


Abstract
Chondroblastoma is a rare benign cartilaginous tumor that accounts for approximately 1% of bone tumors, but it can be associated with lung metastasis in extremely rare cases, leading to a poor prognosis and death. Herein, we report the case of a 19-year-old male patient who presented with an aggressive chondroblastoma of the proximal humerus and bilateral lung metastasis. The patient was treated with wide local resection, partial metastasectomy, and denosumab. Denosumab treatment was effective in controlling metastatic progression and preventing local recurrence.
Chondroblastoma, as per World Health Organization’s (WHO) classification, is a rare benign cartilaginous tumor, accounting for approximately 1% of all bone tumors.1 It predominantly affects male gender than female gender and is most common in children or young adults. It is usually observed in the epiphysis or apophysis of long bones, most commonly located in the proximal tibia, femur, and humerus but may also involve the flat bones, and bones of the hands and feet.1,2 Although chondroblastoma is considered a benign tumor, it may metastasize, leading to varying outcomes, ranging from early to latent fatalities.2,3 Chondroblastoma metastasis usually occurs after diagnosis, particularly after recurrence, but can also be concomitant with the initial presentation.3,4 Lung metastasis is frequently reported, although other forms of metastasis, including soft tissue, bone, and visceral involvement, have been documented.1,5 Various treatment strategies have been explored to treat chondroblastoma-derived lung metastasis, including surgical resection, several chemotherapy regimens, radiotherapy, immunotherapy, and symptomatic palliative treatment.3,5 Histologically, chondroblastoma is characterized by polygonal chondroblastic cells and an eosinophilic chondroid matrix with occasional focal calcification and multinucleated osteoclast-like giant cells.1 Some studies have shown increased activity of receptor activator of nuclear factor kappa-β ligand (RANKL) in tumors containing giant cells (GC).6,7 Denosumab is a human monoclonal antibody that binds and inhibits RANKL, thereby reducing RANKL activity in GC tumors (GCTs). Recently, the clinical use of denosumab has been recommended for preventing recurrence, facilitating resection, and controlling lung metastasis.
In this report, we presented a case of a young male patient who was diagnosed with chondroblastoma of the left humerus. Following the initial Whoops surgery, rapid disease progression was noted, and the development of bilateral lung metastases was observed during follow up. The patient was treated with denosumab. In the second part of this report, we provided a literature review on the chondroblastoma metastasis pattern, treatment options, and outcomes associated with these treatments.
Case Report
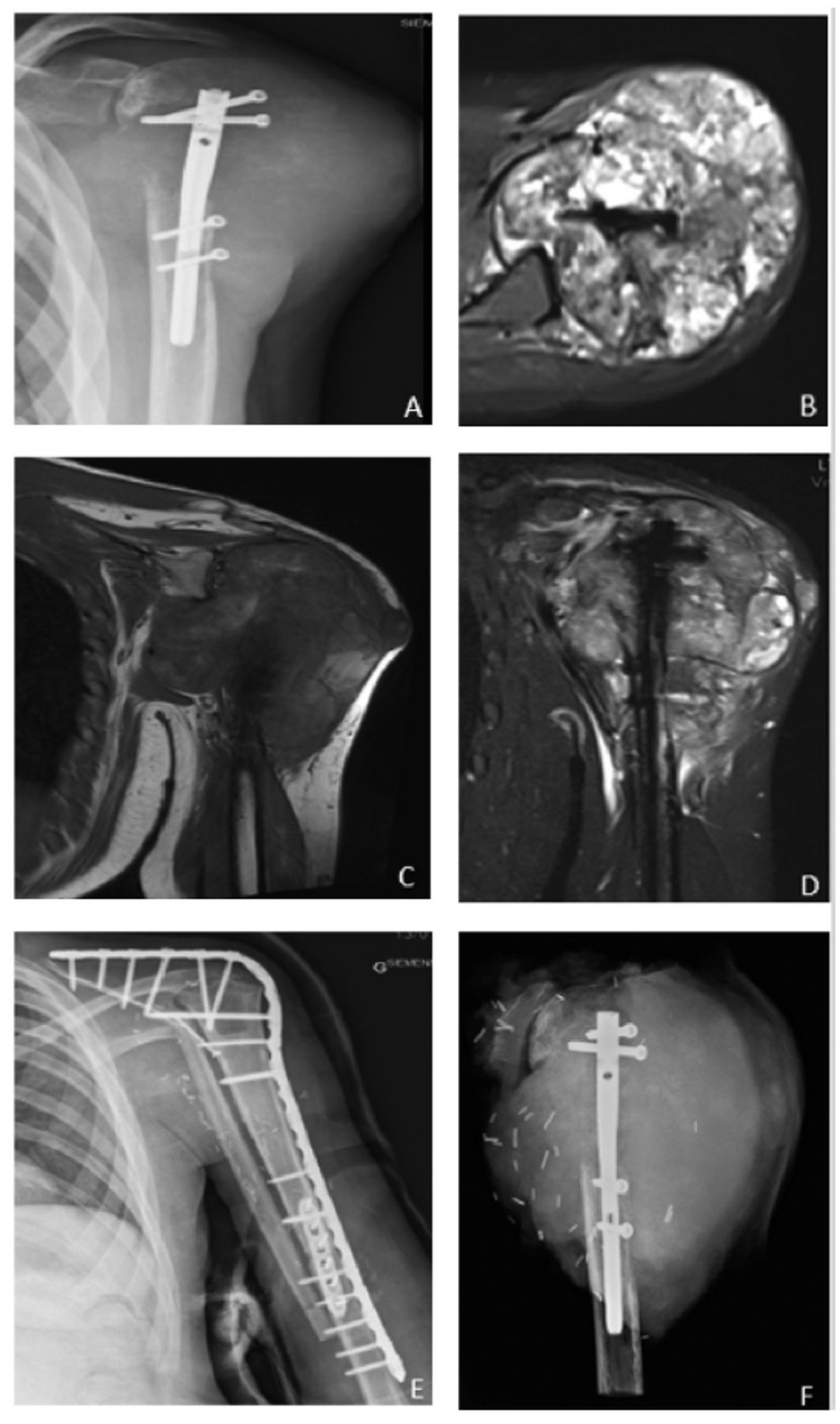
In January 2020, a 19-year-old right-handed patient presented with a pathological fracture of the proximal left humerus, following a football-related injury. The fracture was managed with intramedullary nail fixation in another center (Figure 1A). However, 7 weeks post-surgery, the patient reported limited shoulder flexion and abduction, accompanied by deltoid muscle atrophy.

- An anterior-posterior radiograph of the patient’s left humerus after intramedullary nail fixation. A) An ill-defifined lytic with cortical destruction and soft tissue extensions with no calcification is seen. B) Axial magnetic resonance imaging with T2-weighted fat-suppression reveals heterogenous signal intensity with an articular extension. C) A coronal T2-weighted fat-suppression image reveals a distal extension of the lesion. D) A coronal T1-weighted image reveals an isosignal intensity similar to that of muscles. E) A post-operative anterior-posterior radiograph of the patient’s left shoulder after resection and arthrodesis. F) A radiograph of the resection specimens.
Clinical information
In late February 2021, the patient experienced an increase in pain and was presented with bone osteolysis on X-ray. Consequently, the patient’s file was forwarded to our reference center. Urgent imaging was requested, and the results were received in April 2021.
Diagnostic assessment
Computerized tomography (CT) revealed extensive osteolysis and soft tissue extension at the proximal part of the humerus. Subsequent magnetic resonance imaging (MRI) revealed a complete cortical rupture of the proximal humerus, accompanied by an extensive heterogenous soft tissue extension (15×12×12 cm) and an intra-articular involvement (Figure 1).
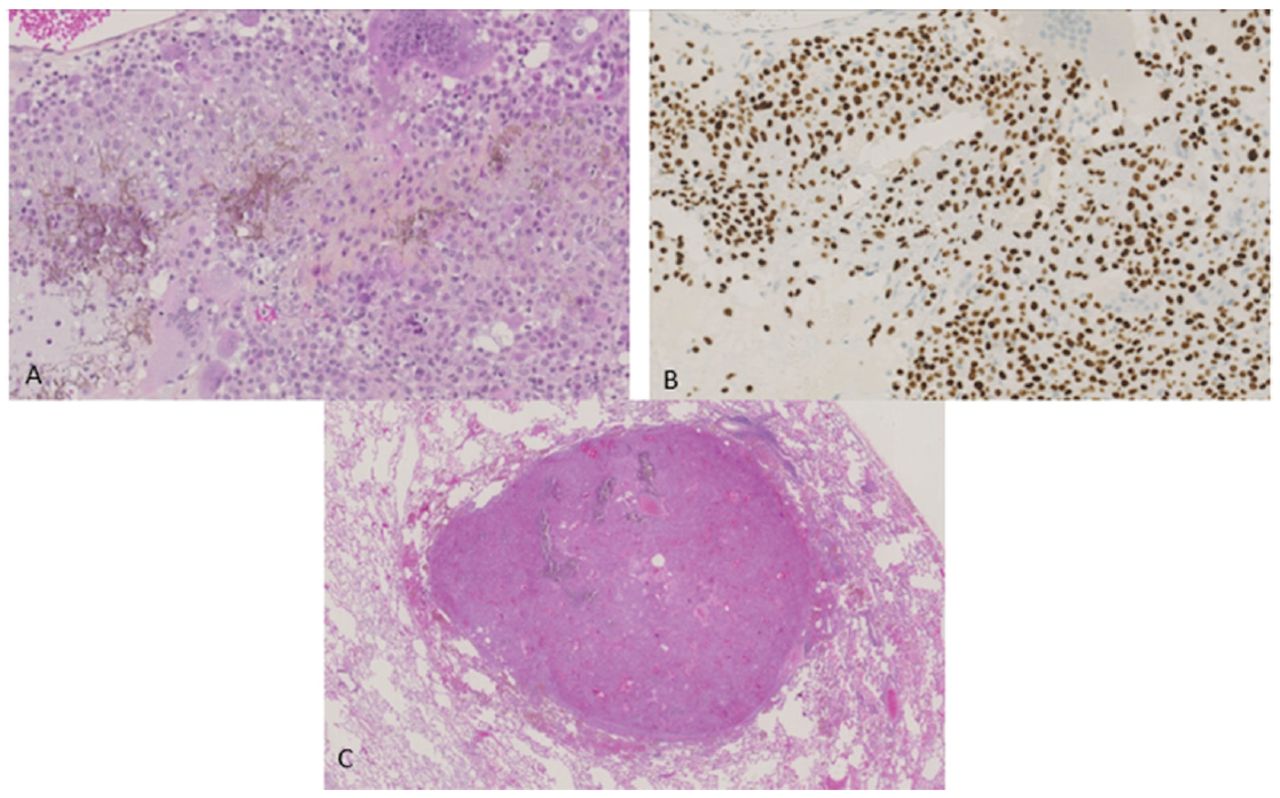
An urgent percutaneous biopsy was carried out in April 2021, and histopathological analysis revealed a tumor composed of chondroblastic cells with chicken-wire calcifications (Figure 2A). The tumor exhibited a high mitotic index (4 mitotic figures per high power field) and ischemic necrosis. Immunohistochemistry revealed positive staining of tumor cells with H3-3B, confirming the diagnosis of chondroblastoma (Figure 2B). Further evaluation using bone scan indicated intense fixation in the proximal left humerus, with no other discernible lesions.

- Microscopic features of the humeral tumor biopsy and lung metastasis resection. A) A tumor composed of chondroblastic cells with chicken-wire calcification (hematoxylin-eosin and saffron). B) Immunohistochemistry indicates H3-3B diffuse staining of chondroblasts. C) Chondroblastoma metastasis involving the lung parenchyma (hematoxylin-eosin and saffron).
A thoraco-abdominopelvic CT scan revealed the presence of 2 pulmonary nodules, measuring 5 mm each, in the right lower lobe. These nodules were accompanied by subpleural micronodules in the posterior basal segment of the left lower lobe.
Therapeutic intervention
In June 2021, the patient underwent video-assisted thoracoscopic surgical wedge resection of the right inferior lobe to address the pulmonary nodules. After 10 days, an extra-articular resection of the proximal humerus was carried out. Reconstruction of the humerus involved a scapula-humeral arthrodesis using a proximal tibia allograft, along with a free vascularized fibula and regional latissimus dorsi flaps (Figures 1E&F). Histopathological examination of the humeral tumor indicated vascular invasion. Microscopic examination of the lung tumor displayed features comparable to that observed in the bone, confirming the diagnosis of humeral chondroblastoma-derived lung metastasis (Figure 2C).
After 2 weeks of surgery, the patient developed a postoperative infection, leading to reoperation involving surgical lavage and antibiotic therapy. Perioperative cultures indicated the presence of Cutibacterium acnes and Finegoldia magna. The patient received antibiotic therapy for 3 months.
In addition, the patient experienced postoperative radial nerve palsy, which resolved within 3 months of the surgery. New multiple pulmonary micronodules were detected 4 months following tumor resection. This prompted further investigation through subsequent chest CT imaging.
By March 2022, a rapid progression of previously observed bilateral micronodules, accompanied by the formation of multiple new pulmonary nodules. The patient’s case was presented to and discussed with the French national tumor board, leading to the decision for the patient to undergo systemic treatment with denosumab.
Before initiating denosumab therapy, the patient underwent a dental check-up to ensure satisfactory oral health. In May 2022, the patient commenced denosumab therapy with a loading dose of 120 mg per week for 3 weeks, followed by monthly administrations. Concurrently, the patient received daily calcium (500 mg) and vitamin D (400 IU) supplements, with regular monitoring of calcium levels. Throughout the treatment period, the patient did not experience any adverse effects related to denosumab.
Follow-up and outcomes
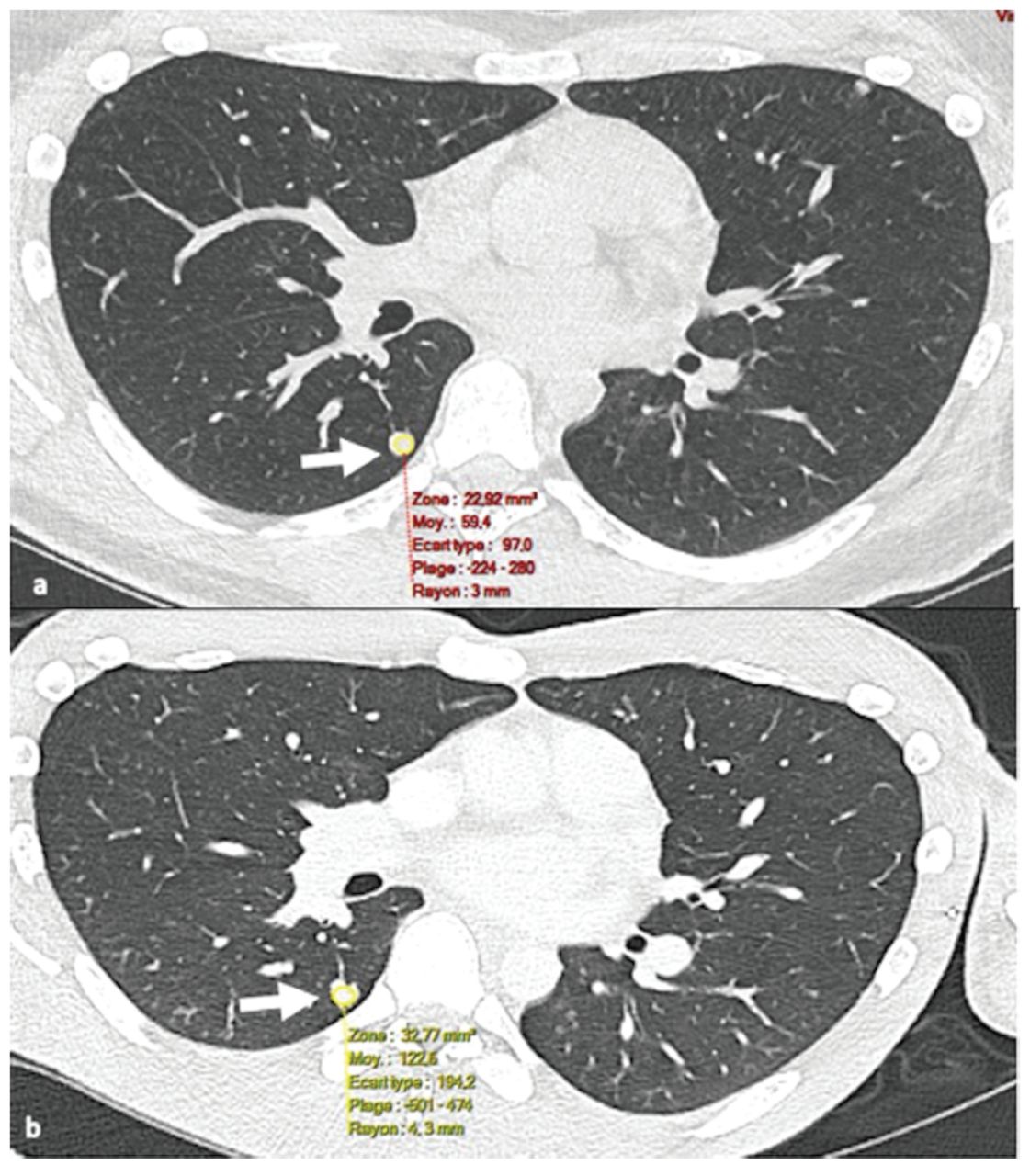
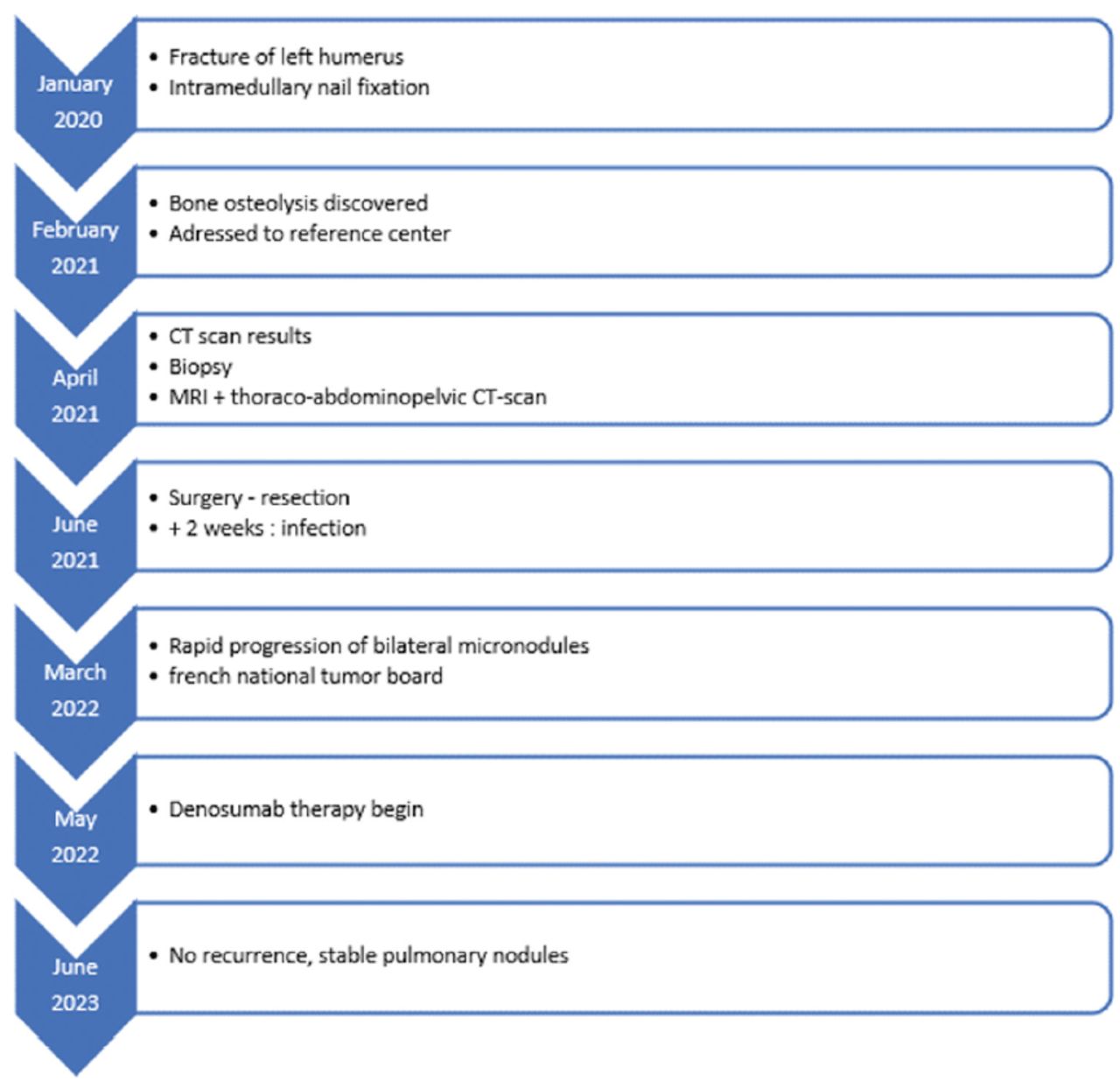
In the most recent follow-up carried out in June 2023 (24 months after surgery and 13 months after denosumab initiation), no signs of local recurrence were observed. A chest CT scan revealed stable pulmonary nodules, which had not progressed after the cessation of denosumab treatment, accompanied by significant calcification (Figure 3). These findings suggested that denosumab therapy was a successful in controlling the disease with a favorable treatment response. The case timeline is summarized in Figure 4.

- Chest computerized tomography (CT) showing changes in the pulmonary metastasis before and after denosumab treatment. a) Chest CT reveals pulmonary metastasis (white arrow) before denosumab treatment (Hounsfield unit: 59.4). b) Chest CT reveals pulmonary metastasis (white arrow) 12 months after the initiation of denosumab treatment (Hounsfield unit: 122.6) indicating calcification.

- Case presentation timeline.
Discussion
Chondroblastoma is a rare benign cartilaginous tumor, accounting for approximately 1% of all bone tumors.1 Despite being considered as a benign lesion, it has a risk of recurrence and exhibits an aggressive local behavior mimicking malignant bone tumors. Moreover, distant metastases may occur throughout clinical follow-ups, with an incidence rate of 1.1-3.3%.2,3,5 This metastases can occur at any age (6-68 years; mean=18.1 years) and are predominantly observed in male gender.6,7 Although the most common primary site for chondroblastoma-derived metastasis is the scapula, pelvis, and ribs, it can also affect the femur, tibia, humerus, spine, fibula, and foot.2 Some authors suggest that chondroblastomas of flat bones may have a higher risk of metastasis.3,5 Approximately 30 cases involving distant metastases have been reported, most commonly involving the lungs; however, involvement of other sites, such as the soft tissue, bone, and viscera, have also been observed.2,5 Metastasis frequently occurs after recurrence, but it can also be observed at the time of initial diagnosis or may even present after many years without recurrence of chondroblastoma.3,4 Survival after metastasis can vary from early death after a few months to prolonged survival.3,5
The correlation between local aggressive behavior and metastasis in chondroblastoma remains unclear. Some cases of metastatic chondroblastomas exhibit a benign radiological aspect, whereas others display an aggressive behavior with soft tissue extensions. Histologically, most studies have not reported any criteria typically associated with malignancies, even when examining metastatic sites.3-5 However, as observed in our case, the risk of metastasis may be associated with the presence of vascular invasion.
Chondroblastoma with associated metastasis has been described only in a few reports, including our case; therefore, no standard treatment is available yet. The previous cases have documented a variety of treatments, including surgical (complete or partial) resection of metastatic lesions, several chemotherapy regimens, radiotherapy, and experimental immunotherapy (with the PD-L1 inhibitor pembrolizumab). These treatments have resulted in varying outcomes, with no definitive consensus on their effectiveness.3,5
Denosumab is a human monoclonal antibody that targets RANKL by blocking the interaction between RANKL and its receptor (RANK) has gained wide acceptance for the treatment of bone GCT. It can be used alone or as a neoadjuvant therapy to facilitate joint-preserving surgery or aid lesion resection by promoting calcification.6,7 It is also effective in treating other bone lesions that features osteoclast-like GCs, including central giant cell granulomas, aneurysmal bone cysts, fibrous dysplasias, and osteoblastomas.7 Chondroblastomas typically contain multinucleated osteoclast-like GCs, and some evidence suggests that these GCs may play a key role in the pathogenesis of chondroblastoma via the RANK/RANKL pathway.1 Huang et al6 demonstrated that RANKL is expressed in chondroblastoma tumor cells and may play a role in the osteolytic bone destruction. Another study demonstrated the expression of RANK, RANKL, and osteoprotegerin in chondroblastomas.7 Using RNA in-situ hybridization, Suster et al8 observed that RANKL RNA is expressed in 92% of the 26 chondroblastoma lesions. Thus, they suggested that denosumab may hold therapeutic potential for the treatment of chondroblastomas.
Despite the existing evidence supporting the efficacy of denosumab in treating various GCT-rich bone lesions and chondroblastomas, its clinical use in treating chondroblastomas has only been noted recently. Three studies have reported the clinical use of denosumab for chondroblastomas. In the first study, Calvert et al9 used denosumab as a local control treatment for recurrent chondroblastoma of the temporal bone. Recently, Visgauss et al10 reported a case of chondroblastoma of the hemipelvis in a 15-year old boy. In this case, denosumab was used as a neoadjuvant treatment for facilitating joint preserving surgery.10 Unfortunately, the patient developed 2 local recurrences and required further surgery. The use of denosumab in metastatic chondroblastoma was reported in only one case by Focaccia et al.4 In their study, denosumab was used to treat lung metastases arising from chondroblastoma of the proximal humerus. Denosumab treatment showed favorable disease stability with reduced pulmonary nodules and nodule calcification.4
Despite evidence of the activity of denosumab against chondroblastoma, it remains unclear whether denosumab treatment is capable of changing the histological aspects of tumors. Only one study has demonstrated the histopathological changes of tumors after denosumab administration. These changes entailed a total absence of osteoclast-like giant cells, alongside a minor augmentation in the chondroid matrix and calcification.10
The unique features of our study included the aggressive local behavior of a chondroblastoma following an unplanned surgery that was treated with intramedullary nail fixation. The presentation of lung metastasis may have resulted from tumor emboli and contamination of the glenohumeral articulation due to the initial surgery and reaming. Furthermore, our case report confirmed the efficacy of denosumab for the treatment of chondroblastoma, aligning with previous reports.
In conclusion, the efficacy of denosumab treatment in controlling the progression of chondroblastoma-derived lung metastasis was clearly evident in our patient. Denosumab should, therefore, be considered for the treatment of metastatic chondroblastoma as it is safer than other previously reported treatment options. This case report confirmed the clinical efficacy of denosumab, in line with previous reports.
Acknowledgment
The authors gratefully acknowledge Dr. Bouilleau Loic for his invaluable contributions to the radiological interpretation in this study. The authors also would like to thank Editage (www.editage.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 24, 2023.
- Accepted April 18, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.