prevalence of risk factors such as obesity (p=0.014), hypertension (p=0.011) and dyslipidemia (p<0.001). The 3 countries also differed significantly in the observed prevalence of eASCVD (p<0.001). There were, however, no observable differences in T2D duration (p=0.956) and current smoking status (p=0.306) (Table 1).
Furthermore, we investigated the use of GLP-1RA and SGLT2i medication across participants’ characteristics (Table 2). We found that GLP-1RA use was most common in Kuwait and least common in Bahrain across all 3 groups, whereas SGLT2i use was highest in Qatar and lowest in Bahrain for those with T2D and those with eASCVD and at a high risk of ASCVD. Of the 1042 study participants receiving antidiabetic medications, 16.4% received a GLP-1RA, and 39.9% received an SGLT2i. Medication trends varied substantially across countries (p<0.001), with Bahrain having the lowest proportion of patients receiving cardioprotective glucose-lowering drugs; 9.8% of participants received a GLP-1RA while 23.2% received an SGLT2i. In the other 2 Gulf Region countries, the use of GLP-1RAs was observed to be higher in Kuwait (25%) than in Qatar (14.6%), whereas in Qatar, a higher percentage of participants (56%) received SGLT2 is than in Kuwait (41.7%).
- Glucagon-like peptide-1 receptor agonists (GLP-1RA) and sodium-glucose cotransporter 2 inhibitors (SGLT2is) medication utilization across participants’ characteristics in the Gulf countries of Bahrain, Kuwait and Qatar.
Among the T2D participants with eASCVD (n=276), a significantly higher proportion (41.3%, 95% CI: 35.4–47.4) received an SGLT2i (n=114) compared to GLP-1RA (10.5%, 95% CI: 7.2–14.7) (p<0.001). There were notable variations across the 3 countries (p<0.001, Table 2). Bahrain had the lowest utilization of cardioprotective glucose-lowering drugs, with 2.3% receiving a GLP-1RA and 18% receiving an SGLT2i. The use of GLP-1RAs was higher in Kuwait (26.9%) than in Qatar (10.1%), while in Qatar, a higher percentage of participants (67.1%) received SGLT2is than in Kuwait (58.2%) (Table 2).
Among the participants classified as having a high risk of ASCVD (n=694), according to the 2021 European Society of Cardiology guidelines,6 19% (95% CI: 16.4 – 22.5) received a GLP-1RA, and 41.3% received an SGLT2i. By country, the use of GLP-1RA/SGLT2i was as follows: Bahrain, 14%/27%; Kuwait, 26%/41%; and Qatar, 17%/56%. The T2D medications, specifically GLP-1RAs and SGLT2is, were stratified into 5 age groups. No significant differences in GLP-1RAs and SGLT2i medication trends were observed across age groups (p>0.05). The use of GLP-1RAs and SGLT2is in patients with T2D was also stratified according to the participant’s body mass index (BMI) scores. Utilization of both medications was significantly higher in individuals with BMI ≥30 kg/m2 (p<0.05). Among participants with BMI <30 kg/m2 (n=451), 8.7% received a GLP-1RA and 36.3% received an SGLT2i. Among participants with BMI ≥30 kg/m2 (n=443), 24.3% received a GLP-1RA and 44.7% an SGLT2i. Data shown in Table 2.
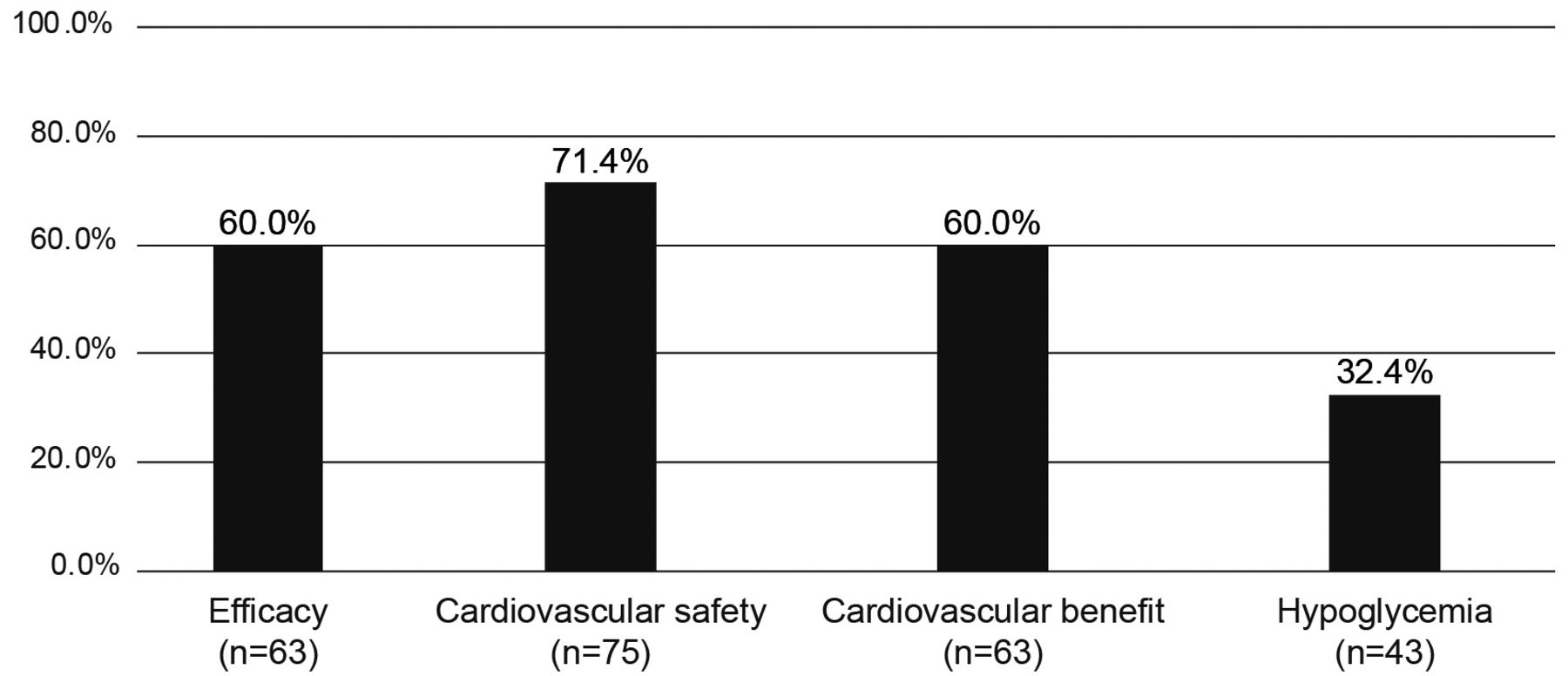
The physician survey included 34, 36, and 35 physicians from Bahrain, Kuwait, and Qatar, respectively. General practitioners comprised 51.7% of the sample, with the remainder comprising endocrinologists, diabetologists, internal medicine physicians, cardiologists, and family practice physicians. The mean number of years in practice for the surveyed physicians was 15.2 (SD=9.1) in Bahrain, 17.9 (SD=8.1) in Kuwait, and 14.3 (SD=8.0) in Qatar. When surveyed regarding the factors that predominantly guide their choice of antihyperglycemic treatment, physicians indicated that the primary considerations were efficacy, cardiovascular safety, cardiovascular benefits, and the risk of hypoglycemia (Figure 1).

- Considerations for antihyperglycemic treatments according to the study physicians surveyed in the Gulf Region (n=105)
In the context of managing T2D, the key clinical factors to consider were HbA1C levels, chronic kidney disease, high risk of ASCVD, complications of diabetes, safety profiles of medications, and heart failure. The most important considerations concerning patients were treatment adherence, safety concerns, and impact on health-related quality of life. Regarding the practice factors that influence T2D management, the most significant were the availability of treatment and access to healthcare personnel. Other factors identified as influential in the management of T2D included continuous medical education, medical knowledge and specialization, adherence to international guidelines, previous experience with medications, and patient-empowering behaviors.
Discussion
The unique characteristics of cardioprotective glucose-lowering agents and the mounting evidence supporting their effectiveness in reducing cardiovascular morbidity and MACEs and their renal safety have resulted in their recommendation as preferred treatment options for patients with T2D with a high risk of or established cardiovascular disease, chronic kidney disease, or both.1,6,20 Taking into consideration the benefits and the recent guideline recommendations from the American Diabetes Association1 and European Society of Cardiology6 advocating their use, our study evaluated the use of GLP-1RAs or SGLT2is among individuals with T2D, eASCVD, or high ASCVD risk in the Gulf Region. Although their use has increased, it remains suboptimal, as this study shows, with less than half of individuals with T2D at high risk of ASCVD who are most likely to benefit from their cardiovascular and renal advantages receiving either medication.21,22
Prior to the international guideline recommendations, a cross-sectional study was conducted on a large set of United States claims data to evaluate the baseline use of antidiabetic medications and healthcare specialty utilization.23 That study identified that the use of GLP-1 RAs and SGLT2is was low overall (<12%) and even lower in the ASCVD group (<9%).23 The use of these cardioprotective drugs in our study appeared to be comparable to the more recent global PACT-MEA study results, which reported that 13% of the 3726 T2D participants received GLP-1RAs and 37% received SGLT2is.4 We found that among the overall T2D population receiving antidiabetic treatments in Bahrain, Kuwait, and Qatar, 16.4% received a GLP-1RA, and 39.9% received an SGLT2i.
Consistent with our findings, the CAPTURE study, involving 9823 participants from 13 countries, reported that SGLT2is were also more frequently used than GLP-1RAs in the overall study sample (15% versus 8.6%).13 However, the percentages of patients utilizing either of these 2 therapeutic classes were lower in the CAPTURE study than in our study. The higher utilization of both medications in our study may reflect the influence of the updated guidelines on prescription practices.
Our study further found that among T2D participants with eASCVD, a significantly higher proportion (41.3%) received SGLT2i compared to GLP-1RA (10.5%), with notable variations across the 3 countries. These differences in utilization patterns between countries in our study may be attributed to variations in the recruitment of study sites, the type of clinical setting, or practice factors such as availability and access to treatment. While our study did not identify a statistically significant difference between age strata and medication use, prescription rates in older populations were notably lower. This may be related to therapeutic inertia, concerns on potential adverse effects, and limited safety data owing to the under-representation of older adults in clinical trials.24,25 Developing precise and current recommendations for the use of these drugs in target populations is thus an important approach to better support clinical decision-making.26 In addition, further research into the use of cardioprotective glucose-lowering agents in high-risk subpopulations in the Gulf Region is needed.27
The GLP-1RAs and SGLT2is are associated with several benefits, including weight loss and improved glycemia, hypertension, and dyslipidemia.9,10,28 Yet, less than half of the study participants with T2D with BMI >30 kg/m2 were treated with either medication. The poor control of T2D and modifiable risk factors for CVD, such as obesity, is a persistent concern in the Gulf Region.14-16 In particular, GLP-1RAs have been recommended and are being used as a treatment for obesity.29 Our study showed that GLP-1RA use was significantly higher in participants with a BMI ≥30 kg/m2 than in those with a BMI <30 kg/m2. However, there is currently little to no evidence on the use of GLP-1RAs and overweight/obesity in the Gulf Region countries, which suggests an opportunity for further investigation. In our study, on average, glycemic levels were higher than the HbA1C guideline recommendation for reducing CVD risk.6 Additionally, there was a high prevalence of other cardiovascular risk factors, including hypertension, dyslipidemia and smoking among the study participants. These findings underscore the need for effective antihyperglycemic therapies, adherence to treatment guidelines, and recommendations for strategies to manage these risk factors.6
The physician survey conducted as part of this study emphasizes the importance of considering the efficacy, risk of hypoglycemia, and cardiovascular benefits when selecting antihyperglycemic treatments for patients with T2D. Other studies conducted have also stressed the importance of clinicians basing their clinical decisions on the positive effects of specific glucose-lowering agents on cardiovascular outcomes.30,31 GLP-1RAs and SGLT2is are generally well tolerated by individuals with minimal risk of hypoglycemia.32
Overall, this study provides valuable insights into the real-world utilization of GLP-1RAs and SGLT2is in the Gulf Region, highlighting the need for improved management of ASCVD and T2D in this population. These findings can guide healthcare professionals in making informed decisions to enhance patient outcomes and alleviate the burden of ASCVD and T2D in the Gulf Region.
Study strengths
The strength of this study lies in its valuable contribution to the limited pool of real-world evidence in the Gulf Region, and growing body of evidence on the recommended treatment with GLP-1RAs or SGLT2is and associated factors among individuals with T2D, eASCVD, or high ASCVD risk in the region. The findings from this study suggest targeted screening and treatment and illuminate the current utilization of these agents, underscoring the imperative need for action. By addressing the existing gap in the literature, this study paves the way for informed decision-making and advancements in this domain.
Study limitations
Our study has several limitations that warrant consideration. First, while medical records have several advantages when used as data sources for research, they may be prone to issues such as inconsistencies in data capture across patients, healthcare facilities and geographical settings. Secondly, the variation in the organization of healthcare, both between and within countries, makes direct comparisons between countries less meaningful. Another limitation is the sampling of participants within healthcare settings, which may be prone to selection bias. As such, the findings may not be generalizable to populations that do not have access to healthcare services or have limited access to them.
Conclusions
Despite the high prevalence of T2D in the 3 Gulf Region countries and guidelines recommending the use of cardioprotective agents in patients with T2D and eASCVD or those at high risk of ASCVD, the study findings suggest suboptimal use of these agents. Findings underscore the need for effective antihyperglycemic therapies, adherence to treatment guidelines, and recommendations for strategies to optimize use, particularly in high-risk patients who are most likely to benefit from the cardiovascular and renal benefits of these therapeutic agents.
Acknowledgment
We would like to thank Last Mile P/S for providing editorial writing support and Editage (https://www.editage.com) for editing the English language.
Footnotes
Disclosure. This study was funded by Novo Nordisk, Salmiya, Kuwait. Dr. Naji Alamuddin is a member of Novo Nordisk’s Speaker Bureau and a consultant for Novo Nordisk. Prof. Usama Al Alami, Dr. Guruprasad Subbarao, and Dr Shashikanth Chetty are Novo Nordisk employees.
- Received November 19, 2024.
- Accepted January 14, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.