


Abstract
Objectives: To compare pathological samples obtained from cases that underwent surgery for ureteropelvic junction (UPJ) obstruction with samples obtained during autopsies of subjects.
Methods: Retrospectively, 42 patients who had undergone surgery due to UPJ obstruction (group 1) were included in the study. Histopathological and immunohistochemical features for sonic hedgehog (SHH), TBX18, and TSHZ3 of UPJ were evaluated and findings were compared with 20 autopsy cases (group 2).
Results: In group 1, the scores were statistically significantly higher in terms of cytoplasmic SHH, nuclear TBX18, cytoplasmic and nuclear TSHZ3 staining. Statistically, no correlation was found between age and the staining scores belonging to these 3 antibodies in group 1 and group 2. Intense inflammation was found to be related with nuclear staining for TBX18.
Conclusion: Gene product expressions of SHH, TBX18 and TSHZ3 are statistically higher in patients with UPJ obstruction, when compared with control group. The explanation may be the reactivation of the processes, which had shown their effects in the embryological period, due to the chronic inflammation and long-term micro-trauma created by the disease.
Ureteropelvic junction (UPJ) obstruction is the most frequent cause of urinary obstructions in children.1 So far, the studies have failed to show how UPJ obstructions develop, with conclusive evidence. Histopathologically, it has been found that there are findings, such as inadequately or irregularly structured smooth muscle fibers, abnormal collagen deposition, increased muscle cell apoptosis, abnormal innervation, and disordered distribution of Cajal cells in UPJ samples obtained during surgery.2-5 Studies that would explain the genetic mechanisms of the UPJ obstructions have been carried out experimentally; the studies performed on humans are very limited in English medical literature. In experimental animal studies, the gene expressions of BMP4,6 sonic hedgehog (SHH),7 TBX18,8 and TSZH39 have been shown to play a primary role in the development of UPJ, particularly in smooth muscle formation. However, studies related to the effects of the productions of these genes on UPJ obstruction in humans are very limited. The aim of this study is to investigate the roles of the products of these genes in the pathogenesis of UPJ obstructions by comparing pathological samples obtained from cases who underwent surgery for UPJ obstruction with samples obtained during legal autopsies of subjects who had died due to legal causes and had no known disease provided by the District Forensic Medicine Institute.
Methods
Search of related articles
Searching of the prior articles related to the study idea has been made by using PubMed.
Patients and control group selection
Retrospectively, a total of 42 patients who had undergone surgery for the diagnosis of UPJ obstruction due to the symptoms and signs like more than 10% decrease in split renal function, pain, and stone formation in our department between January 2009 and December 2014 were included in the study. Grade III or IV hydronephrosis was ultrasonographically detected in all of the patients before the operation. Only patients who had intrinsic obstruction were selected as group 1, excluding cases that had extrinsic obstructions or associated renal disorders. Twenty seven of the cases were boys and 15 were girls in ages ranging between one and 15 (mean 6.72 ± 4.13) years. Twenty autopsy cases of 14 boys and 6 girls, prospectively collected in the Forensic Medicine Institute, Izmir District, Turkey within similar age range (2-15; mean 6.09 ± 4.74), had no known disease and who did not undergo autolysis were selected as control group (group 2); in this group, the cause of death was traffic accident in 8, drowning in 4, and falling off in 3 cases, while no identifiable cause of death were detected in 5 cases. Autopsy cases with renal or another medical disorders identified during autopsy, were excluded from the study. All procedures were in accordance with the Helsinki Declaration, and approvals of Local Ethics Committee and District Forensic Medicine Institute were obtained before the study.
Sampling and microscopic evaluation
The ureteropelvic junctions containing the stenotic area (for group 1) and a small renal parenchymal area (for group 2) were sampled for histopathological examination. After fixing in formalin, embedding in paraffin and obtaining 5µ sections, the slides were stained with hematoxylin and eosin and evaluated for chronic inflammatory cellular infiltration, smooth muscle atrophy or hypertrophy, and subepithelial fibrosis, as well as to rule out presence of any other pathology. Inflammatory cellular infiltration in lamina propria, muscular and serosal layers togetherly and subepithelial fibrosis were scored semi-quantitatively as: absent or mild (0); moderate (1); and intense (2); whereas smooth muscle atrophy and hypertrophy were numbered as atrophy (1) and hypertrophy (2) to facilitate statistical analysis. All slides were evaluated by 2 pathologists in a double-blinded fashion.
Immunohistochemical assessment
After routine tissue processing, selected slides were stained with BMP4, SHH, TBX18, and TSHZ3 antibodies (Table 1) in fully automatic immuno-staining device (Ventana®, Benchmark XT, Ventana Medical Systems, Tucson, Arizona) with standard streptavidin-biotin immunoperoxidase method with 3% hydrogen peroxide for inhibiting endogenous peroxidase activity, Ultra V Block to inhibite non-spesific staining, diaminobenzidine (DAB, DAKO, K4011) as chromogen, Mayer’s hematoxylin for counter-staining, and Entellan® (Merck and Co., Berlin) for sealing.
Staining scores for sonic hedgehog (SHH), TBX18, and TSHZ3 in group 1 and 2.
Staining properties were assessed under standard light microscope by the same pathologists in a semi-quantitatively manner in mesenchymal cells (namely, smooth muscle cells and fibroblasts). Since only cytoplasmic staining for SHH and both cytoplasmic and nuclear staining was observed for TBX18 and TSHZ3 in control tissues, staining in respective sites was assessed in group 1 and 2 cases. For the latter 2, antibodies, cytoplasmic, and nuclear staining were separately evaluated. As for BMP4, this antibody was not found to be reliable to assess and excluded from the study, since diffuse and non-specific staining in extracellular matrix areas and in cytoplasm in control tissues, as well as in both of the study groups.
Either nuclear or cytoplasmic staining of the 3 antibodies was scored as follows: no staining (0); positive staining cells <5% (1); 5%≤ positive staining cells <50% (2), and positive staining cells ≥50% (3). For cytoplasmic staining, intensity of staining was also considered as no staining (0), weak staining (1), moderate staining (2), and intense staining (3). For antibodies staining both nuclear and cytoplasmic (namely, TBX18, and TSHZ3), the average of 2 scores were taken into consideration. Final staining scores were obtained by getting the average score of the scores of the 2 pathologists.
Statistical evaluation
Spearman’s Rho test, Kruskal-Wallis variance analysis test, and Mann-Whitney U test were performed using the Statistical Package for the Social Sciences version 15 (SPSS Inc., Chicago, ILL, USA). A value of p<0.05 was considered statistically significant.
Results
Histopathological findings
In histopathological examination, chronic inflammation was observed in all cases of group 1, which was mild in 2, moderate in 27, and intense in 13 cases with an average inflammation score of 1.21 ± 0.56. No signs of inflammation was found in cases of group 2. In group 1, fibrosis was absent in 2, moderate in 17, and intense in 23 cases with an average fibrosis score of 1.50 ± 0.59, whilst no fibrosis was identified in the subjects of group 2. In all cases of group 1, atrophy (n=29) or hypertrophy (n=13) was observed in ureteral muscular layer, contrary to group 2 carrying none of these findings. In terms of these 3 parameters (namely, inflammation, fibrosis, and athrophy/hiperthrophy), there were statistically significant differences between the 2 groups (p=0.01, p=0.01, p=0.01, Mann Whitney U test).
Immunohistochemical findings
Detailed staining scores of group 1 and group 2 were given in Table 1. Immunohistochemical staining could be evaluated in 39 cases for SHH, 38 cases for TBX18, 42 cases for TSHZ3 of 42 cases (group 1), and all autopsy cases (group 2; n=20). As shown in Table 2, there were statistically significant differences between final average staining scores of the 2 groups, in terms of cytoplasmic SHH (p=0.01), nuclear TBX18 (p=0.01) and cytoplasmic TSHZ3 (p=0.01) staining, as well as a borderline significance in nuclear TSHZ3 (p=0.05) staining. Only cytoplasmic staining of TBX18 was found to be statistically significance.
Final avarage staining scores for sonic hedgehog (SHH), TBX18, and TSHZ3 staining in group 1 and 2, and the statistical differences between the 2 groups (bold numbers indicate statistically significant differences).
Reclassifying cases of group 1 according to severity of inflammatory cell infiltrate as group 1a (cases with moderate inflammatory reaction) and group 1b (cases with intense inflammatory reaction), and comparing the final average staining scores of the 3 antibodies, only statistically significant difference was obtained for TBX18 nuclear staining between the 2 subgroups (p=0.01, Kruskal-Wallis variance analysis test), as shown in Table 3. This datum indicates that nuclei of the stromal cells in cases with intense inflammatory reaction are more likely to be stained with TBX18. Two cases with mild inflammatory reaction were excluded because of inadequacy for statistical tests.
Final average staining scores for sonic hedgehog (SHH), TBX18, and TSHZ3 staining in group 1α (atrophy) and 1β (hypertrophy), and the statistical differences between the 2 groups (bold number indicate statistically significant differences).
The patients in group 1 were subsequently divided into 2 subgroups according to the presence of atrophy (group α) and hypertrophy (group β). Analysis of these subgroups according to the final average staining scores of the 3 antibodies revealed no statistically significant differences except in SHH cytoplasmic staining, indicating that stromal cells in hypertrophic cases are more prone to SHH staining (p=0.03, Mann Whitney U test, Table 4).
Final average staining scores for sonic hedgehog SHH, TBX18, and TSHZ3 staining in group 1a (moderate inflammatory reaction) and 1b (intense inflammatory reaction), and the statistical differences between the 2 groups (bold number indicate statistically significant difference)*.
Comparison of the subgroups according to the degree of fibrosis revealed no relationship between subgroups showing no or mild (n=2), moderate (n=17) and intense (n=23) fibrosis, in terms of expression of SHH, TBX18 (cytoplasmic-nuclear), and TSHZ3 (cytoplasmic-nuclear) gene products (p=0.08, p=0.28, p=0.25, p=0.06, 0.20, Kruskal-Wallis variance analysis test). Also, investigations for possible correlations between final average cytoplasmic and nuclear staining of the antibodies and subjects’ age have given no statistically significant results as shown in Table 5.
Correlation between final average cytoplasmic and nuclear staining scores for antibodies and subjects’ age (Spearman’s Rho test).

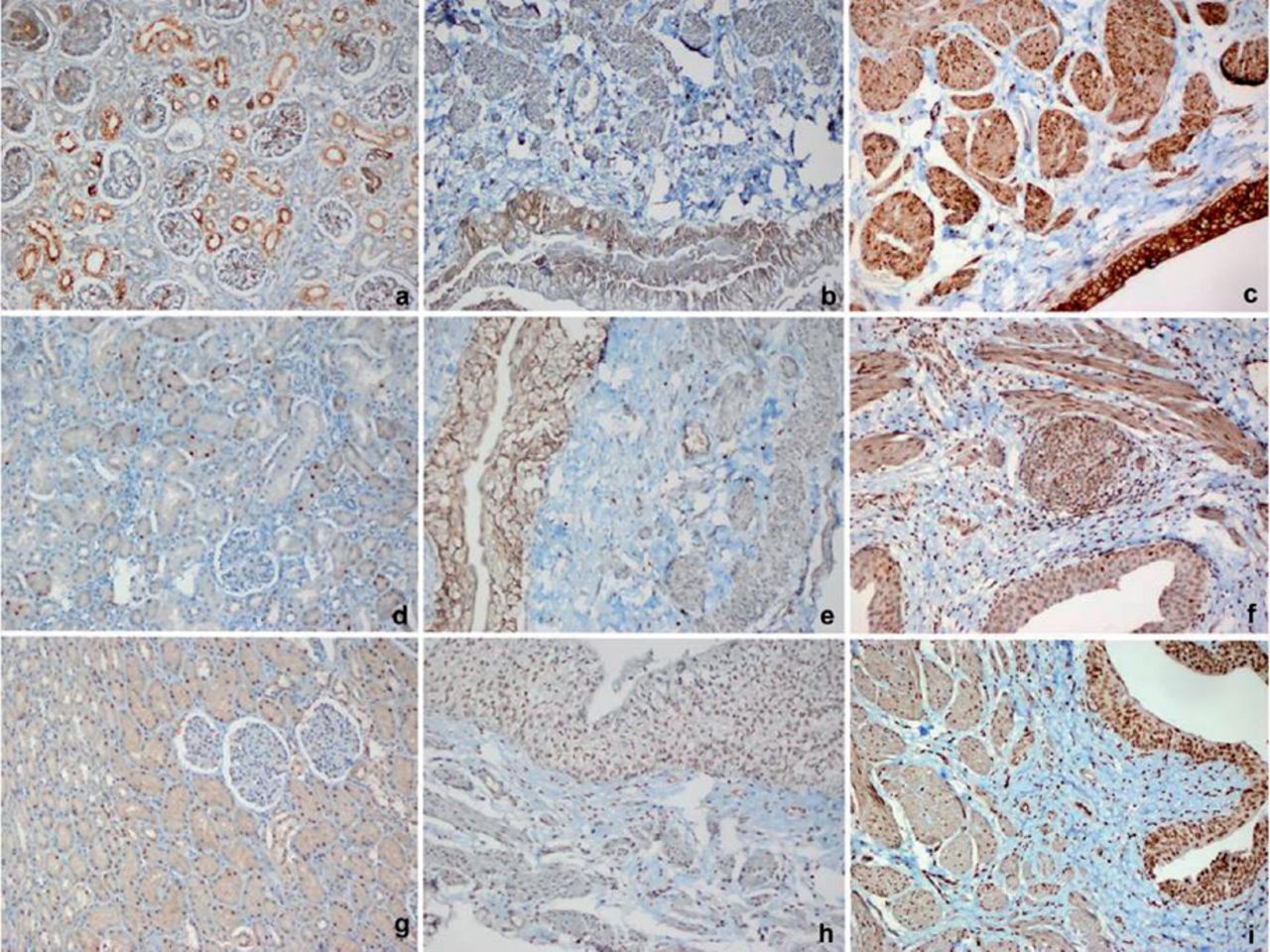
Examples of immunohistochemical staining: A) tubular epithelial cells manifesting cytoplasmic staining in fetal renal parenchyma used as positive control with sonic hedgehog (SHH) (DAB, x200), B) urothelial cells and smooth muscle cells manifesting cytoplasmic staining with SHH in a group 2 case (DAB, x200), C) urothelial cells and smooth muscle cells manifesting cytoplasmic staining with SHH in a group 1 case (DAB, x200), D) tubular epithelial cells manifesting nuclear and patchy mild cytoplasmic staining in renal parenchyma used as positive control with TBX18 (DAB, x200), E) urothelial cells and smooth muscle cells manifesting nuclear and cytoplasmic staining with TBX18 in a group 2 case (DAB, x200), F) urothelial cells and smooth muscle cells manifesting nuclear and cytoplasmic staining with TBX18 in a group 1 case (DAB, x200), G) tubular epithelial cells manifesting nuclear and cytoplasmic staining in fetal renal parenchyma used as positive control with TSHZ3 (DAB, x200), H) urothelial cells and smooth muscle cells manifesting nuclear and mild cytoplasmic staining with TSHZ3 in a group 2 case (DAB, x200), and I) uothelial cells and smooth muscle cells manifesting nuclear and cytoplasmic staining with TSHZ3 in a group 1 case (DAB, x200)
Discussion
In the intrinsic type of UPJ obstruction, the formation of stenosis has been tried to be explained by the occurrence of recanalization of this region to take place as the last one.10 Recently conducted studies have shown that errors in smooth muscle arrangement or organization lead to the deterioration of peristalsis in ureteropelvic junction.3
Our study focused on the products of 3 genes, SHH, TBX18, and TSHZ3, which are known to be responsible for formation of ureteral smooth muscles during the embryological development. The other studies have paid attention to BMP4 additionally. However, we found it to be unreliable due to non-specific background staining, so it was excluded from the study.
Ureter is known to consist of 2 components, epithelial and mesenchymal. Sonic hedgehog is expressed from the epithelium of ureteral bud stalk, which has a proliferative effect on ureteral mesenchyme induces production of BMP4 from the periureteral mesenchyme.7 As the result of SHH inactivation, maturation of the ureteral smooth muscle is delayed and a loss of stromal cells located between the smooth muscle and epithelium occurs. The studies related to SHH are generally experimental and focused on solely embryonic ureters.8 To the best of our knowledge, only Zhou et al10 showed the presence of SHH expression following renal trauma in his non-embryonic experimental study.
In our study, in patients with UPJ obstruction (group 1), a remarkable finding was the increased final average cytoplasmic staining score for SHH when compared with group 2, and this difference was found to be statistically significant (Table 2). Additionally, a statistically significant increase in cytoplasmic immunostaining of SHH in patients with smooth muscle hypertrophy was also stated (Table 4). These 2 findings, as if somewhat contrary to the experimental studies claiming that the reduction of SHH expression leads to delayed smooth muscle maturation, actually may lead to a different conclusion. This is also supported by the finding that, 40 out of 42 patients in group 1 had shown moderate or intense inflammatory reaction with no significant differences between these subgroups (Table 3), while none of the subjects in group 2 had inflammation.
The TBX18 is expressed from the metanephric renal and ureteral mesenchyme.8 The TBX18 was found to be the primary cause of hydroureter due to the reduction or complete disappearance of smooth muscle development in ureters of mutant mice.8 No study for TBX18 involving immunohistochemistry or which was performed in humans at the postnatal period was found in the literature. Since both cytoplasmic and nuclear staining were observed in controls of immunostains performed in fetal kidneys, both were investigated in our study. While no significant difference was found between group 1 and group 2 with TBX18 in terms of cytoplasmic staining, interestingly and akin to SHH, cases with UPJ obstruction (group 1) had statistically significantly higher average nuclear staining scores than in group 2, leading a similar conclusion to SHH.
Regarding the subgroups of group 1 according to the degree of inflammatory reaction, higher scores were obtained in intense inflammatory reaction group in terms of TBX18 nuclear staining, and this was statistically significant. Xu et al11 reported that vascular development during the embryological period was dependent on TBX18 in mammalian kidney. This mechanism, enabling organ development in the embryological period, may be reactivated in postnatal period in cases with UPJ obstruction for neovascularization related to chronic inflammation caused by micro-trauma and infections accompanying hydronephrosis and hydroureter. In our opinion, increased TBX18 nuclear staining being associated with increased degree of inflammation supports this suggestion.
Similar to SHH, TSHZ3 plays its role in the development of proximal ureteral smooth muscle layer. Caubit et al,12 in their study, reported that TSHZ3 was expressed from mesenchyme surrounding the urothelium, enabled smooth muscle development and its deficiency caused hydronephrosis. However, in another study conducted on human fetuses, it was shown to be expressed in human ureters but was not suggested as a major cause of UPJ obstruction.9 In our study, there were statistically significant differences between group 1 and group 2 and higher staining scores, especially cytoplasmic, was noteworthy in cases with UPJ obstruction raising the question, whether TSHZ3 gene may be reactivated postnatally due to the same reasons with the other 2. No significant differences were found in the statistical analysis performed on the cases subclassified according to the degree of inflammation, fibrosis, and presence of atrophy or hypertrophy in group 1. We agree that these genes are reactivated in the postnatal period and their products are increased immunohistochemically due to the mentioned reasons, then another question that comes to mind is if there is a relationship with age. In the statistical analysis, no correlations were found between age and the scores belonging to these 3 gene product expressions in both group 1 and group 2 (Table 5). In other words, the gene product expression scores do not change with age.
In conclusion, this study shows that gene product expressions of SHH, TBX18, and TSHZ3, which are probably playing roles in the embryological development of the ureteropelvic junction and inadequacy of which have been suggested to cause disorders during the embryological processes, are statistically higher in patients who underwent surgery for UPJ obstruction, when compared with normal subjects. This study is performed immunohistochemically on postnatal human subjects and we consider that the explanation may be the reactivation of the processes, which had shown their effects in the embryological period and then had stopped, probably due to the chronic inflammation and long-term micro-trauma caused by disturbances of urine flow in UPJ obstruction, an argument hitherto, mentioned a few times in the literature.13,14 Naturally, to prove this hypothesis in such a mysterious area with limited literature information, further investigations are required. In addition, since this is an immunohistochemical study, it is needed to show, whether protein expression reflects the molecular changes of these genes. Future studies regarding this issue may solve this problem and eventually may lead some therapeutic approaches related to these genes.
Student Corner
We invite students from a variety of medical disciplines to submit original contributions based on their supervised research.
The Student Corner of Saudi Med J aims to help students explore research opportunities and network with other peers and mentors in the same field.
Submission Guidelines
Submitted Abstracts should include the following:
Title should be descriptive
Author’s names and affiliation(specify college level/year, academic degree of Senior Author)
Abstract must be structured and not more than 300 words
The following are the typical headings:
Objectives (background, why the study was done, specific aims)
Methods (setting, date of study, design, subjects, intervention and analysis)
Results (findings, data and statistical tests) and
Conclusion (general interpretation of results)
General Information on Abstract Submission
Submitted Abstracts should be co-authored by a Senior Supervisor
Abstracts will be reviewed by Student’s Corner Section Editor
There is no fee to submit an Abstract
Ethical Approval should be provided non-indexed paper
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company. The study is granted by the Scientific Research Project Coordination Unit of Celal Bayar University, Manisa, Turkey (Grant # 2014/012).
- Received February 10, 2016.
- Accepted May 16, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.